SUMMARY: The FDA on January 19, 2023, approved BRUKINSA® (Zanubrutinib) for Chronic Lymphocytic Leukemia (CLL) or Small Lymphocytic Lymphoma (SLL). The American Cancer Society estimates that for 2023, about 18,740 new cases of Chronic Lymphocytic Leukemia (CLL) will be diagnosed in the US and 4490 patients will die of the disease. CLL accounts for about one-quarter of the new cases of leukemia. The average age of patients diagnosed with CLL is around 70 years, and is rarely seen in people under age 40, and is extremely rare in children.
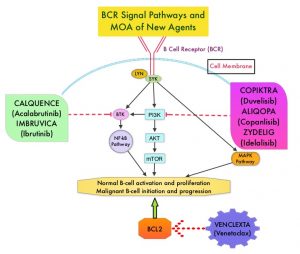
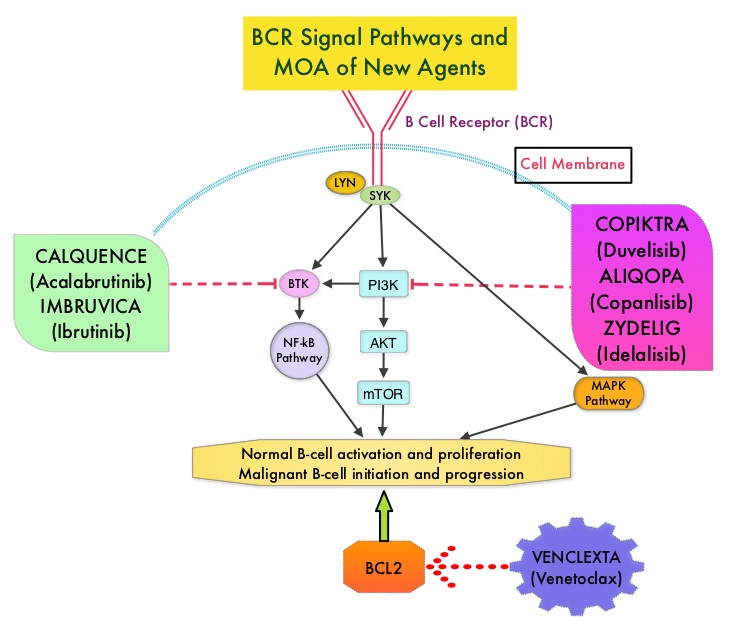
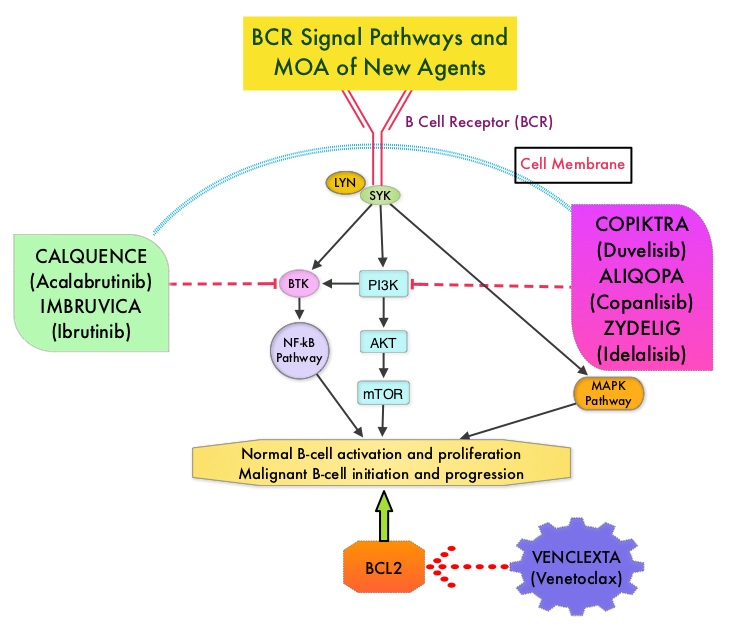
Bruton’s Tyrosine Kinase (BTK) is a member of the Tec family of kinases, downstream of the B-cell receptor and is predominantly expressed in B-cells. It is a mediator of B-cell receptor signaling in normal and transformed B-cells. BTK inhibitors inhibit cell proliferation and promotes programmed cell death (Apoptosis) by blocking B-cell activation and signaling.
Zanubrutinib (BRUKINSA®) is an irreversible, potent, next-generation, small molecule inhibitor of Bruton’s Tyrosine Kinase, designed to deliver targeted and sustained inhibition of the BTK protein by optimizing bioavailability, half-life, and selectivity, while minimizing off-target inhibition of TEC- and EGFR-family kinases. It has been hypothesized that the increased selectivity of BRUKINSA® may minimize toxicities, (such as those often associated with Ibrutinib (IMBRUVICA®) and improve efficacy outcomes. BRUKINSA® demonstrated promising efficacy among patients with CLL/SLL (Small Lymphocytic Lymphoma), in early phase trials.
SEQUOIA is a randomized, multicenter, global Phase III trial, designed to evaluate the efficacy and safety of BRUKINSA® compared to Bendamustine plus Rituximab in patients with treatment naïve CLL or SLL. This trial consists of three cohorts:
Cohort 1 (N=479): Patients NOT harboring del(17p) were randomized 1:1 to receive BRUKINSA® (N=241) or Bendamustine plus Rituximab (N=238) until disease progression or unacceptable toxicity. Patients with del(17p) were not randomized to Bendamustine plus Rituximab, as they experience poor clinical outcomes and poor response to chemoimmunotherapy. Data from this group comprise the Primary endpoint
Cohort 2 (N=110): Patients WITH del(17p) received BRUKINSA® as a monotherapy.
Cohort 3 (enrollment ongoing): Patients WITH del(17p) or pathogenic TP53 variant receiving BRUKINSA® in combination with Venetoclax.
Treatment in Cohort 1 consisted of BRUKINSA® 160 mg orally twice daily as 28-day cycles or Bendamustine 90 mg/m2 IV on Days 1 and 2 for six cycles plus Rituximab 375 mg/m2 IV, the day before or on Day 1 of Cycle 1, and 500 mg/m2 IV on Day 1 of Cycles 2-6. Both treatment groups were well balanced, with more than 50% with unmutated IGHV gene and 18% with del(11q) in each group. Eligible patients had untreated CLL or SLL requiring treatment as per International Workshop on CLL criteria, were 65 years or older, or 18 years or older with comorbidities, WITHOUT del(17p), and had an ECOG PS of 0-2. The Primary endpoint of the SEQUOIA trial was Progression Free Survival (PFS) per Independent Review Committee (IRC) assessment in the randomized Cohort 1 group of patients. Secondary endpoints included Overall Response Rates (ORR), Overall Survival (OS) and Safety.
At the interim analysis, with a median follow-up of 26.2 months, BRUKINSA demonstrated superiority in PFS over Bendamustine plus Rituximab. The median PFS was Not Reached in the BRUKINSA® group and was 33.7 months in the Bendamustine plus Rituximab group. The 24-month PFS rate was 85.5% in the BRUKINSA® group, compared to 69.5% in in the Bendamustine plus Rituximab group (HR=0.42; P<0.0001). This PFS benefit was consistently observed across key patient subgroups, including patients with del(11q), unmutated IGHV status, Binet Stage C, and bulky disease.
In a separate non-randomized group of patients in Cohort 2 of SEQUOIA trial, BRUKINSA® monotherapy was evaluated in 110 patients with previously untreated CLL/SLL, WITH 17p deletion. The Overall Response Rate (ORR) per IRC was 88% and the median Duration of Response (DOR) was not reached after a median follow-up of 25.1 months. The 18-month PFS in this group was 90.6%. Across clinical trials of BRUKINSA® the most common adverse events were neutropenia, upper respiratory tract infection, thrombocytopenia, hemorrhage, and musculoskeletal pain. Atrial fibrillation or flutter were reported in 3.7% of patients.
The researchers from this study concluded that BRUKINSA® significantly improved Progression Free Survival compared to Bendamustine plus Rituximab, in patients with untreated CLL and SLL with an acceptable safety profile, like what has been reported in other BRUKINSA® clinical trials, with consistently low rates of atrial fibrillation. They added that BRUKINSA® as a highly selective BTK inhibitor, can potentially provide a chemo-free treatment option for CLL patients.
Zanubrutinib versus bendamustine and rituximab in untreated chronic lymphocytic leukaemia and small lymphocytic lymphoma (SEQUOIA): a randomised, controlled, phase 3 trial. Tam CS, Brown JR, Kahl BS, et al. The Lancet Oncology 2022;23:1031-1043