SUMMARY: The FDA on Sept. 14, 2017 approved MVASI® (Bevacizumab-awwb) as a Biosimilar to AVASTIN® (Bevacizumab). Bevacizumab is a recombinant immunoglobulin G1 (IgG1) monoclonal antibody (mAb) that binds to Vascular Endothelial Growth Factor (VEGF) and inhibits the interaction of VEGF with its receptors, VEGF receptor-1 and VEGF receptor-2. This in turn inhibits establishment of new blood vessels that are essential for the maintenance and growth of solid tumors. MVASI® is the first Biosimilar approved in the U.S. for the treatment of cancer. A Biosimilar product is a biological product that is approved based on its high similarity to an already approved biological product (also known as reference product). Biological products are made from living organisms including humans, animals and microorganisms such as bacteria or yeast, and are manufactured through biotechnology, derived from natural sources or produced synthetically. Biological products have larger molecules with a complex structure, than conventional drugs (also known as small molecule drugs).
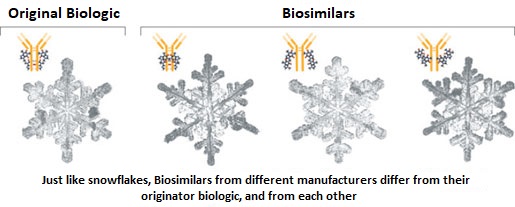 Unlike biological products, conventional drugs are made of pure chemical substances and their structures can be identified. A generic drug is a copy of brand name drug and has the same active ingredient and is the same as brand name drug in dosage form, safety and strength, route of administration, quality, performance characteristics and intended use. Therefore, brand name and the generic drugs are bioequivalent. The Affordable Care Act in 2010 created an abbreviated licensure pathway for biological products that are demonstrated to be “Biosimilar” to, or “interchangeable” with an FDA approved biological product (reference product). The Biosimilar must show that it has no clinically meaningful differences in terms of safety and effectiveness from the reference product. A Biosimilar product can only be approved by the FDA if it has the same mechanism of action, route of administration, dosage form and strength as the reference product, and only for the indications and conditions of use that have been approved for the reference product. Biosimilars are not as easy to manufacture as generics (copies of brand name drugs), because of the complexity of the structure of the biologic product and the process used to make a biologic product. The facilities where Biosimilars are manufactured must also meet the FDA standards.
Unlike biological products, conventional drugs are made of pure chemical substances and their structures can be identified. A generic drug is a copy of brand name drug and has the same active ingredient and is the same as brand name drug in dosage form, safety and strength, route of administration, quality, performance characteristics and intended use. Therefore, brand name and the generic drugs are bioequivalent. The Affordable Care Act in 2010 created an abbreviated licensure pathway for biological products that are demonstrated to be “Biosimilar” to, or “interchangeable” with an FDA approved biological product (reference product). The Biosimilar must show that it has no clinically meaningful differences in terms of safety and effectiveness from the reference product. A Biosimilar product can only be approved by the FDA if it has the same mechanism of action, route of administration, dosage form and strength as the reference product, and only for the indications and conditions of use that have been approved for the reference product. Biosimilars are not as easy to manufacture as generics (copies of brand name drugs), because of the complexity of the structure of the biologic product and the process used to make a biologic product. The facilities where Biosimilars are manufactured must also meet the FDA standards.
MVASI® is approved for the treatment of patients with the following cancers:
• Metastatic Colorectal cancer, in combination with intravenous 5-Fluorouracil-based chemotherapy for first or second line treatment. MVASI® is not indicated for the adjuvant treatment of surgically resected Colorectal cancer.
• Metastatic Colorectal cancer, in combination with Fluoropyrimidine-Irinotecan or Fluoropyrmidine-Oxaliplatin-based chemotherapy for the second line treatment of patients who have progressed on a first-line Bevacizumab containing regimen.
• Non-squamous Non Small Cell Lung Cancer, in combination with Carboplatin and Paclitaxel for first line treatment of unresectable, locally advanced, recurrent or metastatic disease.
• Glioblastoma with progressive disease following prior therapy, based on improvement in Objective Response Rate. No data is available demonstrating improvement in disease-related symptoms or survival with Bevacizumab.
• Metastatic Renal cell carcinoma, in combination with Interferon alfa.
• Cervical cancer that is persistent, recurrent, or metastatic disease, in combination with Paclitaxel and Cisplatin or Paclitaxel and Topotecan.
The approval of MVASI® was based on two studies. In the first study, PharmacoKinetics (PK) of biosimilar MVASI® was compared with Bevacizumab, following a single infusion of 3 mg/kg. It was concluded that the PK data was similar between the Biosimilar, MVASI® and Bevacizumab. The second study is a randomized, double-blind, phase III trial, that evaluated the efficacy and safety of MVASI®, compared with Bevacizumab, in patients with non-squamous Non Small Cell Lung Cancer (NSCLC). Patients with non-squamous NSCLC, on first line chemotherapy with Carboplatin and TAXOL® (Paclitaxel), were randomized in a 1:1 ratio to receive either MVASI® (N=328) or Bevacizumab 15 mg/kg (N=314), as an IV infusion, every 3 weeks, for 6 cycles. The Objective Response Rate (ORR) was similar between the two treatment groups (39.0% for MVASI® and 41.7% for Bevacizumab) and these results were not statistically different. The Duration of Response was similar. Adverse events were comparable in the two treatment groups. This study demonstrated that MVASI® was clinically similar to Bevacizumab.
The FDA concluded that the approval of MVASI® was based on comparisons of extensive structural and functional product characterization, animal data, human PharmacoKinetic and pharmacodynamic data, clinical immunogenicity, between MVASI® and AVASTIN® (Bevacizumab), and it was noted that MVASI® is highly similar to AVASTIN® and that there are no clinically meaningful differences between the two products. Randomized, double-blind, phase 3 study evaluating efficacy and safety of ABP 215 compared with bevacizumab in patients with non-squamous NSCLC. Thatcher N, Thomas M, Paz-Ares L, et al. DOI: 10.1200/JCO.2016.34.15_suppl.9095 Journal of Clinical Oncology 34, no. 15_suppl (May 2016) 9095-9095.