
SUMMARY: The American Cancer Society estimates that approximately 14,620 new cases of Chronic Lymphocytic Leukemia (CLL) will be diagnosed in 2015 and approximately 4650 patients will die from the disease. CLL is a disease of the elderly and the average age at the time of diagnosis is 72 years. There are two main types of lymphocytes, B and T lymphocytes/cells. B-cell CLL is the most common type of leukemia in adults. Normal B-cell activation and proliferation is dependent on B-cell receptor (BCR) signaling. This signaling is also important for initiation and progression of B-cell lymphoproliferative disorders. Bruton’s Tyrosine Kinase (BTK) is a member of the Tec family of kinases, downstream of the B-cell receptor and is predominantly expressed in B-cells. It is a mediator of B-cell receptor signaling in normal and transformed B-cells. Following binding of antigen to the B-Cell Receptor, kinases such as Syk (Spleen Tyrosine Kinase), Lyn (member of the Src family of protein tyrosine kinases) and BTK (Bruton’s Tyrosine Kinase) are activated, with subsequent propagation through PI3K/Akt, MAPK, and NF-κB pathways. This results in B-cell activation and proliferation. IMBRUVICA® (Ibrutinib) is an oral, irreversible inhibitor of BTK and inhibits cell proliferation and promotes programmed cell death (Apoptosis) by blocking B-cell activation and signaling. The FDA initially granted accelerated approval to IMBRUVICA® in February 2014 for previously treated patients with CLL and this was followed by full FDA approval and a new treatment indication for high-risk CLL patients with 17p deletions, in July 2014. Previously published studies had shown significant Response Rates and and Event-Free Survival with BR (Bendamustine-TREANDA® and Rituximab-RITUXAN®) in FLUDARA® (Fludarabine) refractory patients, with Chronic Lymphocytic Leukemia.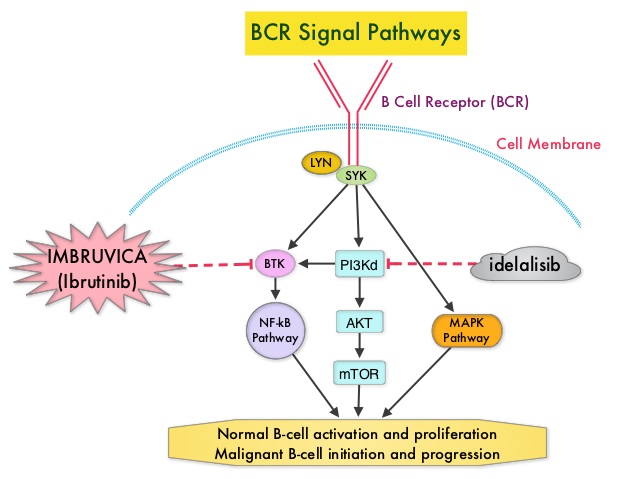
The HELIOS study is a double-blind, randomized, phase III trial which evaluated the benefit of combining IMBRUVICA® with BR compared to placebo plus BR, in patients with previously treated, relapsed/refractory Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. In this study, of the 578 randomized patients, 289 patients received a maximum of six cycles of BR with IMBRUVICA® 420 mg PO daily and 289 patients received BR with placebo. The median patient age was 64 years, patients had received a median of two prior therapies and 38% of the patients had Rai Stage III/IV disease. Patients with 17p deletions in more than >20% of cells, were excluded. The planned six cycles of BR were completed by 83% in the IMBRUVICA® group and 78% in the placebo group. The primary endpoint was Progression Free Survival (PFS). Secondary endpoints included Overall Survival (OS) and Overall Response Rate (ORR). Following an interim analysis, this study was unblinded as there was a significant PFS benefit with IMBRUVICA® and patients receiving placebo, were allowed to cross over to the IMBRUVICA® group, per study protocol,. Thirty one percent (31%) of the patients in the BR plus placebo group with confirmed progressive disease crossed over to receive BR plus IMBRUVICA®. At a median follow up of 17.2 months, the PFS in the IMBRUVICA® plus BR group was not yet reached whereas the PFS was 13.3 months for patients receiving placebo plus BR (HR=0.203; P<0.0001). This PFS benefit was seen across subgroups of high-risk patients as well. The ORR was 82.7% in the IMBRUVICA® plus BR group compared to 67.8% in the placebo plus BR group (P <0.0001). Complete Response (CR) rates which included CR with incomplete blood count recovery were 10.4% versus 2.8% with IMBRUVICA® and placebo, respectively. The median OS was not reached. The incidence of most adverse events were comparable between the two treatment groups and the most frequent side effects were neutropenia affecting about 55% of the patients and nausea experienced by about 35% of the patients. The authors concluded that IMBRUVICA® plus BR resulted in an 80% reduction in the risk of disease progression, as well as improved Overall Response Rates, compared to placebo plus BR. This triplet combination of IMBRUVICA®, TREANDA® and RITUXAN® should therefore be considered an important treatment option for patients with previously treated Chronic Lymphocytic Leukemia and Small Lymphocytic Lymphoma. Ibrutinib combined with bendamustine and rituximab (BR) in previously treated chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL): first results from a randomized, double-blind, placebo-controlled, phase III study. Chanan-Khan AAA, Cramer P, Demirkan F, et al. J Clin Oncol. 2015;33 (suppl; abstr LBA7005).
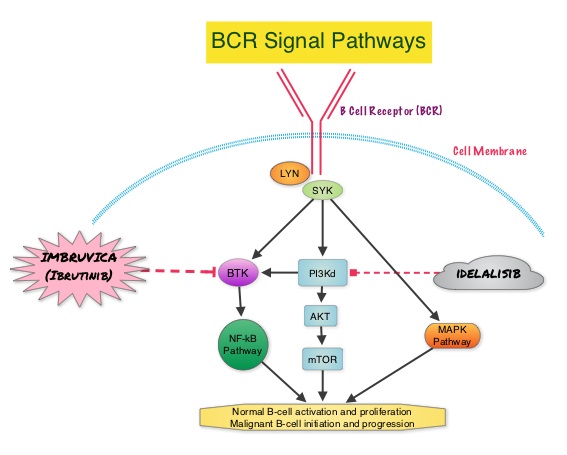 This signaling is also important for initiation and progression of B-cell lymphoproliferative disorders. Bruton’s tyrosine kinase (BTK) is a member of the Tec family of kinases, downstream of the B-cell receptor and is predominantly expressed in B-cells. It is a mediator of B-cell receptor signaling in normal and transformed B-cells. Following binding of antigen to the BCR, Syk (Spleen Tyrosine Kinase), Lyn (member of the Src family of protein tyrosine kinases) and BTK (Bruton’s Tyrosine Kinase) are activated, with subsequent propagation through PI3K/Akt, MAPK, and NF-κB pathways and resulting B-cell activation and proliferation. IMBRUVICA® (Ibrutinib) is an oral, irreversible inhibitor of BTK and inhibits cell proliferation and promotes programmed cell death (Apoptosis). The RESONATE trial is a multicenter, randomized, open-label Phase III study in which single agent IMBRUVICA® was compared to single agent ARZERRA® (Ofatumumab) in patients with relapsed or refractory CLL or Small Lymphocytic Lymphoma (SLL). In this study, 391 patients who had measurable nodal disease and received at least one prior therapy, were randomized to receive 420 mg of IMBRUVICA® orally once daily until progression (N=195) or ARZERRA® at an initial dose of 300 mg followed by 11 doses at 2000 mg, given intravenously weekly (N=196). Patients randomized to the ARZERRA® group, on disease progression were allowed to receive treatment with IMBRUVICA®. The median age was 67 years, 40% of the patients enrolled in the study were 70 years of age or over and 30% of patients had deletion of chromosome 17p. The primary endpoint of this study was Progression-Free Survival (PFS) and the secondary endpoints included Overall Survival (OS), Overall Response rate (ORR) and safety. Following recommendations from the Independent Data Monitoring Committee (IDMC), the study was stopped earlier, as the primary endpoint as well as an important secondary endpoint of the study, were met. At a median follow up of 9.4 months, IMBRUVICA® significantly prolonged PFS compared to ARZERRA® (median not reached vs 8.1 months; HR 0.215, P<0.0001) with a 78.5% reduction in the risk of disease progression and also significantly improved OS (median not reached, HR 0.43, P=0.0049) when compared with ARZERRA®, with a 57% reduction in the risk of death. The Overall Response Rates were significantly higher in the IMBRUVICA® group compared to the ARZERRA® group (42.6% vs 4.1% (P <0 .0001). An additional 20% of patients treated with IMBRUVICA® had a partial response of their persistent lymphocytosis. The benefit with IMBRUVICA® was similarly high even in the two very high risk groups of patients such as those with 17p deletions and those refractory to purine analog chemoimmunotherapy. The overall survival was significant despite the crossover of 57 patients upon progression, from the ARZERRA® group to IMBRUVICA®. Treatment was well tolerated in both groups. Diarrhea, fatigue, nausea and atrial fibrillation were more frequent in the IMBRUVICA® group but did not result in frequent dose reductions or treatment discontinuation. The authors concluded that IMBRUVICA® significantly improved Progression Free Survival, Overall Survival and Overall Response Rates, in patients with relapsed/refractory CLL/SLL, compared with ARZERRA® and IMBRUVICA® should also be a consideration for elderly patients who often are unable to tolerate intensive chemotherapy. Byrd JC, Brown JR, O’Brien SM, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA7008)
This signaling is also important for initiation and progression of B-cell lymphoproliferative disorders. Bruton’s tyrosine kinase (BTK) is a member of the Tec family of kinases, downstream of the B-cell receptor and is predominantly expressed in B-cells. It is a mediator of B-cell receptor signaling in normal and transformed B-cells. Following binding of antigen to the BCR, Syk (Spleen Tyrosine Kinase), Lyn (member of the Src family of protein tyrosine kinases) and BTK (Bruton’s Tyrosine Kinase) are activated, with subsequent propagation through PI3K/Akt, MAPK, and NF-κB pathways and resulting B-cell activation and proliferation. IMBRUVICA® (Ibrutinib) is an oral, irreversible inhibitor of BTK and inhibits cell proliferation and promotes programmed cell death (Apoptosis). The RESONATE trial is a multicenter, randomized, open-label Phase III study in which single agent IMBRUVICA® was compared to single agent ARZERRA® (Ofatumumab) in patients with relapsed or refractory CLL or Small Lymphocytic Lymphoma (SLL). In this study, 391 patients who had measurable nodal disease and received at least one prior therapy, were randomized to receive 420 mg of IMBRUVICA® orally once daily until progression (N=195) or ARZERRA® at an initial dose of 300 mg followed by 11 doses at 2000 mg, given intravenously weekly (N=196). Patients randomized to the ARZERRA® group, on disease progression were allowed to receive treatment with IMBRUVICA®. The median age was 67 years, 40% of the patients enrolled in the study were 70 years of age or over and 30% of patients had deletion of chromosome 17p. The primary endpoint of this study was Progression-Free Survival (PFS) and the secondary endpoints included Overall Survival (OS), Overall Response rate (ORR) and safety. Following recommendations from the Independent Data Monitoring Committee (IDMC), the study was stopped earlier, as the primary endpoint as well as an important secondary endpoint of the study, were met. At a median follow up of 9.4 months, IMBRUVICA® significantly prolonged PFS compared to ARZERRA® (median not reached vs 8.1 months; HR 0.215, P<0.0001) with a 78.5% reduction in the risk of disease progression and also significantly improved OS (median not reached, HR 0.43, P=0.0049) when compared with ARZERRA®, with a 57% reduction in the risk of death. The Overall Response Rates were significantly higher in the IMBRUVICA® group compared to the ARZERRA® group (42.6% vs 4.1% (P <0 .0001). An additional 20% of patients treated with IMBRUVICA® had a partial response of their persistent lymphocytosis. The benefit with IMBRUVICA® was similarly high even in the two very high risk groups of patients such as those with 17p deletions and those refractory to purine analog chemoimmunotherapy. The overall survival was significant despite the crossover of 57 patients upon progression, from the ARZERRA® group to IMBRUVICA®. Treatment was well tolerated in both groups. Diarrhea, fatigue, nausea and atrial fibrillation were more frequent in the IMBRUVICA® group but did not result in frequent dose reductions or treatment discontinuation. The authors concluded that IMBRUVICA® significantly improved Progression Free Survival, Overall Survival and Overall Response Rates, in patients with relapsed/refractory CLL/SLL, compared with ARZERRA® and IMBRUVICA® should also be a consideration for elderly patients who often are unable to tolerate intensive chemotherapy. Byrd JC, Brown JR, O’Brien SM, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA7008)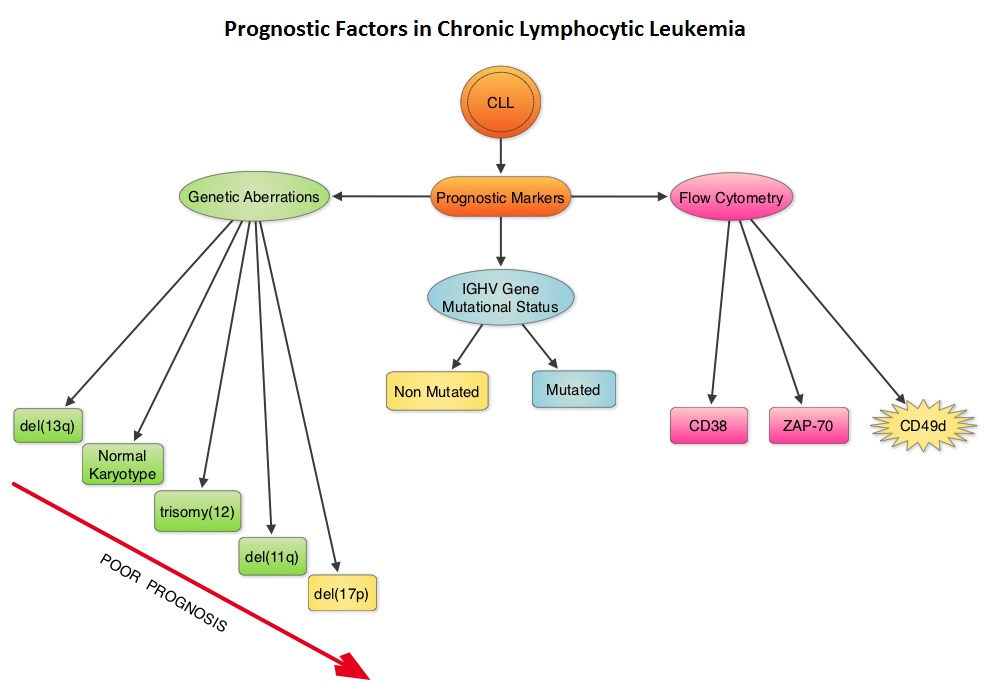 Retrospective studies have suggested that patients with CLL whose leukemic cells have clonotypically rearranged immunoglobulin genes in germline configuration (Unmutated IGHV gene) demonstrated more aggressive disease and shorter survival time compared to those patients with somatic hypermutations in their IGHV genes (Mutated IGHV gene). Expression of two flow cytometry based biomarkers, CD38 (surface marker) and ZAP-70 (intracytoplasmic protein), have been associated with poor outcomes. As we learn more about the pathobiology of CLL, it is becoming clear that survival of CLL cells is dependent not only on their intracellular defects but also on the microenvironment. CD49d, an integrin, is a surface molecule, detected by flow cytometry. CD49d expression promotes microenvironment mediated proliferation of CLL cells and has been associated with shortened survival. The authors conducted this multicenter analysis to evaluate the prognostic utility of CD49d in CLL, in comparison with CD38 and ZAP-70. The authors analysed the data of 2972 patients from 9 clinical trials. All these studies had data on CD49d expression of CLL cells by flow cytometry and reported the association between CD49d expression and Overall survival and/or Treatment Free Survival and/or Progression Free Survival. Patients with 30% or more of CLL cells expressing CD49d were considered CD49d positive. In this pooled analysis, CD49d positive patients had a significantly lower Overall Survival both at 5 years (87% vs 94%) and 10 years (62% vs 84%) compared with CD49d negative patients (P<0.001). Further, CD49d positive patients more likely required treatment, suggesting that these patients had a lower probability of remaining treatment free at both 5 years (42% vs 68%) and 10 years (24% vs 50%), compared with CD49d negative patients. When other variables were taken into consideration, CD49d was the only flow cytometry based marker which independently predicted Overall Survival with greater prognostic relevance than CD38 and ZAP-70. The authors concluded that CD49d expression and IGHV gene mutational status may be the strongest predictors of Overall Survival and Treatment Free Survival in patients with CLL and should be a part of routine baseline testing at the time of diagnosis. Bulian P, Shanafelt TD, Fegan C, et al. J Clin Oncol 2014;32:897-904
Retrospective studies have suggested that patients with CLL whose leukemic cells have clonotypically rearranged immunoglobulin genes in germline configuration (Unmutated IGHV gene) demonstrated more aggressive disease and shorter survival time compared to those patients with somatic hypermutations in their IGHV genes (Mutated IGHV gene). Expression of two flow cytometry based biomarkers, CD38 (surface marker) and ZAP-70 (intracytoplasmic protein), have been associated with poor outcomes. As we learn more about the pathobiology of CLL, it is becoming clear that survival of CLL cells is dependent not only on their intracellular defects but also on the microenvironment. CD49d, an integrin, is a surface molecule, detected by flow cytometry. CD49d expression promotes microenvironment mediated proliferation of CLL cells and has been associated with shortened survival. The authors conducted this multicenter analysis to evaluate the prognostic utility of CD49d in CLL, in comparison with CD38 and ZAP-70. The authors analysed the data of 2972 patients from 9 clinical trials. All these studies had data on CD49d expression of CLL cells by flow cytometry and reported the association between CD49d expression and Overall survival and/or Treatment Free Survival and/or Progression Free Survival. Patients with 30% or more of CLL cells expressing CD49d were considered CD49d positive. In this pooled analysis, CD49d positive patients had a significantly lower Overall Survival both at 5 years (87% vs 94%) and 10 years (62% vs 84%) compared with CD49d negative patients (P<0.001). Further, CD49d positive patients more likely required treatment, suggesting that these patients had a lower probability of remaining treatment free at both 5 years (42% vs 68%) and 10 years (24% vs 50%), compared with CD49d negative patients. When other variables were taken into consideration, CD49d was the only flow cytometry based marker which independently predicted Overall Survival with greater prognostic relevance than CD38 and ZAP-70. The authors concluded that CD49d expression and IGHV gene mutational status may be the strongest predictors of Overall Survival and Treatment Free Survival in patients with CLL and should be a part of routine baseline testing at the time of diagnosis. Bulian P, Shanafelt TD, Fegan C, et al. J Clin Oncol 2014;32:897-904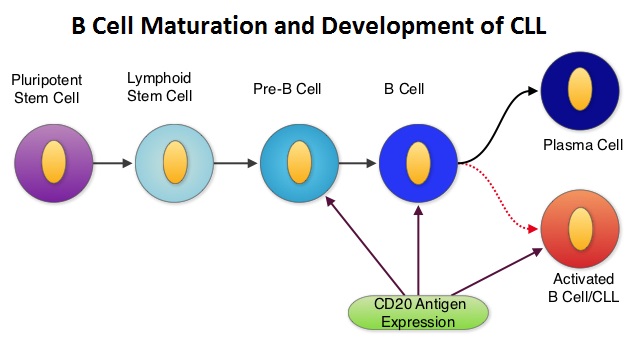 Monoclonal antibodies targeting CD20 destroy CD20 positive B cells by 3 different mechanisms. They include Antibody Dependent Cellular Cytotoxicity (ADCC), Complement Dependent Cytotoxicity (CDC) and programmed cell death (Apoptosis).
Monoclonal antibodies targeting CD20 destroy CD20 positive B cells by 3 different mechanisms. They include Antibody Dependent Cellular Cytotoxicity (ADCC), Complement Dependent Cytotoxicity (CDC) and programmed cell death (Apoptosis).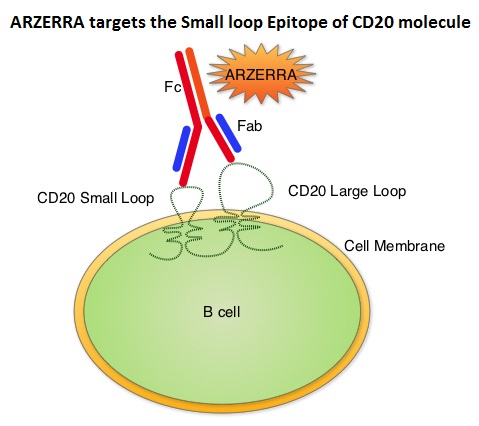 Unlike RITUXAN®, ARZERRA® targets the Small loop epitope of CD20 molecule which is proximal to the B cell membrane and this has been shown to be associated with highly efficient cell lysis through complement dependent cytotoxicity. So, compared to RITUXAN®. ARZERRA® has stronger CDC, similar ADCC and does not appear to induce Apoptosis. In this study, 447 CLL patients for whom FLUDARA® based therapy was considered to be inappropriate due to age and comorbidities, were randomly assigned 1:1 to receive either ARZERRA® in combination with LEUKERAN® or LEUKERAN® alone. ARZERRA® was given as an IV infusion at a dose of 300 mg on Cycle 1, Day 1, 1000 mg on Cycle 1, Day 8 and 1000 mg administered on Day 1 of all subsequent 28 day cycles. LEUKERAN® was given at a dose of 10 mg/m2 orally on Days 1 to 7 every 28 days in both treatment groups. The median age was 69 years and majority of the patients had 2 or more comorbidities. The primary endpoint of this study was Progression Free Survival (PFS) and secondary endpoints included Overall Response Rate (ORR), Overall Survival (OS) and safety. The median number of cycles in both treatment groups was 6. The median PFS was 22.4 months for patients receiving ARZERRA® in combination with LEUKERAN® compared with 13.1 months for those receiving single agent LEUKERAN® (HR=0.57, P< 0.001). The ORR was higher with the combination regimen versus single agent LEUKERAN® (82% vs 69%, P=0.001) and 37% of patients in the combination arm were MRD negative. The median OS for the combination group was not reached. The majority of adverse reactions were Grade 2 or lower, in both of the treatment arms and included infusion reactions, neutropenia, asthenia, headache, herpes simplex, lower respiratory tract infections, arthralgia and upper abdominal pain. The authors concluded that ARZERRA® in combination with LEUKERAN® is a clinically important milestone, in the management of elderly patients with CLL, who are considered inappropriate for FLUDARA® based therapy. Hillmen P, Robak T, Janssens A, et al. Blood 2013;122: Abstract#528
Unlike RITUXAN®, ARZERRA® targets the Small loop epitope of CD20 molecule which is proximal to the B cell membrane and this has been shown to be associated with highly efficient cell lysis through complement dependent cytotoxicity. So, compared to RITUXAN®. ARZERRA® has stronger CDC, similar ADCC and does not appear to induce Apoptosis. In this study, 447 CLL patients for whom FLUDARA® based therapy was considered to be inappropriate due to age and comorbidities, were randomly assigned 1:1 to receive either ARZERRA® in combination with LEUKERAN® or LEUKERAN® alone. ARZERRA® was given as an IV infusion at a dose of 300 mg on Cycle 1, Day 1, 1000 mg on Cycle 1, Day 8 and 1000 mg administered on Day 1 of all subsequent 28 day cycles. LEUKERAN® was given at a dose of 10 mg/m2 orally on Days 1 to 7 every 28 days in both treatment groups. The median age was 69 years and majority of the patients had 2 or more comorbidities. The primary endpoint of this study was Progression Free Survival (PFS) and secondary endpoints included Overall Response Rate (ORR), Overall Survival (OS) and safety. The median number of cycles in both treatment groups was 6. The median PFS was 22.4 months for patients receiving ARZERRA® in combination with LEUKERAN® compared with 13.1 months for those receiving single agent LEUKERAN® (HR=0.57, P< 0.001). The ORR was higher with the combination regimen versus single agent LEUKERAN® (82% vs 69%, P=0.001) and 37% of patients in the combination arm were MRD negative. The median OS for the combination group was not reached. The majority of adverse reactions were Grade 2 or lower, in both of the treatment arms and included infusion reactions, neutropenia, asthenia, headache, herpes simplex, lower respiratory tract infections, arthralgia and upper abdominal pain. The authors concluded that ARZERRA® in combination with LEUKERAN® is a clinically important milestone, in the management of elderly patients with CLL, who are considered inappropriate for FLUDARA® based therapy. Hillmen P, Robak T, Janssens A, et al. Blood 2013;122: Abstract#528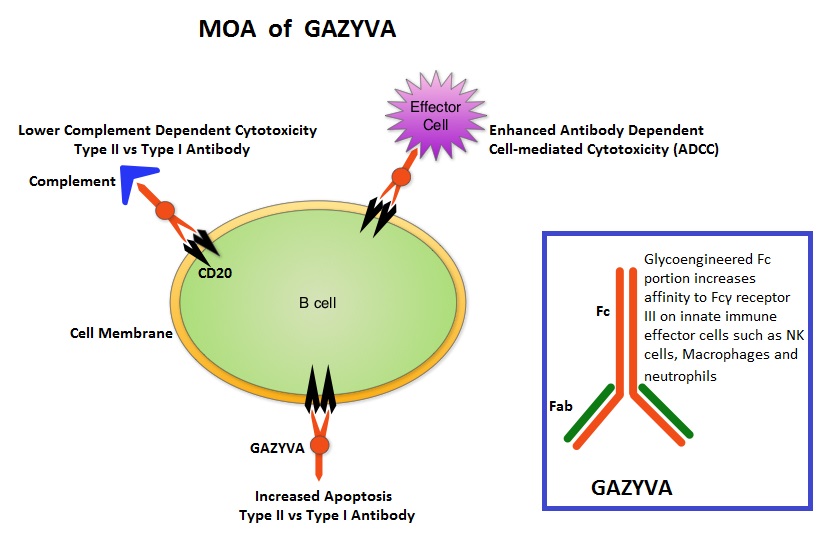 GAZYVA® is glycoengineered, fully humanized, third generation, type II anti-CD20 antibody (IgG1 monoclonal antibody) that selectivity binds to the extracellular domain of the CD20 antigen on malignant human B cells. By virtue of binding affinity of the glycoengineered Fc portion of GAZYVA® to Fcγ receptor III on innate immune effector cells such as natural killer cells, macrophages and neutrophils, antibody-dependent cell-mediated cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis is significantly enhanced, whereas it induces very little complement-dependent cytotoxicity. This is in contrast to RITUXAN® (Rituximab), which is a first generation type I, chimeric anti-CD20 targeted monoclonal antibody that kills CLL cells primarily by complement-dependent cytotoxicity and also ADCC. In this phase III trial, LEUKERAN® (Chlorambucil) was compared with a combination of GAZYVA® plus LEUKERAN® and a combination of RITUXAN® plus LEUKERAN®. Five Hundred and eighty nine (589) treatment naïve CLL patients over 70 years of age with comorbidities were enrolled of whom 118 patients received LEUKERAN® alone, 238 received GAZYVA® plus LEUKERAN® and 233 received RITUXAN® plus LEUKERAN®. The primary endpoint was Progression-Free Survival (PFS). Chemoimmunotherapy with both GAZYVA® plus LEUKERAN® and RITUXAN® plus LEUKERAN® significantly prolonged PFS compared to LEUKERAN® alone. The median PFS was 11.1 months with LEUKERAN® alone compared to 26.7 months for GAZYVA® plus LEUKERAN® (HR=0.18, P<0.001) and 16.3 months for RITUXAN® plus LEUKERAN® (HR=0.44, P<0.001). This benefit was seen in all subgroups except those with del(17) and quality of life in those who received antibody along with LEUKERAN® was not compromised. The combination of GAZYVA® and LEUKERAN®, also prolonged overall survival when compared to LEUKERAN® alone (HR=0.41; P=0.002). This benefit however was not noted with the RITUXAN® plus LEUKERAN® combination. Treatment with GAZYVA® plus LEUKERAN® when compared with RITUXAN® plus LEUKERAN®, resulted in a longer PFS (26.7 vs15.2 months; HR=0.39; P<0.001), higher complete response rates (20.7% vs. 7.0%) and deeper molecular responses. Infusion related reactions were more common in the GAZYVA® plus LEUKERAN® group without increase in the risk for infections. The authors concluded that a combination of GAZYVA® and LEUKERAN® when given to elderly patients with comorbid conditions improved overall survival compared to LEUKERAN® alone and resulted in higher response rates and longer PFS than RITUXAN® plus LEUKERAN®. Goede V, Fischer K, Busch R, et al. N Engl J Med 2014; 370:1101-1110
GAZYVA® is glycoengineered, fully humanized, third generation, type II anti-CD20 antibody (IgG1 monoclonal antibody) that selectivity binds to the extracellular domain of the CD20 antigen on malignant human B cells. By virtue of binding affinity of the glycoengineered Fc portion of GAZYVA® to Fcγ receptor III on innate immune effector cells such as natural killer cells, macrophages and neutrophils, antibody-dependent cell-mediated cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis is significantly enhanced, whereas it induces very little complement-dependent cytotoxicity. This is in contrast to RITUXAN® (Rituximab), which is a first generation type I, chimeric anti-CD20 targeted monoclonal antibody that kills CLL cells primarily by complement-dependent cytotoxicity and also ADCC. In this phase III trial, LEUKERAN® (Chlorambucil) was compared with a combination of GAZYVA® plus LEUKERAN® and a combination of RITUXAN® plus LEUKERAN®. Five Hundred and eighty nine (589) treatment naïve CLL patients over 70 years of age with comorbidities were enrolled of whom 118 patients received LEUKERAN® alone, 238 received GAZYVA® plus LEUKERAN® and 233 received RITUXAN® plus LEUKERAN®. The primary endpoint was Progression-Free Survival (PFS). Chemoimmunotherapy with both GAZYVA® plus LEUKERAN® and RITUXAN® plus LEUKERAN® significantly prolonged PFS compared to LEUKERAN® alone. The median PFS was 11.1 months with LEUKERAN® alone compared to 26.7 months for GAZYVA® plus LEUKERAN® (HR=0.18, P<0.001) and 16.3 months for RITUXAN® plus LEUKERAN® (HR=0.44, P<0.001). This benefit was seen in all subgroups except those with del(17) and quality of life in those who received antibody along with LEUKERAN® was not compromised. The combination of GAZYVA® and LEUKERAN®, also prolonged overall survival when compared to LEUKERAN® alone (HR=0.41; P=0.002). This benefit however was not noted with the RITUXAN® plus LEUKERAN® combination. Treatment with GAZYVA® plus LEUKERAN® when compared with RITUXAN® plus LEUKERAN®, resulted in a longer PFS (26.7 vs15.2 months; HR=0.39; P<0.001), higher complete response rates (20.7% vs. 7.0%) and deeper molecular responses. Infusion related reactions were more common in the GAZYVA® plus LEUKERAN® group without increase in the risk for infections. The authors concluded that a combination of GAZYVA® and LEUKERAN® when given to elderly patients with comorbid conditions improved overall survival compared to LEUKERAN® alone and resulted in higher response rates and longer PFS than RITUXAN® plus LEUKERAN®. Goede V, Fischer K, Busch R, et al. N Engl J Med 2014; 370:1101-1110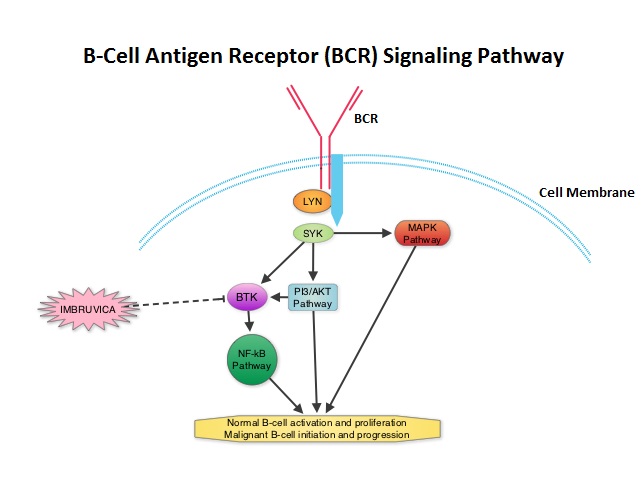 The FDA granted accelerated approval of IMBRUVICA® for the treatment of patients with Chronic Lymphocytic Leukemia (CLL) who had received at least one prior therapy. This approval was based on the outcomes in a select group of 48 patients who were a part of a larger group of 85 patients, enrolled in a multicenter single arm phase Ib/II trial. The median age was 67 years and 71% were male. Patients had a median number of 4 prior treatments and had an ECOG PS of 0-1. Patients in this group received IMBRUVICA® 420 mg PO daily until disease progression or unacceptable toxicity. The overall response rate was 58.3% as assessed by an independent review committee. No complete responses were seen and the response duration ranged from 5.6 to over 24 months. This analysis did not include data from those patients enrolled in the trial who received IMBRUVICA® 840 mg PO daily or those with Small Lymphocytic Lymphoma (N=37). The most common toxicities included fatigue, myalgias and arthralgias, cytopenias, nausea, diarrhea, fever and rash. Transient asymptomatic increase in lymphocyte count with resolution of lymphadenopathy and splenomegaly was common but resolved with continued treatment. The confirmatory RESONATE trial is a multicenter, randomized, open-label Phase III study in which single agent IMBRUVICA® was compared to single agent ARZERRA® (Ofatumumab) in patients with relapsed or refractory CLL or Small Lymphocytic Lymphoma . This was a part of the requirement by the FDA. Enrolled patients had measurable nodal disease and were not eligible for treatment with purine analog-based therapy. In this study, 391 patients who had received at least one prior therapy, were enrolled and randomized to receive 420 mg of IMBRUVICA® orally once daily or ARZERRA® given intravenously. Treatment was given over a period of 24 weeks until disease progression or unacceptable toxicity. Patients randomized to the ARZERRA® group on disease progression were allowed to receive treatment with IMBRUVICA®. The primary endpoint of this study was progression-free survival and the secondary endpoint was overall survival. Following recommendations from the Independent Data Monitoring Committee (IDMC), the study was stopped earlier, as the primary endpoint as well as an important secondary endpoint of the study were met. At the planned interim analysis, patients in the IMBRUVICA® group showed a statistically significant improvement in progression-free survival, the primary endpoint of the study as well as a statistically significant improvement in overall survival, the secondary endpoint of the trial. This data confirmed the efficacy of IMBRUVICA® and gives patients with CLL, an important new treatment option. Byrd JC, Furman RR, Coutre SE, et al. N Engl J Med 2013; 369:32-42
The FDA granted accelerated approval of IMBRUVICA® for the treatment of patients with Chronic Lymphocytic Leukemia (CLL) who had received at least one prior therapy. This approval was based on the outcomes in a select group of 48 patients who were a part of a larger group of 85 patients, enrolled in a multicenter single arm phase Ib/II trial. The median age was 67 years and 71% were male. Patients had a median number of 4 prior treatments and had an ECOG PS of 0-1. Patients in this group received IMBRUVICA® 420 mg PO daily until disease progression or unacceptable toxicity. The overall response rate was 58.3% as assessed by an independent review committee. No complete responses were seen and the response duration ranged from 5.6 to over 24 months. This analysis did not include data from those patients enrolled in the trial who received IMBRUVICA® 840 mg PO daily or those with Small Lymphocytic Lymphoma (N=37). The most common toxicities included fatigue, myalgias and arthralgias, cytopenias, nausea, diarrhea, fever and rash. Transient asymptomatic increase in lymphocyte count with resolution of lymphadenopathy and splenomegaly was common but resolved with continued treatment. The confirmatory RESONATE trial is a multicenter, randomized, open-label Phase III study in which single agent IMBRUVICA® was compared to single agent ARZERRA® (Ofatumumab) in patients with relapsed or refractory CLL or Small Lymphocytic Lymphoma . This was a part of the requirement by the FDA. Enrolled patients had measurable nodal disease and were not eligible for treatment with purine analog-based therapy. In this study, 391 patients who had received at least one prior therapy, were enrolled and randomized to receive 420 mg of IMBRUVICA® orally once daily or ARZERRA® given intravenously. Treatment was given over a period of 24 weeks until disease progression or unacceptable toxicity. Patients randomized to the ARZERRA® group on disease progression were allowed to receive treatment with IMBRUVICA®. The primary endpoint of this study was progression-free survival and the secondary endpoint was overall survival. Following recommendations from the Independent Data Monitoring Committee (IDMC), the study was stopped earlier, as the primary endpoint as well as an important secondary endpoint of the study were met. At the planned interim analysis, patients in the IMBRUVICA® group showed a statistically significant improvement in progression-free survival, the primary endpoint of the study as well as a statistically significant improvement in overall survival, the secondary endpoint of the trial. This data confirmed the efficacy of IMBRUVICA® and gives patients with CLL, an important new treatment option. Byrd JC, Furman RR, Coutre SE, et al. N Engl J Med 2013; 369:32-42