
The FDA on May 28, 2019 approved REVLIMID® in combination with a RITUXAN® (Rituximab) for previously treated Follicular Lymphoma (FL) and previously treated Marginal Zone Lymphoma (MZL). REVLIMID® is a product of Celgene Corp.
Tag: Non-Hodgkin Lymphoma
ASH 2018 Four Cycles of Chemotherapy Equally Effective as Six Cycles in Diffuse Large B-Cell Lymphoma
SUMMARY: The American Cancer Society estimates that in 2019, about 74,200 people will be diagnosed with Non Hodgkin Lymphoma (NHL) in the United States and about 19,970 individuals will die of this disease. Diffuse Large B-Cell Lymphoma (DLBCL) is the most common of the aggressive Non-Hodgkin lymphoma’s in the United States, and the incidence has steadily increased 3-4% each year. More than half of patients are 65 or older at the time of diagnosis and the incidence is likely to increase with the aging of the American population. The etiology of Diffuse Large B-Cell Lymphoma is unknown. Contributing risk factors include immunosuppression (AIDS, transplantation setting, autoimmune diseases), UltraViolet radiation, pesticides, hair dyes, and diet. DLBCL is a neoplasm of large B cells and the most common chromosome abnormality involves alterations of the BCL-6 gene at the 3q27 locus, which is critical for germinal center formation. Two major molecular subtypes of DLBCL arising from different genetic mechanisms have been identified, using gene expression profiling: Germinal Center B-cell-like (GCB) and Activated B-Cell-like (ABC). Patients in the GCB subgroup have a higher five year survival rate, independent of clinical IPI (International Prognostic Index) risk score, whereas patients in the ABC subgroup have a significantly worse outcome. Regardless, R-CHOP regimen (RITUXAN®-Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone), given every 21 days, for 6 cycles, delivered with curative intent, is the current standard of care for patients of all ages, with newly diagnosed DLBCL, regardless of molecular subtype. The MInT trial (MabThera International Trial Group) published in The Lancet Oncology in 2006 established that for a subgroup of young DLBCL patients with favorable prognosis (age-adjusted International Prognostic Index (aaIPI) of 0 and no bulky disease, 6 cycles CHOP-like chemotherapy plus RITUXAN® resulted in a 3-year Event Free Survival of 89%, Progression Free Survival of 95% and Overall Survival of 98% (Lancet Oncol 2006;7:379-391).
The International Prognostic Index includes the following risk factors and one point is assigned to each risk factor (Age greater than 60 years, ECOG PS of 2, 3 or 4, elevated serum LDH, more than one Extranodal site and Stages III or IV disease). Age-Adjusted IPI is a simplified version and can be used when comparing patients within an age group (i.e. 60 years or younger, or over 60 years) and includes only 3 of the above factors (Performance Status, LDH and Stage).
Treatment with CHOP-like chemotherapy can result in delayed toxicities including cardiotoxicity and second malignancies. De-escalating chemotherapy can reduce toxicities and cost, while improving patient convenience. The authors conducted the FLYER trial to evaluate whether a shorter chemotherapy course of 4 cycles of R-CHOP plus 2 cycles of RITUXAN® alone was non-inferior to the standard treatment of 6 cycles of R-CHOP.
The FLYER trial is an international, multicenter, randomized phase III study in which 592 treatment naïve patients with favorable risk (age 18-60 years, tumor size less than 7.5 cm), Stage I or II DLBCL, were randomly assigned to receive either 6 cycles of R-CHOP, or 4 cycles of R-CHOP plus 2 cycles of RITUXAN®. For this final analysis, 588 patients were evaluable. Each treatment cycle was 21 days. Radiotherapy was not part of the planned treatment, with the exception of prophylactic radiotherapy of the contralateral testis, in patients with Testicular lymphoma. Both treatment groups were well balanced. The mean age was 48 years, 99% were classified as IPI = 0 and 1% as IPI = 1. The Primary endpoint was Progression Free Survival (PFS).
At a median follow up of 66 months, there was no significant difference in the PFS between the two treatment groups (P=0.76). The 3-year Progression Free Survival (PFS) rate was 94% for patients who received 6 cycles of R-CHOP (N=295) compared with 96% for those who received 4 cycles of R-CHOP followed by 2 cycles of RITUXAN® (N=293). The 3-year Overall Survival (OS) rate was 98% among those who received 6 cycles of R-CHOP versus 99% for those who received 4 cycles of R-CHOP followed by 2 cycles of RITUXAN® (P=0.89). There was also no significant difference in the Relapse Rate between the two treatment groups (4-5%). Grade 3 and 4 nonhematologic as well as hematologic Adverse Events were higher in those patients who received 6 cycles of R-CHOP versus the 4 cycles of R-CHOP.
The authors concluded that in this randomized, noninferiority, phase III study, 2 fewer cycles of R-CHOP greatly reduced toxicity without compromising efficacy, in young treatment naïve patients, with low-risk Diffuse Large B-Cell Lymphoma. Data on outcomes in the Germinal Center B-cell-like (GCB) versus Activated B-Cell-like (ABC) subsets is not available. Excellent outcome of young patients (18-60 years) with favourable-prognosis diffuse large B-cell lymphoma (DLBCL) treated with 4 cycles CHOP plus 6 applications of rituximab: results of the 592 patients of the FLYER trial of the Dshnhl/GLA. Poeschel V, Held G, Ziepert M, et al. Presented at ASH Annual Meeting and Exposition: December 4-8, 2018; San Diego, California. Abstract 781.
TRUXIMA® (Rituximab-abbs)
The FDA on November 28, 2018 approved TRUXIMA® as the first biosimilar to RITUXAN® (Rituximab) for patients with CD20-positive, B-cell non-Hodgkin’s lymphoma (NHL), to be used as a single agent or in combination with chemotherapy. TRUXIMA® is a product of Celltrion Inc.
ADCETRIS® (Brentuximab vedotin)
The FDA on November 16, 2018 approved ADCETRIS® in combination with chemotherapy for previously untreated systemic Anaplastic Large Cell Lymphoma or other CD30-expressing Peripheral T-Cell Lymphomas. ADCETRIS® is a product of Seattle Genetics Inc.
Circulating Tumor DNA (Liquid Biopsy) Can Predict Outcomes in Diffuse Large B-Cell Lymphoma
SUMMARY: The American Cancer Society estimates that in 2018, about 74,680 people will be diagnosed with Non Hodgkin Lymphoma (NHL) in the United States and about 19,910 individuals will die of this disease. Diffuse Large B-Cell Lymphoma (DLBCL) is the most common of the aggressive Non-Hodgkin lymphoma’s in the United States, and the incidence has steadily increased 3-4% each year. More than half of patients are 65 or older at the time of diagnosis and the incidence is likely to increase with the aging of the American population. The etiology of Diffuse Large B-Cell Lymphoma is unknown. Contributing risk factors include immunosuppression (AIDS, transplantation setting, autoimmune diseases), UltraViolet radiation, pesticides, hair dyes, and diet. DLBCL is a neoplasm of large B cells and the most common chromosome abnormality involves alterations of the BCL-6 gene at the 3q27 locus, which is critical for germinal center formation. Two major molecular subtypes of DLBCL arising from different genetic mechanisms have been identified, using gene expression profiling: Germinal Center B-cell-like (GCB) and Activated B-Cell-like (ABC). Patients in the GCB subgroup have a higher five year survival rate, independent of clinical IPI (International Prognostic Index) risk score, whereas patients in the ABC subgroup have a significantly worse outcome. Regardless, R-CHOP regimen (RITUXAN®-Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone), given every 21 days, for 6 cycles, delivered with curative intent, is the current standard of care for patients of all ages, with newly diagnosed DLBCL, regardless of molecular subtype.
Approximately 30-40% of patients experience disease progression or relapse, during the first 2 years and it is important to be able to predict which patients will need more aggressive intervention earlier. Circulating tumor DNA (ctDNA) is being increasingly used as a biomarker across various tumor types and the researchers have previously shown that ctDNA levels can predict tumor recurrence weeks or months before clinical symptoms arise, in patients with lung cancer.
The use of International Prognostic Index (IPI) and interim Positron Emission Tomography (PET) to select patients for intensified therapy, has failed to improve Overall Survival in patients with DLBCL. Several recent studies have suggested that for patients with DLBCL, the addition of pretreatment tumor genomic information to the established clinical prognostic tools such as the International Prognostic Index (IPI) score and interim positron emission tomography (PET) may greatly improve risk stratification. However, the association between the use of this risk stratification to select patients for more aggressive therapy and improvement in outcomes has remained unclear.
The authors in this study evaluated whether dynamic and serial measurements of circulating tumor DNA (ctDNA) from plasma of DLBCL patients had additional prognostic value for predicting patient outcomes, before and during therapy of Diffuse Large B-Cell Lymphoma, as the existing methods are unable to consistently predict treatment failure, given the heterogeneity of DLBCL.
The researchers measured ctDNA from 217 patients with DLBCL or Primary Mediastinal B-cell Lymphoma at six centers in the US and Europe using CAPP-Seq (Cancer Personalized Profiling by deep sequencing ) methodology and compared levels of ctDNA before treatment with levels after the first and second cycles of conventional chemotherapy for each patient. CAPP-Seq is a form of targeted deep next-generation sequencing invented by these authors. They applied deep sequencing of genes for mutational genotyping and tracking of mutations before and during therapy for predicting Event Free Survival (EFS) at 24 months as well as Overall Survival (OS). Using this method, 99% of patients had at least one tumor-specific alteration detected for monitoring, and 98% had ctDNA prior to therapy. Further, the researchers also assessed the prognostic value of ctDNA in the context of established risk factors, including the International Prognostic Index and interim Positron Emission Tomography/Computed Tomography scans.
It was noted that Pretreatment ctDNA levels were prognostic in both the frontline and the relapsed setting. A two-log (i.e., 100-fold) decrease in ctDNA between pretreatment samples and end of cycle 1 of therapy (Early Molecular Response-EMR) or a 2.5-log drop in ctDNA between pretreatment samples and end of cycle 3 of therapy (Major Molecular Response-MMR) was associated with a substantially higher likelihood of cure, independent of the IPI score, in the multivariate analysis. Early Molecular Response and Major Molecular Response were concordant in 92% of patients in whom both were evaluable.
The 24-month Event Free Survival among patients receiving frontline therapy who experienced an Early Molecular Response was 83% vs. 50% (P=0.0015) and for those who experienced a Major Molecular Response was 82% vs. 46% (P<0.001). Early Molecular Response also predicted superior 24-month EFS among patients receiving salvage therapy (100% vs. 13%; P =0.011).
The molecular responses as defined by the drop in ctDNA levels, when correlated with established risk factors such as IPI and interim PET/CT scans, remained prognostic for EFS and OS in patients with low or high IPI, as well as in the context of interim PET/CT. It was noted that patients with favorable results for both molecular response and interim PET had excellent outcomes, whereas those with a combination of a positive interim PET scan and no molecular response were at extremely high risk for treatment failure.
It was concluded that pretreatment ctDNA levels and molecular responses are independently prognostic of outcomes in DLBCL. ctDNA could be used as a risk stratification tool and those who do not have a rapid drop in the ctDNA levels ( within 21 days after the initiation of treatment) may be candidates for more aggressive or novel therapies. More importantly standardization of the available assays for molecular monitoring in DLBCL will be necessary. Circulating Tumor DNA Measurements As Early Outcome Predictors in Diffuse Large B-Cell Lymphoma. Kurtz DM, Scherer F, Jin MC, et al. J Clin Oncol. 2018 Oct 1;36(28):2845-2853. doi: 10.1200/JCO.2018.78.5246. Epub 2018 Aug 20.
COPIKTRA® (Duvelisib)
The FDA on September 24, 2018 granted regular approval to COPIKTRA® for adult patients with Relapsed or Refractory Chronic Lymphocytic Leukemia (CLL) or Small Lymphocytic Llymphoma (SLL) after at least two prior therapies. In addition, COPIKTRA® received accelerated approval for adult patients with Relapsed or Refractory Follicular Lymphoma (FL) after at least two prior systemic therapies. COPIKTRA® is a product of Verastem, Inc.
REVLIMID® plus RITUXAN®, A Potential Chemo-Free Frontline Therapy for Follicular Lymphoma
SUMMARY: The American Cancer Society estimates that in 2018, about 74,680 people will be diagnosed with Non Hodgkin Lymphoma (NHL) in the United States and about 19,910 individuals will die of this disease. Indolent Non Hodgkin Lymphomas are mature B cell lymphoproliferative disorders and include Follicular Lymphoma, Nodal Marginal Zone Lymphoma (NMZL), Extranodal Marginal Zone Lymphoma (ENMZL) of Mucosa-Associated Lymphoid Tissue (MALT), Splenic Marginal Zone Lymphoma (SMZL), LymphoPlasmacytic Lymphoma (LPL) and Small Lymphocytic Lymphoma (SLL).
Follicular Lymphoma is the most indolent form and second most common form of all NHLs and they are a heterogeneous group of lymphoproliferative malignancies. Approximately 20% of all NHLs are Follicular Lymphomas. Advanced stage indolent NHL is not curable and as such, prolonging Progression Free Survival (PFS) and Overall Survival (OS), while maintaining Quality of Life, have been the goals of treatment intervention. Asymptomatic patients with indolent NHL are generally considered candidates for “watch and wait” approach. Patients with advanced stage symptomatic Follicular Lymphoma are often treated with induction chemoimmunotherapy followed by maintenance RITUXAN® (Rituximab).
REVLIMID® (Lenalidomide) is an oral immunomodulatory agent (IMiD) with activity in lymphoid malignancies, primarily through immune modulation (repair T-cell immune synapse dysfunction and Natural Killer cell/T-cell effector augmentation). It additionally has antiproliferative effects. Chemo-free combination immunotherapy with REVLIMID® and RITUXAN® or the R2 regimen, has shown promising activity in phase II studies.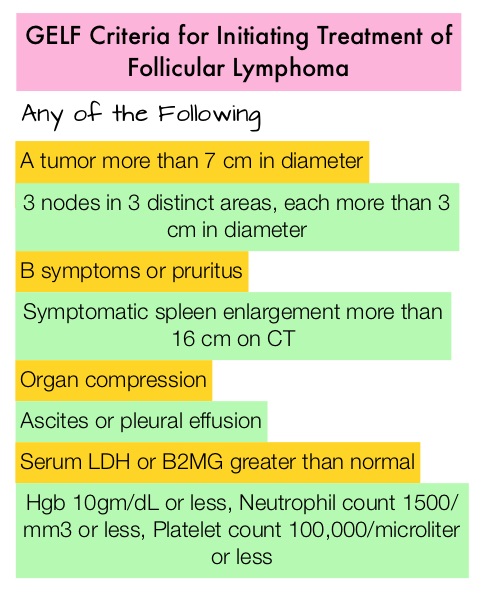
RELEVANCE is a global, randomized, open-label, phase III study, conducted in partnership with the Lymphoma Academic Research Organisation (LYSARC). This study evaluated the investigational regimen of REVLIMID® plus RITUXAN® (R2), followed by RITUXAN® maintenance, compared to the standard of care treatment of RITUXAN® plus chemotherapy, followed by RITUXAN® maintenance, in patients with previously untreated Follicular Lymphoma.
In this study, 1030 patients with treatment naïve, advanced Follicular Lymphoma, were randomized to R2 regimen (N=513) and R-Chemo regimen (N=517). Patients had Grade 1-3a Follicular Lymphoma, requiring therapy according to GELF criteria. Patients in the R2 group received REVLIMID® 20 mg orally daily on Days 2 thru 22 every 28 days for 6-12 cycles and continued responders received REVLIMID® 10 mg orally daily on Days 2 thru 22 every 28 days, for a total of 18 cycles. RITUXAN® was administered at 375 mg/m2 IV on Days 1, 8, 15, and 22 of cycle 1 and Day 1 of cycles 2 thru 6, and then continued in responders for 12 additional cycles every 8 weeks. R-Chemo group received investigators choice of standard R-CHOP (72%), R-Bendamustine (23%) or R-CVP (5%), and responding patients continued with RITUXAN® 375 mg/m2 IV every 8 weeks, for 12 cycles. The median age of the patients was 59 years. The co-Primary endpoints were Complete Response/unconfirmed Complete Response at 120 weeks and Progression Free Survival (PFS) during the preplanned analysis.
At a median follow up of 37.9 months, PFS was similar in both treatment groups and the 3-year PFS rate was 77% in the R2 group compared with 78% for the R-Chemo group (HR=1.10; P=0.48). The Complete Response/unconfirmed Complete Response at 120 weeks were 48% in the R2 group and 53% in the R-chemo group and this was also not statistically significant (P=0.13). Preliminary Overall Survival outcomes (Secondary endpoint) showed a 3-year survival rate of 94% in both treatment groups. Adverse events were different in the two treatment groups, with a higher incidence of neutropenia and febrile neutropenia in the R-Chemo group, and higher incidence of cutaneous events in the R2 group.
It was concluded that in this first randomized phase III comparison of a chemo-free regimen (R2) with standard R-Chemo, in previously untreated Follicular Lymphoma, a combination of REVLIMID® and RITUXAN® (R2) showed similar efficacy, with a more favorable safety profile, making it a potential chemo-free, firstline option, for patients with Follicular Lymphoma. RELEVANCE: Phase III randomized study of lenalidomide plus rituximab (R2) versus chemotherapy plus rituximab, followed by rituximab maintenance, in patients with previously untreated follicular lymphoma. Fowler NH, Morschhauser F, Feugier P, et al. J Clin Oncol 36, 2018 (suppl; abstr 7500)
KEYTRUDA® (Pembrolizumab)
The FDA on June 13, 2018 granted accelerated approval to KEYTRUDA® for the treatment of adult and pediatric patients with refractory Primary Mediastinal Large B-Cell Lymphoma (PMBCL), or who have relapsed after two or more prior lines of therapy. KEYTRUDA® is a product of Merck and Co., Inc.
FDA Approves KYMRIAH® for Relapsed or Refractory Large B-Cell Lymphoma
SUMMARY: The FDA on May 1, 2018 approved KYMRIAH®, a CD19-directed genetically modified autologous T-cell immunotherapy, for adult patients with Relapsed or Refractory Large B-Cell Lymphoma, after two or more lines of systemic therapy including Diffuse Large B-Cell Lymphoma (DLBCL) Not Otherwise Specified (NOS), High grade B-Cell Lymphoma and DLBCL arising from Follicular Lymphoma. The American Cancer Society estimates that in 2018, about 74,680 people will be diagnosed with Non Hodgkin Lymphoma (NHL) in the United States and about 19,910 individuals will die of this disease. Diffuse Large B-Cell Lymphoma is the most common of the aggressive Non-Hodgkin lymphomas in the United States, and the incidence has steadily increased 3-4% each year. The etiology of DLBCL is unknown. Contributing risk factors include immunosuppression (AIDS, transplantation setting, autoimmune diseases), ultraviolet radiation, pesticides, hair dyes, and diet.
What is (CAR) T-cell immunotherapy?
Chimeric Antigen Receptor (CAR) T-cell therapy is a type of immunotherapy and consists of T cells collected from the patient’s blood in a leukapheresis procedure, and genetically engineered to produce special receptors on their surface called Chimeric Antigen Receptors (CAR). These reprogrammed cytotoxic T cells with the Chimeric Antigen Receptors on their surface are now able to recognize a specific antigen on tumor cells. These genetically engineered and reprogrammed CAR T-cells are grown in the lab and are then infused into the patient. These cells in turn proliferate in the patient’s body and the engineered receptor on the cell surface help recognize and kill cancer cells that expresses that specific antigen. KYMRIAH® (genetically engineered T-cells) seeks out cancer cells expressing the antigen CD19, which is found uniquely on B cells and destroy them. Patients, following treatment with CAR T-cells, develop B-cell aplasia (absence of CD19 positive cells) due to B-cell destruction and may need immunoglobin replacement. Hence, B-cell aplasia can be a useful therapeutic marker, as continued B-cell aplasia has been seen in all patients who had sustained remission, following CAR T-cell therapy. Cytokine Release Syndrome, an inflammatory process is the most common and serious side effect of CAR T-cell therapy and is associated with marked elevation of Interleukin-6. Cytokine release is important for T-cell activation and can result in high fevers and myalgias. This is usually self limiting although if severe can be associated with hypotension and respiratory insufficiency. Tocilizumab (ACTEMRA®), an Interleukin-6 receptor blocking antibody produces a rapid improvement in symptoms. This is however not recommended unless the symptoms are severe and life threatening, as blunting the cytokine response can in turn negate T-cell proliferation. Elevated serum Ferritin and C-reactive protein levels are surrogate markers for severe Cytokine Release Syndrome.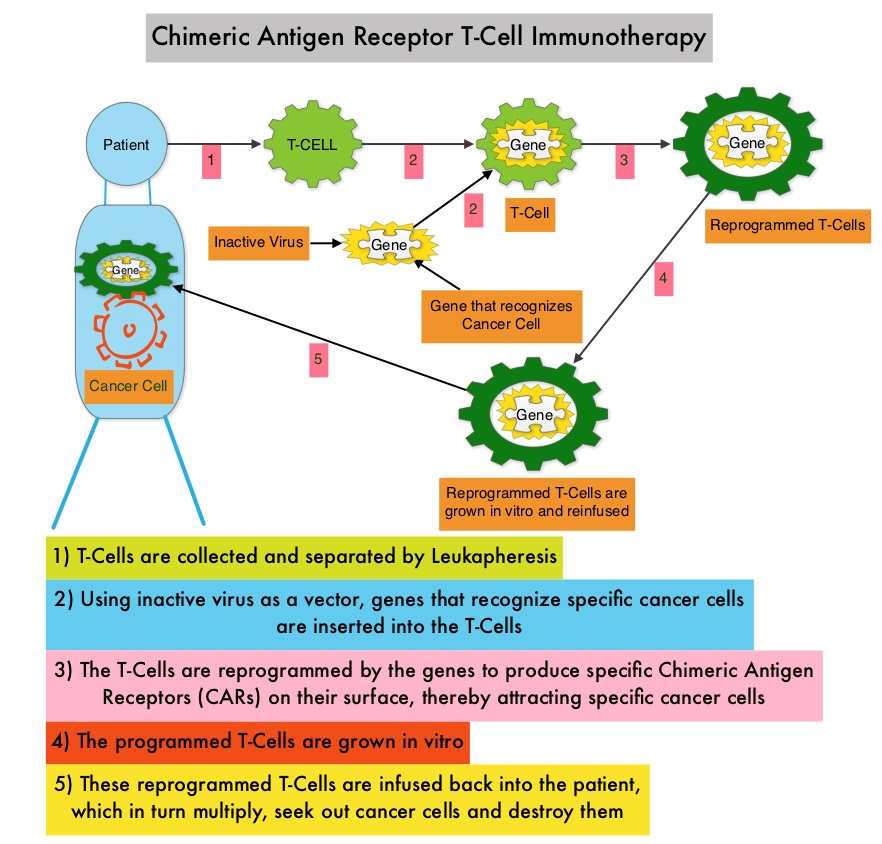
The CAR T-cells have been shown to also access sanctuary sites such as the central nervous system and eradicate cancer cells. CD19 antigen is expressed by majority of the B-cell malignancies and therefore most studies using CAR T-cell therapy have focused on the treatment of advanced B-cell malignancies such as Chronic Lymphocytic Leukemia (CLL), Acute Lymphoblastic Leukemia (ALL) and Non Hodgkin lymphoma (NHL), such as Diffuse Large B-Cell Lymphoma (DLBCL).
The approval of KYMRIAH® was based on a single-arm, open-label, multi-center, global, pivotal phase II trial (JULIET), in adults with Relapsed or Refractory DLBCL and DLBCL after transformation from Follicular lymphoma. The study enrolled 147 patients, 99 of whom received the CAR T-cell infusion with a single dose of KYMRIAH®, which was manufactured at 2 sites (United States and Germany). Eligible patients were 18 years or older with Relapsed or Refractory DLBCL and had progressed after receiving two or more lines of chemotherapy, including an Anthracycline and Rituximab, and were ineligible for or failed Autologous Stem Cell Transplant (auto-SCT). The median number of prior lines of therapy was 3 and 47% of patients had prior auto-SCT. Prior to infusion with KYMRIAH®, 90% of patients received bridging therapy, 93% received lymphodepleting chemotherapy, which in most patients consisted of Fludarabine/Cyclophosphamide. The median age was 56 years and 77% of patients had Stage III or IV disease at the time of enrollment. The median time from infusion to data cutoff was 5.6 months. The Primary endpoint was best Overall Response Rate-ORR (Complete Response-CR + Partial Response-PR), per independent review committee.
In this primary analysis, the authors reported the outcomes among 81 patients who received KYMRIAH® manufactured in the United States, with more than 3 months of follow up. The Objective Response Rate was 53%, the Complete Response rate was 39.5% and Partial Response rate 13.6%. At month 3, the CR rate was 32% and the PR rate 6%. Among patients evaluable at 6 months (N=46), the CR Rate was 30% and PR rate was 7%. Response rates were consistent across prognostic subgroups, including those who received prior auto-SCT and those with Double-Hit lymphoma. The median Duration of Response and the median Overall Survival were not reached. The 6-month probability of being relapse free was 73.5% and the 6-month probability of Overall Survival was 64.5%. Grade 3 or 4 adverse events were reported in 86% of the patients and Cytokine-Release Syndrome occurred in 58%. CRS was managed with ACTEMRA® in 15% of patients with good response and 11% of patients received corticosteroids. Neurologic adverse events were reported in 12% of patients. No deaths were attributed to KYMRIAH®.
It was concluded that KYMRIAH® produces high Response Rates with 95% of Complete Responses at 3 months being sustained at 6 months, in heavily pretreated adult patients with Relapsed or Refractory Diffuse Large B-Cell Lymphoma (DLBCL). This first global study of CAR T-cell therapy in DLBCL also demonstrated that centralized manufacturing of CAR T-cells is feasible. Schuster SJ, Bishop MR, Tam CS, et al. Primary Analysis of Juliet: A Global, Pivotal, Phase 2 trial of CTL019 in Adult Patients with Relapsed or Refractory Diffuse Large B-Cell Lymphoma. Presented at: ASH Annual Meeting and Exposition; Dec. 9-12, 2017; Atlanta. Abstract 577.
KYMRIAH® (Tisagenlecleucel)
The FDA on May 1, 2018 approved KYMRIAH®, a CD19-directed genetically modified autologous T-cell immunotherapy, for adult patients with relapsed or refractory large B-cell lymphoma, after two or more lines of systemic therapy including Diffuse Large B-Cell Lymphoma (DLBCL) not otherwise specified, high grade B-cell lymphoma and DLBCL arising from Follicular Lymphoma. KYMRIAH® is a product of Novartis Pharmaceuticals Corp.