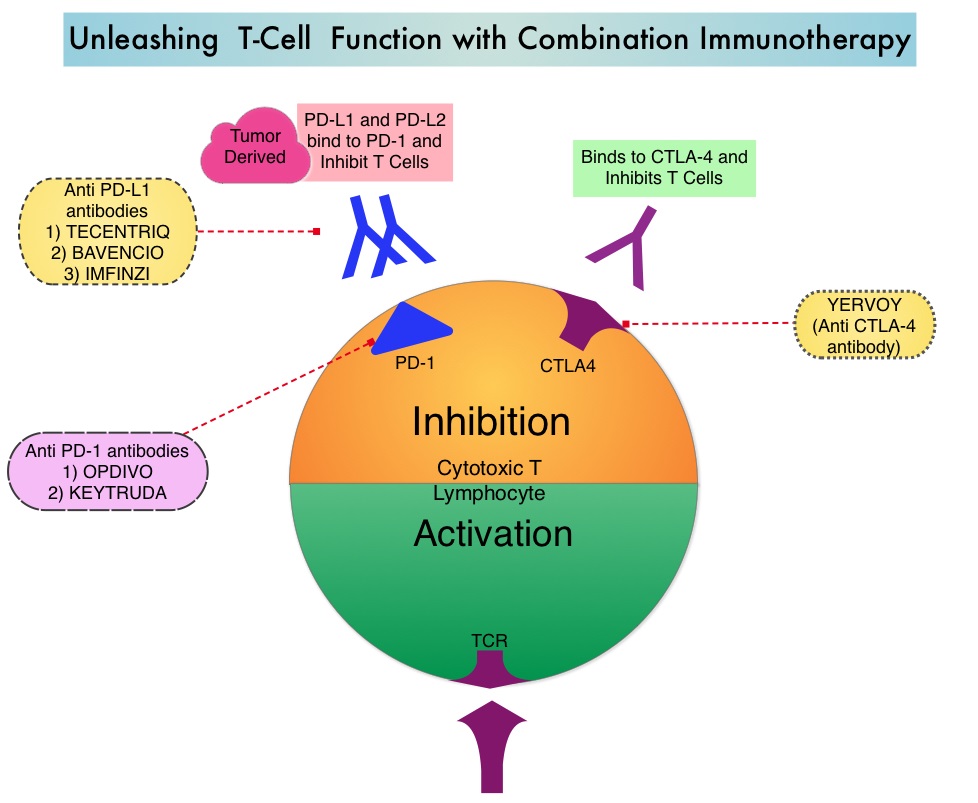
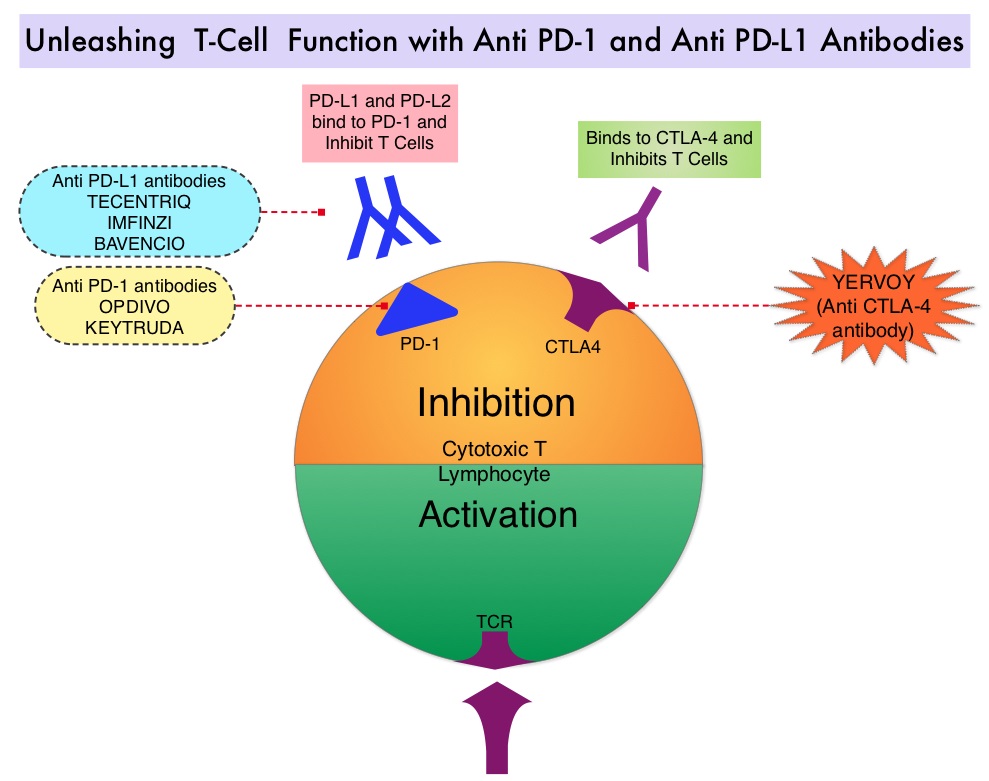
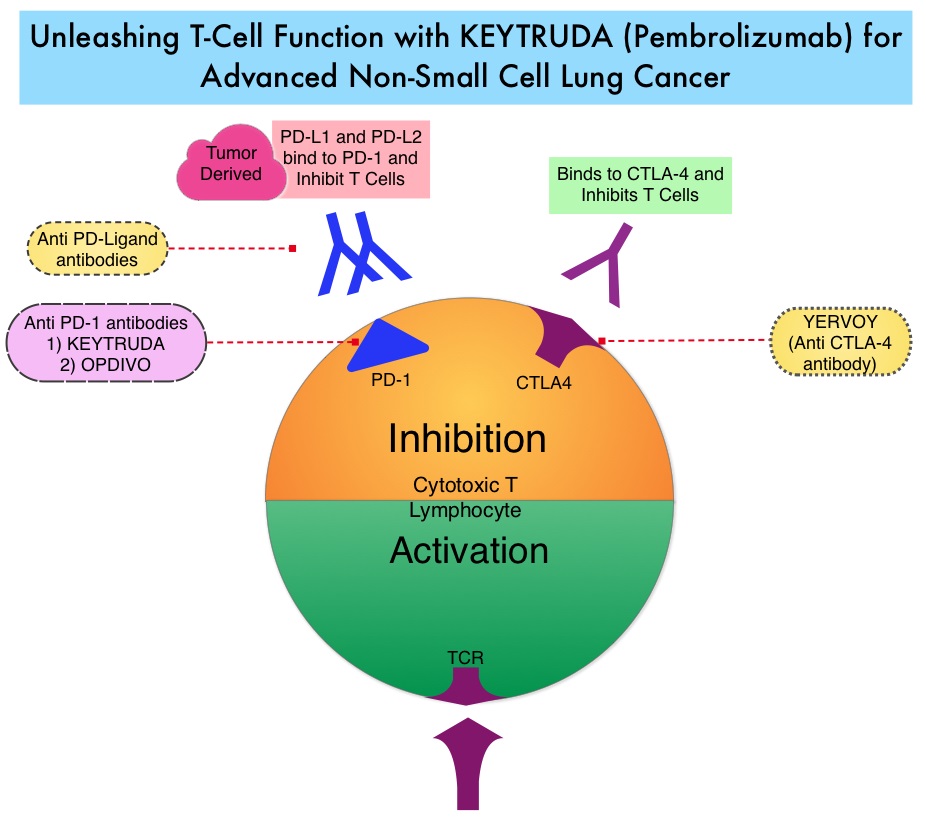
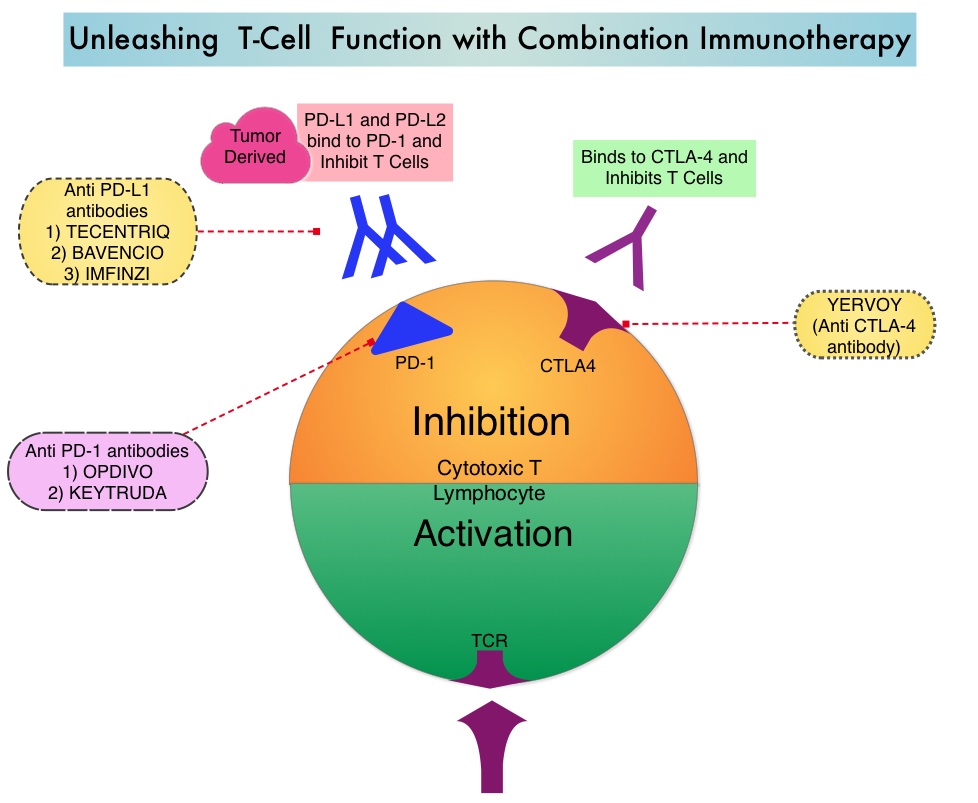
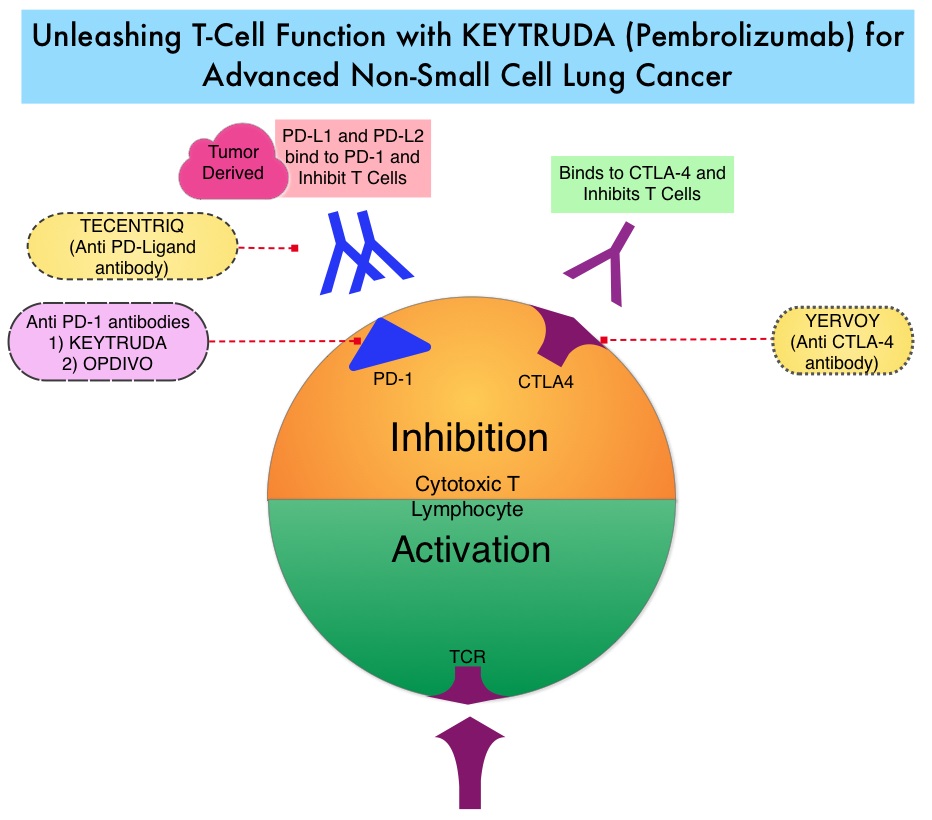
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2018 about 234,030 new cases of lung cancer will be diagnosed and over 154,050 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Immunotherapy with PD-1 (Programmed cell Death 1) and PD-L1 (Programmed cell Death Ligand 1) inhibitors have demonstrated a clear survival benefit both as a single agent or in combination, compared with standard chemotherapy, in both treatment-naive and previously treated patients for advanced Non Small Cell Lung Cancer (NSCLC). Immuno-Oncology therapies unleash the T cells by blocking the Immune checkpoint proteins, thereby resulting in T cell proliferation, activation and a therapeutic response.
Recent reports of an acceleration of tumor growth during immunotherapy, defined as HyperProgressive Disease (HPD), has been observed in 9% of advanced malignancies and in 29% of patients with Head and Neck cancer treated with PD-1/PD-L1 inhibitors. It has been postulated that high level of interferon gamma (IFN-gamma) usually released by PD-1 blockade may have detrimental effects on immunity. Alternatively PD-1/PD-L1 blockade may upregulate Interleukin 6, Interleukin 17, and neutrophil axis, generating a potent aberrant inflammation, responsible for immune escape and accelerated growth.
HyperProgressive Disease should be differentiated from Pseudoprogression. The later is defined as progressive disease, followed by Complete Response and/or Partial Response or Stable Disease longer than 6 months. The Tumor Growth Rate (TGR) estimates the increase in tumor volume over time based on two Computed Tomography (CT) scan measurements. TGR can be used to quantitatively assess tumor dynamics and kinetics during treatment and can be specifically applied to identify the subset of patients experiencing HPD.
This study was conducted to investigate whether HPD is observed in patients with advanced NSCLC treated with PD-1/PD-L1 inhibitors compared with single-agent chemotherapy and whether there is an association between treatment and HPD. This multicenter, retrospective study included 406 consecutive eligible patients with confirmed Stage III or IV NSCLC treated with PD-1/PD-L1 inhibitors such as OPDIVO® (Nivolumab), KEYTRUDA® (Pembrolizumab), TECENTRIQ® (Atezolizumab), or IMFINZI® (Durvalumab) as monotherapy in second or later line treatment, at eight French institutions between November 2012 and April 2017. The control cohort included equivalent data collected on 59 eligible patients with advanced NSCLC, who had failed a Platinum-based regimen and received single-agent chemotherapy (Taxanes, Pemetrexed, Vinorelbine , or Gemcitabine) in 4 French institutions from August 2011, to June 2016. The median age was 50 years, over 70% of the patients had nonsquamous histology and approximately 20% of the patients had PD-L1 positive status (1% or more by IHC) confirmed. The median followup was 12.1 months. Measurable disease (defined by Response Evaluation Criteria in Solid Tumors – RECIST version 1.1) on at least two CT scans before treatment and one CT scan during treatment, was required. HyperProgressive Disease (HPD) was defined as disease progression on the first CT scan during treatment with an absolute increase in Tumor Growth Rate exceeding 50%. The Primary end point was assessment of the HyperProgressive Disease rate in patients treated with Immunotherapy or chemotherapy.
Among those treated with PD-1/PD-L1 inhibitors, HyperProgressive Disease was noted in 13.8% of patients. HPD was significantly associated with more than two metastatic sites prior to treatment with PD-1/PD-L1 inhibitors, compared with those without HPD (62.5% versus 42.6%; P=0.006). However, baseline tumor burden and number of previous lines of therapy did not make a significant difference. Patients experiencing HPD within the first 6 weeks of beginning PD-1/PD-L1 inhibitor therapy had significantly lower median Overall Survival compared with those with progressive disease without HyperProgression at the first evaluation (3.4 months versus 6.2 months; HR=2.18; P=0.003). Pseudoprogression was observed in 4.7% patients.
Among patients treated with single-agent chemotherapy, only 5.1% were classified as having HyperProgressive Disease and the median Overall Survival was 4.5 months in those with HPD and 3.9 months in other patients with progressive disease without HyperProgression at the first evaluation (P=0.60).
The authors concluded that HyperProgressive Disease is more common with PD-1/PD-L1 inhibitors compared with chemotherapy, among previously treated patients with advanced NSCLC, and is also associated with high number of metastatic sites at baseline and poor survival. They added that the present study is the largest analysis exploring HPD to date and is the first conducted, in a dedicated NSCLC population, with a control cohort of chemotherapy-treated patients Hyperprogressive Disease in Patients With Advanced Non–Small Cell Lung Cancer Treated With PD-1/PD-L1 Inhibitors or With Single-Agent Chemotherapy. Ferrara R, Mezquita L, Texier M, et al. JAMA Oncol. Published online September 6, 2018. doi:10.1001/jamaoncol.2018.3676