
SUMMARY: The American Cancer Society’s estimates that for 2015, approximately 74,000 new melanomas will be diagnosed in the United States and about 10,000 people are expected to die of the disease. The incidence of melanoma has been on the rise for the past 30 years. The US Food and Drug Administration approved YERVOY® (Ipilimumab) for the treatment of unresectable or metastatic melanoma in March 2011. This therapy was the first, to improve Overall Survival in a phase III trial. YERVOY® is a fully human immunoglobulin G1 monoclonal antibody, that blocks Immune checkpoint protein/receptor CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), and this is the first Immune checkpoint protein that was clinically targeted.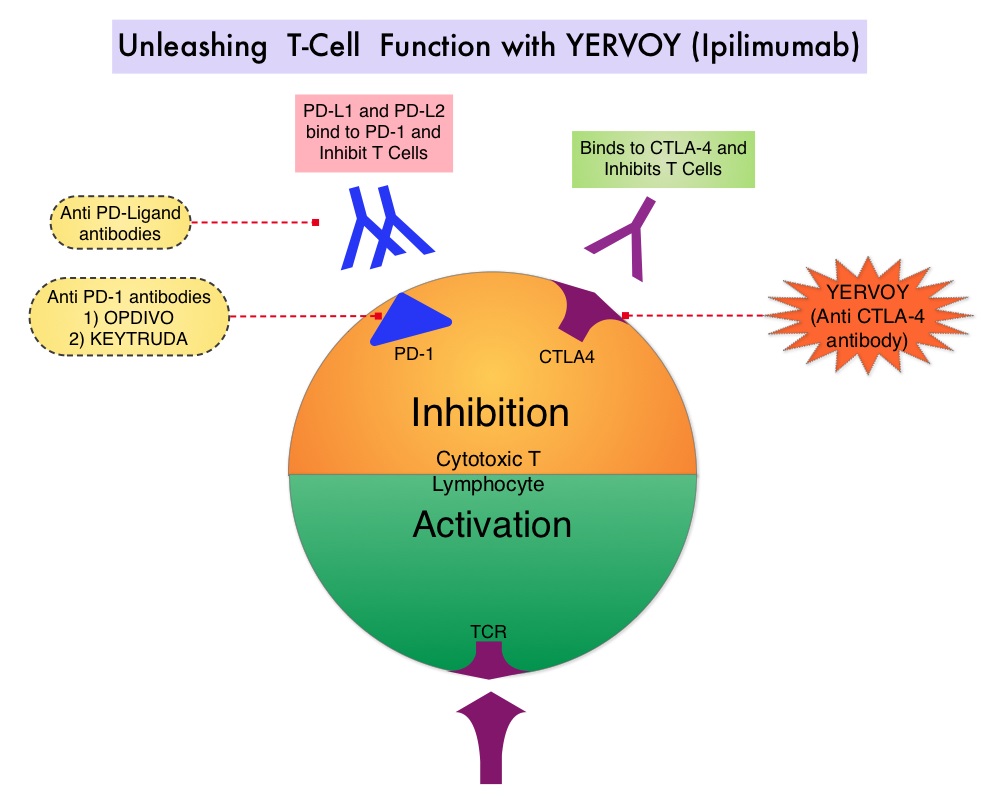 Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4, also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. CA184-024 is a phase III trial in which treatment naïve patients with stage IIIc, N3 (unresectable), or stage IV melanoma were randomly assigned to receive YERVOY® 10 mg/kg IV given along with Dacarbazine 850 mg/m2 IV (N=250) or placebo plus Dacarbazine 850 mg/m2 IV (N=252) administered every 3 weeks for 4 doses followed by Dacarbazine given alone every 3 weeks through week 22. Responders and those with stable disease from week 12 through week 24 were then allowed to receive YERVOY® or placebo as maintenance therapy given every 12 weeks beginning at week 24, until disease progression or unacceptable toxicity. Dacarbazine was not given during the maintenance phase. The median Overall Survival was significantly longer in the group treated with YERVOY® plus Dacarbazine than in patients treated with placebo plus Dacarbazine (11.2 vs 9.1 months, HR=0.72; P< 0.001). This Overall Survival benefit was maintained after 3 years of follow up and toxicities were manageable.
Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4, also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. CA184-024 is a phase III trial in which treatment naïve patients with stage IIIc, N3 (unresectable), or stage IV melanoma were randomly assigned to receive YERVOY® 10 mg/kg IV given along with Dacarbazine 850 mg/m2 IV (N=250) or placebo plus Dacarbazine 850 mg/m2 IV (N=252) administered every 3 weeks for 4 doses followed by Dacarbazine given alone every 3 weeks through week 22. Responders and those with stable disease from week 12 through week 24 were then allowed to receive YERVOY® or placebo as maintenance therapy given every 12 weeks beginning at week 24, until disease progression or unacceptable toxicity. Dacarbazine was not given during the maintenance phase. The median Overall Survival was significantly longer in the group treated with YERVOY® plus Dacarbazine than in patients treated with placebo plus Dacarbazine (11.2 vs 9.1 months, HR=0.72; P< 0.001). This Overall Survival benefit was maintained after 3 years of follow up and toxicities were manageable.
The authors in this publication conducted a milestone survival analysis with a minimum follow-up of 5 years and they noted that the 5-year survival rate doubled and was 18.2% for patients treated with YERVOY® plus Dacarbazine versus 8.8% for patients treated with placebo plus Dacarbazine (P=0.002). The plateau in the survival curve began at approximately 3 years. In patients who survived at least 5 years and continued maintenance YERVOY®, grade 3 or 4 immune-related adverse events were observed exclusively in the skin. Based on these findings, it was concluded that patients treated with YERVOY® for advanced melanoma, continue to respond following a period of stable disease and these ongoing and durable responses may contribute to long term survival in some patients. Five-Year Survival Rates for Treatment-Naive Patients With Advanced Melanoma Who Received Ipilimumab Plus Dacarbazine in a Phase III Trial. Maio M, Grob J, Aamdal S, et al. J Clin Oncol 2015;33: 1191-1196
Bottom Ad

Advertisement