
The FDA on June 12, 2025, approved KEYTRUDA® for adults with resectable locally advanced Head and Neck Squamous Cell Carcinoma (HNSCC) whose tumors express PD-L1 [Combined Positive Score (CPS) ≥1] as determined by an FDA-approved test, as a single agent as neoadjuvant treatment, continued as adjuvant treatment in combination with Radiotherapy (RT) with or without Cisplatin after surgery, and then as a single agent. KEYTRUDA® is a product of Merck.
Tag: Head & Neck: Oropharynx
De-escalated Adjuvant Radiotherapy Demonstrates Reduced Long-Term Toxicity in HPV-Associated Oropharyngeal Cancer
SUMMARY: The American Cancer Society estimates that about 59,660 new cases of oral cavity and pharynx cancer will be diagnosed in the US in 2025 and about 12,770 patients will die of the disease. According to the CDC, about 46,711 Human PapillomaVirus (HPV)-associated cancers occur in the United States each year (25,689 among women, and 21,022 among men). Cervical cancer is the most common HPV-associated cancer among women, and Oropharyngeal cancers are the most common among men. There has been a significant increase in the incidence during the past several decades, due to changes in sexual practices.
HPV-positive Oropharyngeal Squamous Cell Carcinoma (OPSCC) is an entirely distinct disease entity from HPV-negative OPSCC. Patients with HPV-positive OPSCC tend to be younger males, who are former smokers or nonsmokers, with risk factors for exposure to High Risk HPV. The HPV-positive primary Squamous Cell Carcinoma tend to be smaller in size, with early nodal metastases, and these patients have a better prognosis compared with patients with HPV-negative Head and Neck Squamous Cell Carcinoma (HNSCC) when treated similarly. Expression of tumor suppressor protein, known as p16, is highly correlated with infection with HPV in HNSCC. Accurate HPV assessment in Head and Neck cancers is becoming important as it significantly impacts clinical management. HPV status is considered the most important prognostic indicator in patients with Head and Neck cancer, and p16 status is now included in the American Joint Committee on Cancer (AJCC) Staging System.
HPV-positive OPSCC is more sensitive to chemotherapy and radiotherapy than is HPV-negative OPSCC, which translates to a much better prognosis and survival, when treated with a combination of platinum based chemotherapy and radiotherapy. This treatment however can be associated with substantial morbidity and lifelong toxicities such as dry mouth, difficulty swallowing, and loss of taste. These tumors, typically being more responsive to therapy than their non-HPV counterparts, appear to benefit from reduced radiation doses, potentially minimizing the severe toxicities linked with conventional radiotherapy, without compromising oncologic outcomes.
Adjuvant chemoradiotherapy has been a mainstay of treatment for patients with surgically resected HPV-positive OPSCC, offering excellent oncologic control. However, standard radiotherapy regimens, typically 60-66 Gy with concurrent chemotherapy, are associated with substantial treatment-related morbidity, particularly long-term dysphagia and feeding tube dependence. With the rising incidence of HPV-driven OPSCC in younger patients with favorable prognoses, interest has grown in identifying de-escalated approaches that maintain efficacy while reducing toxicity.
Trial Overview
The MC1675 Phase III trial (NCT02908477), conducted at two Mayo Clinic sites, directly compared a de-intensified adjuvant regimen against the conventional standard of care. Eligible participants were adults with resected, pathologic Stage III–IV HPV-associated OPSCC (≥70% p16 expression) and at least one intermediate-risk pathological feature. Patients had an ECOG performance status of 0-1 and were stratified by extranodal extension and smoking history.
A total of 194 patients were randomized 2:1 to receive either:
- De-escalated regimen (DART): 30-36 Gy delivered in 1.5-1.8 Gy twice-daily fractions over 2 weeks, with Docetaxel 15 mg/m² IV on days 1 and 8.
- Standard of care (SOC): 60 Gy delivered in 2 Gy daily fractions over 6 weeks, with concurrent weekly IV Cisplatin at 40 mg/m².
The Primary endpoint was the cumulative incidence of chronic grade ≥3 toxicity between 3 and 24 months post-treatment.
Key Findings
With a median follow-up of 37.3 months, the trial confirmed that de-escalated adjuvant therapy significantly reduced late high-grade toxicities:
- Cumulative grade ≥3 toxicity: 3% with DART vs 11% with SOC (P=0.042).
- Feeding tube dependence: 2% with DART vs 8% with SOC (p=0.039).
- Most frequent toxicities: Dysphagia (2%) and esophagitis (1%) in the DART arm vs dysphagia (8%), fatigue (2%), pain (2%), and osteonecrosis of the jaw (2%) in the SOC arm.
Importantly, no new unexpected safety signals emerged, and the reduction in morbidity was consistent across subgroups.
Clinical Implications
These findings add to the growing body of evidence that de-intensification strategies can safely reduce long-term treatment burden for patients with HPV-associated OPSCC, a population with excellent baseline prognosis. The DART approach, using half the standard radiation dose combined with Docetaxel, achieved meaningful reductions in swallowing dysfunction and PEG tube dependence, two of the most disabling toxicities after chemoradiation.
While efficacy outcomes were not the primary endpoint, the trial’s results suggest that oncologic control can be preserved even with substantially lower radiation exposure, provided patient selection is stringent. Longer follow-up and confirmatory studies will be critical to define which subsets of patients may benefit most, and whether this regimen could shift practice standards for intermediate-risk HPV-positive disease.
Looking Ahead
The MC1675 trial underscores a pivotal movement in head and neck oncology, tailoring therapy intensity to disease biology and patient risk, rather than applying a uniform high-intensity standard. For the increasing number of younger patients facing decades of survivorship, approaches like DART may offer durable disease control with far less long-term morbidity. Ongoing research will clarify whether such regimens could become a new benchmark for adjuvant treatment in this favorable-risk population.
De-escalated adjuvant radiotherapy versus standard adjuvant treatment for human papillomavirus-associated oropharyngeal squamous cell carcinoma (MC1675): a phase 3, open-label, randomised controlled trial. Ma D, Price K, Moore E, et al. The Lancet Oncology. 2025;26:1227-1239
FDA Approves Perioperative KEYTRUDA® for Resectable Locally Advanced Head and Neck Squamous Cell Carcinoma
SUMMARY: The FDA on June 12, 2025, approved Pembrolizumab (KEYTRUDA®) for adults with resectable locally advanced Head and Neck Squamous Cell Carcinoma (HNSCC) whose tumors express PD-L1 Combined Positive Score (CPS) of 1 or more, as determined by an FDA-approved test, as a single agent as neoadjuvant treatment, continued as adjuvant treatment in combination with Radiotherapy (RT) with or without Cisplatin after surgery, and then as a single agent.This is the first approval for HNSCC in 6 years and the first overall perioperative approval for locally advanced HNSCC.
The American Cancer Society estimates that 59,660 new cases of cancer involving the oral cavity and pharynx will be diagnosed in the US in 2025 and 12,770 will die of the disease. The Head and Neck region includes the oral cavity, oropharynx, hypopharynx and larynx. Squamous Cell Carcinoma (SCC) of the Head and Neck accounts for about 3-5% of all cancers in the United States. Common risk factors include tobacco and alcohol use and Human PapillomaVirus (HPV) infection. Even though tobacco has long been associated with head and neck cancer development, cannabis has similar carcinogens.
The Standard of Care for patients with Stage III–IVA Head and Neck Squamous Cell Carcinoma (HNSCC) has remained largely static for nearly 2 decades: surgery followed by risk-adapted adjuvant radiotherapy, with or without concurrent chemotherapy. Despite refinements in technique and supportive care, relapse rates remain high, particularly among patients with adverse pathological features such as extranodal extension and positive margins.
The treatment paradigm for Head and Neck cancer has been rapidly evolving with the recognition and better understanding of immune evasion and the role of immune checkpoints or gate keepers in suppressing antitumor immunity. Blocking the immune checkpoints unleashes the T cells, resulting in T cell proliferation, activation, and a therapeutic response. Checkpoint inhibitors administered in a neoadjuvant setting activates both the priming phase of immunity within tumor tissue, and the effector phase within the tumor microenvironment. It has been shown that neoadjuvant immunotherapy expands more T-cell clones than adjuvant treatment. Preclinical models have also demonstrated that both radiation therapy and Cisplatin chemotherapy increase the PD-L1 expression on the tumor, suggesting that combining radiotherapy with anti-PD-1 therapy could improve the outcomes.
Pembrolizumab (KEYTRUDA®) is a fully humanized, Immunoglobulin G4, monoclonal antibody and checkpoint inhibitor, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. Pembrolizumab has been shown to improve Overall Survival in patients with Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma
KEYNOTE-689, a landmark Phase 3 trial, has provided the most compelling evidence to date that perioperative immunotherapy, specifically Pembrolizumab, can significantly improve clinical outcomes for patients with resectable, locally advanced Head and Neck Squamous Cell Carcinoma (HNSCC). This international, randomized, placebo-controlled study enrolled 714 patients (N=714) with newly diagnosed, resectable, Stage III–IVA HNSCC of the oral cavity, oropharynx, larynx, or hypopharynx.
Patients were randomized 1:1 to receive:
- Investigational arm (N=356):
- 2 cycles of neoadjuvant Pembrolizumab (200 mg IV Q3W) starting about 3 weeks before surgery.
- Standard-of-care surgery.
- Up to 3 doses of Pembrolizumab administered concurrently with adjuvant chemoradiotherapy, with Cisplatin (depending on pathologic risk- positive margins <1 mm or extranodal extension present at surgery was considered high risk).
- 12 additional adjuvant doses of Pembrolizumab Q3W (total treatment duration: about 1 year).
- Control arm (N=358):
- Identical treatment structure, substituting placebo for Pembrolizumab.
PD-L1 expression was assessed via Combined Positive Score (CPS), and stratification included CPS ≥1 and CPS ≥10 subgroups, recognizing the prognostic and potentially predictive value of PD-L1 expression. The Primary endpoint was Event-Free Survival (EFS) by Blinded Independent Central Review, defined as time from randomization to disease progression, local/regional recurrence, distant metastasis, or death from any cause. Secondary endpoints included Overall Survival (OS) and Major Pathological Response.
The trial met its Primary endpoint of EFS. At median follow-up of 38.3 months, patients in the investigational arm had significantly improved EFS compared with the Standard of Care arm (median 51.8 months vs. 30.4 months; HR=0.73; P=0.0041). Patients who received Pembrolizumab who had a CPS score ≥10 derived the greatest benefit (median 59.7 months vs. 26.9 months; HR = 0.66; P=0.002) whereas the median EFS in the CPS ≥1 subgroup was 59.7 vs. 29.6 months (HR, 0.70; P = .0014).
Major pathological response defined as 90% or more tumor regression was also notably improved. Among all patients, the major pathological response rate was 9.4% with Pembrolizumab vs. 0% with Standard of Care (P < 0.00001). In the CPS ≥10 subgroup, the major pathological response rate reached 13.7%.
While the interim analysis did not demonstrate a statistically significant OS benefit, trends were favorable, particularly in the CPS ≥10 group (HR, 0.72; P =0.02). Further OS follow-up is ongoing.
Adverse events were consistent with known profiles of checkpoint inhibitors. Grade 3 or more Treatment-Related Adverse Events (TRAEs) occurred in 44.6% of the Pembrolizumab group and 42.9% in the Standard of Care group. Immune-mediated adverse events were observed in 43.2% of the Pembrolizumab arm, with hypothyroidism being the most common (24.7%). Mortality attributable to treatment was slightly higher with Pembrolizumab (1.1% vs. 0.3%).
The researchers concluded that perioperative Pembrolizumab is now emerging as a new standard of care in the treatment of resectable locally advanced HNSCC. The findings from this study underscore the importance of harnessing the immune system both before and after surgery. Neoadjuvant administration may prime the immune response when tumor antigen burden is highest, while adjuvant therapy may help eliminate residual microscopic disease.
Neoadjuvant and adjuvant pembrolizumab plus standard of care in resectable locally advanced head and neck squamous cell carcinoma: phase 3 KEYNOTE-689 study. Uppaluri R, et al. Abstract CT001. Presented at: American Association for Cancer Research Annual Meeting; April 25-30, 2025; Chicago.
Late Breaking Abstract – ASCO 2025: A New Era for High-Risk Resected Head and Neck Cancer: Nivolumab Adds Disease-Free Survival Benefit in NIVOPOSTOP Trial
SUMMARY: The American Cancer Society estimates that 59,660 new cases of cancer involving the oral cavity and pharynx will be diagnosed in the US in 2025 and 12,770 will die of the disease. The head and neck region includes the oral cavity, oropharynx, hypopharynx and larynx. Squamous Cell Carcinoma (SCC) of the Head and Neck accounts for about 3-5% of all cancers in the United States. Common risk factors include tobacco and alcohol use and Human PapillomaVirus (HPV) infection. Even though tobacco has long been associated with head and neck cancer development, cannabis has similar carcinogens.
The Standard of Care for patients with Stage III–IVA Head and Neck Squamous Cell Carcinoma (HNSCC) has remained largely static for nearly 2 decades: surgery followed by risk-adapted adjuvant radiotherapy, with or without concurrent Cisplatin based chemotherapy. Despite refinements in technique and supportive care, relapse rates remain high, particularly among patients with adverse pathological features such as extranodal extension and positive margins.
The treatment paradigm for Head and Neck cancer has been rapidly evolving with the recognition and better understanding of immune evasion and the role of immune checkpoints or gate keepers in suppressing antitumor immunity. Blocking the immune checkpoints unleashes the T cells, resulting in T cell proliferation, activation, and a therapeutic response. Checkpoint inhibitors administered in a neoadjuvant setting activates both the priming phase of immunity within tumor tissue, and the effector phase within the tumor microenvironment. It has been shown that neoadjuvant immunotherapy expands more T-cell clones than adjuvant treatment. Preclinical models have also demonstrated that both radiation therapy and Cisplatin chemotherapy increase the PD-L1 expression on the tumor, suggesting that combining radiotherapy with anti-PD-1 therapy could improve the outcomes.
Phase 3 NIVOPOSTOP trial (GORTEC 2018-01) provides compelling evidence that integrating immunotherapy into the adjuvant setting may finally shift this long-standing treatment landscape. Nivolumab (OPDIVO®) is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2. Blocking the Immune checkpoint proteins unleashes the T cells, resulting in T cell proliferation, activation and a therapeutic response.
Study Design and Patient Population
NIVOPOSTOP (NCT03576417) was an international, randomized, open-label Phase 3 study that enrolled 680 patients with completely resected LA-SCCHN (Locally Advanced Squamous Cell Carcinoma of the Head and Neck), which included the oral cavity, oropharynx, hypopharynx, and larynx. Eligible patients were less than 75 years old, with ECOG performance status 0-1, and exhibited high-risk features for recurrence, including extracapsular nodal extension, positive surgical margins, involvement of 4 or more lymph nodes, or extensive perineural invasion. PD-L1 expression was not required for study eligibility. Majority of patients had disease of the oral cavity (58%), about 50% were current smokers, most patients had Stage IVA or IVB disease (83%), and slightly more than one-half of patients (56%) had a PD-L1 Combined Positive Score less than 20. Patients were first stratified by HPV status and enrolling center before being randomly assigned to receive standard CRT or standard CRT plus nivolumab.
Patients were randomized 1:1 to receive:
- Control Arm (SOC CRT): 66 Gy radiotherapy with three cycles of Cisplatin 100 mg/m² Q3W (N=334).
- Experimental Arm (NIVO + CRT): One lead-in dose of Nivolumab 240 mg, followed by CRT plus Nivolumab 360 mg Q3W for three cycles, followed by six cycles of Nivolumab 480 mg Q4W for maintenance (N=332).
Both treatment groups were well balanced. The Primary endpoint was Disease Free Survival (DFS). Key Secondary endpoints include Overall Survival (OS) and Safety.
Primary Endpoint Met: Significant Improvement in Disease-Free Survival
At a median follow-up of 30.3 months, the trial met its Primary endpoint. Among the 666 patients included in the Disease-Free Survival (DFS) analysis (ITT population), the addition of adjuvant Nivolumab significantly reduced the risk of disease recurrence or death compared with CRT alone (HR 0.76; 95% CI, 0.60–0.98; P = 0.034).
Three-year DFS rates were 63.1% with NIVO + CRT (95% CI, 57.0–68.7) and 52.5% with CRT alone (95% CI, 46.2–58.4). This represents a 24% relative reduction in recurrence risk with Nivolumab. Importantly, this benefit was observed across all PD-L1 expression levels, supporting the use of this strategy in an unselected population.
Safety Profile: Manageable Toxicity with Increased Grade 3–4 Events
While the addition of Nivolumab was associated with an increase in grade 3-4 adverse events, particularly within the first 100 days post-CRT (13.1% vs. 5.6%), no increase in treatment-related mortality was seen (0.6% vs. 0.7%). Late grade ≥3 toxicities occurring beyond 9 months were rare in both groups and did not exceed grade 3. The overall safety profile was considered acceptable and consistent with known immune-related toxicities.
Locoregional Control Improved with Nivolumab
One of the most noteworthy findings was a significant reduction in locoregional recurrences. At 3 years, locoregional failure occurred in 13% of patients in the NIVO + CRT arm versus 20% in the CRT-only arm (HR 0.63; 95% CI, 0.42–0.94). Interestingly, unlike perioperative immunotherapy regimens such as KEYNOTE-689 that predominantly reduced distant failures, NIVOPOSTOP’s benefit was concentrated in locoregional disease control, suggesting a synergistic effect between radiotherapy and immune checkpoint inhibition.
Survival Data Pending but Trending Favorably
Although Overall Survival (OS) data remain immature, early trends favor the Nivolumab arm. At the time of reporting, 74% of patients receiving NIVO + CRT remained alive at 3 years, compared to 68% in the CRT-alone group. The final OS analysis is planned upon reaching 283 events (currently at 158).
Clinical Context and Expert Perspectives
The NIVOPOSTOP findings stand in sharp contrast to prior trials like KEYNOTE-412 and JAVELIN Head and Neck 100, which failed to show benefit from concurrent immune checkpoint inhibitor with CRT in unselected populations. Notably, the timing and sequencing of immunotherapy in NIVOPOSTOP, administered in the postoperative setting and continued as maintenance may have circumvented the immunosuppressive milieu of CRT and allowed more robust immune priming. The researchers emphasized the clinical need among the ~40–45% of LA-SCCHN patients who relapse after surgery and CRT.
Conclusion
NIVOPOSTOP represents the first successful Phase 3 trial to demonstrate a Disease-Free Survival advantage with the addition of immunotherapy to adjuvant CRT in high-risk, resected LA-SCCHN. With a favorable balance of efficacy and manageable toxicity, this regimen is poised to reshape clinical practice, marking a long-overdue advancement in the postoperative management of head and neck cancer.
NIVOPOSTOP (GORTEC 2018-01): A phase III randomized trial of adjuvant nivolumab added to radio-chemotherapy in patients with resected head and neck squamous cell carcinoma at high risk of relapse. Bourhis J, Auperin A, Borel C, et al. J Clin Oncol 43, 2025 (suppl 17; abstr LBA2).
Perioperative KEYTRUDA® Reshapes the Treatment Landscape for Resectable Locally Advanced HNSCC
SUMMARY: The American Cancer Society estimates that 59,660 new cases of cancer involving the oral cavity and pharynx will be diagnosed in the US in 2025 and 12,770 will die of the disease. The head and neck region includes the oral cavity, oropharynx, hypopharynx and larynx. Squamous Cell Carcinoma (SCC) of the Head and Neck accounts for about 3-5% of all cancers in the United States. Common risk factors include tobacco and alcohol use and Human PapillomaVirus (HPV) infection. Even though tobacco has long been associated with head and neck cancer development, cannabis has similar carcinogens.
The Standard of Care for patients with Stage III–IVA Head and Neck Squamous Cell Carcinoma (HNSCC) has remained largely static for nearly 2 decades: surgery followed by risk-adapted adjuvant radiotherapy, with or without concurrent chemotherapy. Despite refinements in technique and supportive care, relapse rates remain high, particularly among patients with adverse pathological features such as extranodal extension and positive margins.
The treatment paradigm for Head and Neck cancer has been rapidly evolving with the recognition and better understanding of immune evasion and the role of immune checkpoints or gate keepers in suppressing antitumor immunity. Blocking the immune checkpoints unleashes the T cells, resulting in T cell proliferation, activation, and a therapeutic response. Checkpoint inhibitors administered in a neoadjuvant setting activates both the priming phase of immunity within tumor tissue, and the effector phase within the tumor microenvironment. It has been shown that neoadjuvant immunotherapy expands more T-cell clones than adjuvant treatment. Preclinical models have also demonstrated that both radiation therapy and Cisplatin chemotherapy increase the PD-L1 expression on the tumor, suggesting that combining radiotherapy with anti-PD-1 therapy could improve the outcomes.
Pembrolizumab (KEYTRUDA®) is a fully humanized, Immunoglobulin G4, monoclonal antibody and checkpoint inhibitor, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. Pembrolizumab has been shown to improve Overall Survival in patients with Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma
KEYNOTE-689, a landmark Phase 3 trial, has provided the most compelling evidence to date that perioperative immunotherapy, specifically Pembrolizumab, can significantly improve clinical outcomes for patients with resectable, locally advanced Head and Neck Squamous Cell Carcinoma (HNSCC). This international, randomized, placebo-controlled study enrolled 714 patients (N=714) with newly diagnosed, resectable, Stage III–IVA HNSCC of the oral cavity, oropharynx, larynx, or hypopharynx.
Patients were randomized 1:1 to receive:
- Investigational arm (N=356):
- 2 cycles of neoadjuvant Pembrolizumab (200 mg IV Q3W) starting about 3 weeks before surgery.
- Standard-of-care surgery.
- Up to 3 doses of Pembrolizumab administered concurrently with adjuvant chemoradiotherapy (depending on pathologic risk).
- 12 additional adjuvant doses of Pembrolizumab Q3W (total treatment duration: about 1 year).
- Control arm (N=358):
- Identical treatment structure, substituting placebo for Pembrolizumab.
PD-L1 expression was assessed via Combined Positive Score (CPS), and stratification included CPS ≥1 and CPS ≥10 subgroups, recognizing the prognostic and potentially predictive value of PD-L1 expression. The Primary endpoint was Event-Free Survival (EFS), defined as time from randomization to disease progression, local/regional recurrence, distant metastasis, or death from any cause. Secondary endpoints included Overall Survival (OS) and Major Pathological Response.
The trial met its Primary endpoint of EFS. At median follow-up of 38.3 months, patients in the investigational arm had significantly improved EFS compared with the Standard of Care arm (median 51.8 months vs. 30.4 months; HR=0.73; P=0.0041). Patients who received Pembrolizumab who had a CPS score ≥10 derived the greatest benefit (median 59.7 months vs. 26.9 months; HR = 0.66; P=0.002) whereas the median EFS in the CPS ≥1 subgroup was 59.7 vs. 29.6 months (HR, 0.70; P = .0014).
Major pathological response defined as 90% or more tumor regression was also notably improved. Among all patients, the major pathological response rate was 9.4% with Pembrolizumab vs. 0% with Standard of Care (P < 0.00001). In the CPS ≥10 subgroup, the major pathological response rate reached 13.7%.
While the interim analysis did not demonstrate a statistically significant OS benefit, trends were favorable, particularly in the CPS ≥10 group (HR, 0.72; P =0.02). Further OS follow-up is ongoing.
Adverse events were consistent with known profiles of checkpoint inhibitors. Grade 3 or more Treatment-Related Adverse Events (TRAEs) occurred in 44.6% of the Pembrolizumab group and 42.9% in the Standard of Care group. Immune-mediated adverse events were observed in 43.2% of the Pembrolizumab arm, with hypothyroidism being the most common (24.7%). Mortality attributable to treatment was slightly higher with Pembrolizumab (1.1% vs. 0.3%).
The researchers concluded that perioperative Pembrolizumab is now emerging as a new standard of care in the treatment of resectable locally advanced HNSCC. The findings from this study underscore the importance of harnessing the immune system both before and after surgery. Neoadjuvant administration may prime the immune response when tumor antigen burden is highest, while adjuvant therapy may help eliminate residual microscopic disease.
Neoadjuvant and adjuvant pembrolizumab plus standard of care in resectable locally advanced head and neck squamous cell carcinoma: phase 3 KEYNOTE-689 study. Uppaluri R, et al. Abstract CT001. Presented at: American Association for Cancer Research Annual Meeting; April 25-30, 2025; Chicago.
Cannabis Use Increases the Risk of Head and Neck Cancer
SUMMARY: The American Cancer Society estimates that about 58,450 new cases of oral cavity and pharynx cancer will be diagnosed in the US in 2024 and about 12,230 patients will die of the disease. The head and neck region includes the oral cavity, oropharynx, hypopharynx and larynx. Squamous Cell Carcinoma of the Head and Neck accounts for about 3-5% of all cancers in the United States. Common risk factors include tobacco and alcohol use and Human PapillomaVirus (HPV) infection. Even though tobacco has long been associated with head and neck cancer development, cannabis has similar carcinogens.
Cannabis refers to all products derived from the plant Cannabis sativa, and is the most commonly used illicit substance worldwide. The cannabis plant contains about 540 chemical substances and has similar carcinogens as tobacco. Marijuana refers to the dried leaves, flowers, stems, and seeds from the plant Cannabis sativa that contain substantial amounts of TetraHydroCannabinol (THC), which is primarily responsible for the effects of marijuana on a persons mental state. Individuals with head and neck cancer have used cannabis to help alleviate pain and improve well-being. In 2022, 30.7% of 12th graders reported using marijuana in the previous year and 6.3% reported using marijuana daily. In addition, many young people also use vaping devices to consume cannabis products.
As cannabis use grows, understanding its carcinogenic potential becomes increasingly important, particularly given its rising popularity and industry expansion. Cannabis smoke may be more proinflammatory than tobacco smoke due to its unfiltered nature and higher combustion temperature. This increased inflammation could lead to cancer development. Cannabis smoke also enhances the expression of Epidermal Growth Factor Receptor (EGFR), which is associated with many head and neck squamous cell carcinomas, including Laryngeal cancer. It remained unclear if cannabis use is associated with increased risk of head and neck cancer.
The researchers conducted a large-scale, retrospective cohort study over a 20 year period from April 19, 2004, to April 19, 2024, to investigate whether there is an association between cannabis use and an increased risk of head and neck cancers. Given the growing prevalence of cannabis use and its potential health effects, understanding this relationship is crucial for public health. In this study, clinical records of 116,076 U.S. adults with and without cannabis-related disorders who had outpatient hospital clinic visits and no prior history of head and neck cancers were extracted from a database covering 64 healthcare organizations across the United States. The mean age of 46.4 years, 44.5% were women and 60% white. Cannabis-related disorder was defined as excessive cannabis use leading to psychosocial symptoms, including impaired occupational or social functioning. The control cohort consisted of 3,985,286 individuals with a mean age of 60.8 years (54.5% women, 74.6% white), with no cannabis-related disorder. Participants were matched for age, race, tobacco use, and alcohol-related disorders. Relative risks (RRs) for head and neck cancers and subtypes were calculated, with stratified analysis for those younger and older than 60 years.
It was noted that Individuals with cannabis-related disorder had a significantly higher risk of developing any type of head and neck cancer, compared to those without such disorders. Specifically, the risk for any head and neck cancer was 3.49 times greater in the cannabis-related disorder group. A site-specific analysis yielded that among those with cannabis-related disorder, Laryngeal cancer risk was 8.39 times higher, Oropharyngeal cancer risk was 4.9 times higher, Salivary gland cancer risk was 2.7 times higher, Nasopharyngeal cancer risk was 2.6 times higher and Oral cancer risk was 2.51 times higher. Risks were consistent across different age groups. Elevated risks persisted when cancer diagnoses were considered at least one year or five years after the initial cannabis use, indicating a sustained risk over time.
One of the study limitations was that the study did not capture information on the frequency, quantity, or type of cannabis use, which are crucial for understanding the dose-response relationship.
In conclusion, this study confirms a significant association between cannabis-related disorder and an increased risk of head and neck cancers, particularly Laryngeal and Oropharyngeal cancers. Future studies should focus on understanding the mechanisms behind this association and investigate the impact of cannabis use dose and duration on cancer risk. More comprehensive data collection and analysis are necessary to solidify these findings and inform public health recommendations.
Cannabis Use and Head and Neck Cancer. Gallagher TJ, Chung RS, Lin ME, et al. JAMA Otolaryngol Head Neck Surg. Published online August 8, 2024. doi:10.1001/jamaoto.2024.2419.
De-escalation of Treatment for HPV-Associated Oropharyngeal Cancer
SUMMARY: The American Cancer Society estimates that about 58,450 new cases of oral cavity and pharynx cancer will be diagnosed in the US in 2024 and about 12,230 patients will die of the disease. According to the CDC, about 46,711 Human PapillomaVirus (HPV)-associated cancers occur in the United States each year (25,689 among women, and 21,022 among men). Cervical cancer is the most common HPV-associated cancer among women, and Oropharyngeal cancers are the most common among men. There has been a significant increase in the incidence during the past several decades, due to changes in sexual practices.
HPV-positive Oropharyngeal Squamous Cell Carcinoma (OPSCC) is an entirely distinct disease entity from HPV-negative OPSCC. Patients with HPV-positive OPSCC tend to be younger males, who are former smokers or nonsmokers, with risk factors for exposure to High Risk HPV. The HPV-positive primary Squamous Cell Carcinoma tend to be smaller in size, with early nodal metastases, and these patients have a better prognosis compared with patients with HPV-negative Head and Neck Squamous Cell Carcinoma (HNSCC) when treated similarly. Expression of tumor suppressor protein, known as p16, is highly correlated with infection with HPV in HNSCC. Accurate HPV assessment in Head and Neck cancers is becoming important as it significantly impacts clinical management. HPV status is considered the most important prognostic indicator in patients with Head and Neck cancer, and p16 status is now included in the American Joint Committee on Cancer (AJCC) Staging System.
HPV-positive OPSCC is more sensitive to chemotherapy and radiotherapy than is HPV-negative OPSCC, which translates to a much better prognosis and survival, when treated with a combination of platinum based chemotherapy and radiotherapy. This treatment however can be associated with substantial morbidity and lifelong toxicities such as dry mouth, difficulty swallowing, and loss of taste. These tumors, typically being more responsive to therapy than their non-HPV counterparts, appear to benefit from reduced radiation doses, potentially minimizing the severe toxicities linked with conventional radiotherapy, without compromising oncologic outcomes.
Two pivotal studies presented at the 2024 Multidisciplinary Head and Neck Cancers Symposium have provided compelling evidence supporting the deintensification of radiotherapy in early-stage Oropharyngeal Squamous Cell Carcinomas associated with HPV. The approach for the first study was de-escalated postoperative adjuvant therapy, whereas the second study utilized mid-treatment FDG-PET response criteria to select patients eligible for de-escalated radiotherapy
Study by Washington University School of Medicine: De-escalation of Postoperative Adjuvant Therapy
The MINT trial (The Minimalist Trial) is a nonrandomized Phase II study which enrolled 58 patients with clinical Stage I–III HPV-positive Oropharyngeal Squamous Cell Carcinoma, or with a positive neck node with an unknown primary, who underwent surgery and selective neck dissection. Out of these, 54 patients were stratified post-surgery into three treatment groups based on pathologic risk:
Group 1: High-risk pathology patients (extracapsular extension or positive margin but not clinical or pathologic T4 or clinical N3 disease) received de-escalated postoperative adjuvant chemoradiotherapy with Cisplatin at 100 mg/m2 for one dose plus 42 Gy of radiotherapy in 21 daily fractions (N=20)
Group 2: Intermediate-risk pathology patients (lymphovascular invasion, perineural invasion, at least two positive nodes, at least one positive node 3 mm, T3 or N2 disease, but no extracapsular extension or positive margins, and not clinical or pathologic T4 or clinical N3 disease) received de-escalated postoperative adjuvant radiotherapy with 42 Gy in 21 daily fractions (N=30)
Group 3: Highest-risk pathology (Patients with clinical or pathologic T4 or clinical N3 disease) received standard-of-care treatment with higher doses of Cisplatin at 100 mg/m2 for three doses plus 60 Gy of radiotherapy delivered concurrently (N=4).
So, the experimental arms involved de-escalating postoperative chemoradiotherapy in Group 1 and de-escalating postoperative radiotherapy in Group 2. The Primary outcome measure was mean percent weight change starting at Day 1 and ending on the last day of radiation therapy (approximately 4 weeks). The hypothesis was that de-escalated treatment would result in less weight loss, which served as a quantitative surrogate for the severity of mucositis. Secondary outcome measures included disease Recurrence Rate, Progression Free Survival (PFS) and Overall Survival (OS).
It was noted that the de-escalated treatment resulted in significantly less weight loss. Specifically, the mean percent weight loss during de-escalated postoperative adjuvant chemoradiotherapy (Group 1) was 4.9%, compared to 7.4% in a historical cohort treated with conventional therapy (P=0.0003). For de-escalated radiotherapy alone (Group 2), the mean percent weight loss was 3.18%. The follow-up data of this study at a median of 50 months indicated low recurrence rates: 10% in Group 1 and 3.3% in Group 2. The 4-year PFS rates were 90.0% for Group 1 and 90.1% for Group 2, with OS rates of 100% and 94%, respectively. These results suggest that reduced radiation doses do not compromise the efficacy of treatment for patients with HPV-positive Oropharyngeal Squamous Cell Carcinoma.
Study by University of Michigan: FDG-PET-Guided Deintensification
The second study is a Phase II trial which enrolled 89 patients with Stage I–II HPV-positive Oropharyngeal Squamous Cell Carcinoma confirmed to have FDG-PET avidity. The treatment plan included an initial course of 70 Gy to gross disease and 56 Gy to elective nodal regions, administered concurrently with Carboplatin and Paclitaxel. Mid-treatment FDG-PET assessments were performed to evaluate metabolic tumor volume reduction. Patients with at least a 50% reduction in tumor volume had their radiotherapy de-escalated to 54 Gy, whereas the others completed the entire course of 70 Gy. The Primary endpoint was noninferiority of 2-year locoregional recurrence in the entire cohort, compared with an institutional historical control.
At a median follow-up of 32 months, the 2-year locoregional recurrence rate for the entire cohort was 6.8%. Patients continuing with the standard 70 Gy therapy had a 2-year locoregional recurrence rate of 4.6%, while those de-escalated to 54 Gy had a rate of 9.4%. These figures translate to two and three locoregional recurrences, respectively, which suggests overlapping confidence intervals and precludes definitive comparisons between the cohorts. The study also assessed other endpoints such as weight loss, swallowing function, and quality of life. Patients in the de-escalated group experienced significantly less weight loss (11 lbs versus 23 lbs in the standard-treatment group, P=0.001), and showed better maintenance of swallowing function and quality of life. The authors concluded that FDG-PET may be a reliable predictive biomarker to selectively de-escalate the radiation dose in early-stage HPV-positive disease.
The findings from these two studies underscore the feasibility and potential benefits of de-escalating radiotherapy in HPV-positive Oropharyngeal Squamous Cell Carcinoma. By tailoring treatment intensity, based on individual patient risk profiles and early responses to therapy, clinicians can achieve effective disease control while minimizing the severe side effects traditionally associated with high-dose radiation. This shift towards personalized, less intensive treatment protocols promises to enhance the quality of life and long-term outcomes for patients with this particular subset of Head and Neck cancers.
1. Long-term efficacy of risk-directed, de-escalated post-operative adjuvant therapy for surgically resected locally advanced, human papillomavirus-positive oropharynx squamous-cell carcinoma: A non-randomized, multi-arm phase 2 trial. Thorstad WL, Jackson RS, Oppelt P, et al.: 2024 Multidisciplinary Head and Neck Cancers Symposium. Abstract 14. Presented March 1, 2024.
2. FDG-PET-based selective de-escalation of radiotherapy for HPV-related oropharynx cancer: Results from a phase II trial. Regan SN, Rosen BS, Suresh K, et al.: 2024 Multidisciplinary Head and Neck Cancers Symposium. Abstract 16. Presented March 1, 2024.
Late Breaking Abstract – ESMO 2022: Neoadjuvant KEYTRUDA® with Chemoradiation in Locally Advanced Head and Neck Squamous Cell Carcinoma
SUMMARY: The American Cancer Society estimates that in the US for 2022, about 54,000 new cases of oral cavity or oropharyngeal cancer will be diagnosed and about 11,230 patients will die of the disease. Patients with Squamous Cell Carcinoma of the head and neck, frequently present with locoregionally advanced disease.
The treatment paradigm for Head and Neck cancer has been rapidly evolving with the recognition and better understanding of immune evasion and the role of immune checkpoints or gate keepers in suppressing antitumor immunity. Blocking the immune checkpoints unleashes the T cells, resulting in T cell proliferation, activation, and a therapeutic response. Checkpoint inhibitors administered in a neoadjuvant setting activates both the priming phase of immunity within tumor tissue, and the effector phase within the tumor microenvironment. It has been shown that neoadjuvant immunotherapy expands more T-cell clones than adjuvant treatment. Preclinical models have also demonstrated that both radiation therapy and Cisplatin chemotherapy increase the PD-L1 expression on the tumor, suggesting that combining radiotherapy with anti-PD-1 therapy could improve the outcomes.
Pembrolizumab (KEYTRUDA®) is a fully humanized, Immunoglobulin G4, monoclonal antibody and checkpoint inhibitor, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. Pembrolizumab has been shown to improve Overall Survival in patients with Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma
KEYNOTE-412 is a randomized, double-blind, Phase III trial, conducted to evaluate the efficacy and safety of Pembrolizumab in combination with chemoradiation versus placebo in combination with chemoradiation, in treatment naïve patients with locally advanced Head and Neck Squamous Cell carcinoma. In this study, 804 patients were randomly assigned 1:1 to receive Pembrolizumab 200 mg IV every 3 weeks plus chemoradiation (70Gy in 35 fractions along with Cisplatin 100 mg/m2 IV every 3 weeks) followed by Pembrolizumab (N=402), or placebo every 3 weeks plus chemoradiation, followed by placebo (N=402). Patients received Pembrolizumab /placebo priming dose 1 week before chemoradiation, followed by 2 doses during chemoradiation and 14 doses of maintenance therapy after chemoradiation, for a total of 17 doses. Enrolled patients had newly diagnosed, pathologically proven, treatment naive locally advanced Head and Neck Squamous Cell carcinoma (T3-T4, N0-N3 or any N2a-3, T1-T4 larynx/hypopharynx/oral cavity/p16-negative oropharynx cancers, or T4 or N3 p16-positive oropharynx cancer). Both treatment groups were well balanced. The Primary endpoint was Event Free Survival (EFS). Secondary endpoints included Overall Survival (OS), and Safety.
At the time of data cutoff, with a median follow up of 47.7 months, there was a favorable trend toward improved Event Free Survival (EFS) with the addition of Pembrolizumab vs placebo to chemoradiation (HR 0.83, P=0.04), but the difference did not achieve statistical significance. The 2-year EFS was 63.2% in the Pembrolizumab group and 56.2% in the placebo group. In an exploratory analysis however, the 2-year EFS among patients with high expression of PD-L1 (CPS 20 or higher) was 71% in the Pembrolizumab group and 62% in the placebo group. A favorable of Overall Survival benefit was also observed among these patients, with a 3-year OS of 79% in Pembrolizumab group and 73% in the placebo group.
It was concluded that Pembrolizumab in combination with chemoradiation was associated with a favorable trend toward improved Event Free Survival, compared with placebo plus chemoradiation, in patients with locally advanced Head and Neck Squamous Cell carcinoma, but the difference did not reach statistical significance. The researchers added that perhaps patients with high CPS score on the tumor could benefit with this treatment approach.
Primary results of the phase III KEYNOTE-412 study: Pembrolizumab (pembro) with chemoradiation therapy (CRT) vs placebo plus CRT for locally advanced (LA) head and neck squamous cell carcinoma (HNSCC). Machiels J, Tao Y, Burtness B, et al. Annals of Oncology (2022) 33 (suppl_7): S808-S869. 10.1016/annonc/annonc1089. LBA5
Late Breaking Abstract – ASCO 2022: Docetaxel as Radiosensitizer Improves Overall Survival in Cisplatin-Ineligible Head and Neck cancer
SUMMARY: The American Cancer Society estimates that in the US for 2022, about 54,000 new cases of oral cavity or oropharyngeal cancer will be diagnosed and about 11,230 patients will die of the disease. Patients with squamous cell carcinoma of the head and neck, frequently present with locoregionally advanced disease. For patients in this setting, chemoradiotherapy is an effective non-surgical approach as primary treatment. Alternatively, chemoradiotherapy can be delivered as adjuvant therapy after a curative resection.
Cisplatin-based concurrent chemoradiation is generally accepted as the standard, definitive non-surgical and post-operative approach in selected patients with locoregionally advanced squamous cell carcinoma of the head and neck. This treatment can however be associated with substantial morbidity and lifelong toxicities. Cetuximab is an immunoglobulin G1 chimeric monoclonal antibody against Epidermal Growth Factor Receptor (EGFR), and the only approved targeted agent in locoregionally advanced squamous cell carcinoma of the head and neck. Cetuximab plus Radiotherapy significantly improved Overall Survival at 5 years, when compared with radiotherapy alone, in patients with locoregionally advanced squamous cell carcinoma of the head and neck (Lancet Oncol. 2010). Cetuximab plus Radiotherapy is therefore an important treatment option in this patient group. However, financial barriers make Cetuximab as a Cisplatin substitute, inaccessible to patients, in low and middle-income countries.
Docetaxel is a semisynthetic taxane that affects polymerized tubulin to promote microtubule formation and inhibit its disassembly. Docetaxel has been shown to have significant antitumor activity as a single agent in head and neck cancer, when given in the neoadjuvant setting. Docetaxel is also a potent radiosensitizer. The researchers evaluated Docetaxel as a radiosensitizer in this clinical trial.
The authors in this open-label, randomized, Phase III study enrolled 356 Cisplatin-ineligible patients with locally advanced head and neck squamous cell carcinoma, planned for treatment with radical or adjuvant chemoradiation. The patients were randomly assigned 1:1 to receive Radiation alone (N=176) or Radiation with concurrent Docetaxel 15 mg/m2 IV weekly for a maximum of 7 cycles (N=180). Both treatment groups were well balanced. The median age was 62 yrs, approximately 45% of patients had a ECOG Performance Status of 2, and reasons for Cisplatin ineligibility included low creatinine clearance (26%), and hearing loss (43%). Approximately 33% of patients had oral cavity cancer and about two-thirds of patients had Stage IVA disease. The FACT-G, and Head and Neck questionnaires were completed by patients at baseline, 6 months, 12 months and at 24 months. FACT-G (Functional Assessment of Cancer Therapy-G) is a 27-item questionnaire designed to measure four domains of Health-Related Quality of Life (HRQOL) in cancer patients, which includes physical, social, emotional, and functional well-being. The Primary endpoint was Disease Free Survival (DFS), and key Secondary endpoints included Overall Survival (OS), adverse events and Quality of Life.
It was noted that the 2-year DFS was 30.3% with Radiation alone versus 42% with Docetaxel plus Radiation Therapy (HR=0.67; P=0.002). Docetaxel plus Radiation Therapy also significantly improved Overall Survival. The median Overall Survival was 15.3 months with Radiation Therapy alone, versus 25.5 months in the Docetaxel plus Radiation Therapy group (P=0.035). The 2 -year Overall Survival was also significantly higher in the Docetaxel plus Radiation Therapy group and was 41.7% with Radiation Therapy alone, versus 50.8% in the Docetaxel plus Radiation Therapy group (HR=0.74; P=0.035). These survival outcomes were observed across all preplanned subgroups.
Grade 3 or above adverse events were seen in 58% of patients receiving Radiation Therapy alone and in 81.6% of patients receiving Docetaxel plus Radiation Therapy. The addition of Docetaxel to Radiation Therapy resulted in a higher incidence of Grade 3 and above mucositis (49.7% versus 22.2%; P<0.001), odynophagia (52.5% versus 33.5%; P<0.001) and dysphagia (49.7% versus 33%; P<0.002). The addition of Docetaxel however did not lead to a worsening of Quality of Life, including Trial Outcome Index and FACT-G scores at 6 months.
The authors concluded that the addition of Docetaxel to Radiation Therapy improved Disease Free Survival and Overall Survival, in Cisplatin-ineligible locally advanced head and neck squamous cell carcinoma, and provides an evidence based, financially more viable treatment option, for this patient group.
Results of phase 3 randomized trial for use of docetaxel as a radiosensitizer in patients with head and neck cancer unsuitable for cisplatin-based chemoradiation. Patil VM, Noronha V, Menon NS, et al. DOI: 10.1200/JCO.2022.40.17_suppl.LBA6003 Journal of Clinical Oncology 40, no. 17_suppl (June 10, 2022) LBA6003.
PET Response-Based Radiotherapy De-Escalation in p16 Positive Oropharyngeal Cancer
SUMMARY: The American Cancer Society estimates that about 54,000 new cases of oral cavity or Oropharyngeal Cancer will be diagnosed in the US in 2022 and about 11,230 patients will die of the disease. According to the CDC, based on data from 2014 to 2018, about 46,143 HPV-associated cancers occur in the United States each year (25,719 among women, and 20,424 among men). Cervical cancer is the most common HPV-associated cancer among women, and Oropharyngeal cancers are the most common among men. There has been a significant increase in the incidence during the past several decades, due to changes in sexual practices.
HPV-positive Oropharyngeal Squamous Cell Carcinoma (OPSCC) is an entirely distinct disease entity from HPV-negative Oropharyngeal Squamous Cell Carcinoma. Patients with HPV-positive OPSCC tend to be younger males, who are former smokers or nonsmokers, with risk factors for exposure to High Risk HPV (HR-HPV). The HPV-positive primary Squamous Cell Carcinoma tend to be smaller in size, with early nodal metastases, and these patients have a better prognosis compared with patients with HPV-negative Head and Neck Squamous Cell Carcinoma (HNSCC), when treated similarly. Expression of tumor suppressor protein, known as p16, is highly correlated with infection with HPV in HNSCC. Accurate HPV assessment in head and neck cancers is becoming important as it significantly impacts clinical management. HPV status is considered the most important prognostic indicator in patients with head and neck cancer and p16 status is now included in the American Joint Committee on Cancer (AJCC) Staging System.
HPV-positive Oropharyngeal Squamous Cell Carcinoma is more sensitive to chemotherapy and radiotherapy than is HPV-negative Oropharyngeal Squamous Cell Carcinoma, which translates to a much better prognosis and survival, when treated with a combination of Cisplatin chemotherapy and Radiotherapy. This treatment however can be associated with substantial morbidity and lifelong toxicities such as dry mouth, difficulty swallowing, and loss of taste.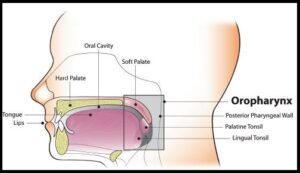
To address these toxicities, the authors conducted a prospective Phase II de-escalation study utilizing FDG-PET response criteria to select patients eligible for de-escalated radiotherapy. The researchers hypothesized that early swallow function and quality of life will improve with lower dose radiation. This study enrolled 59 patients (N=59) with Stage I-II (AJCC) p16-positive Oropharyngeal cancer, with FDG-avid disease and any smoking history. Patients with matted lymph nodes or history of head and neck surgery were excluded.
All enrolled patients had a pre-treatment FDG-PET/CT imaging and received weekly Carboplatin and Paclitaxel concurrently with planned radiotherapy at 70 Gy in 35 fractions. FDG-PET was repeated midway through treatment after 2 weeks at fraction 10. Patients who had tumors with lower metabolic activity before treatment and more than 50% reduction in Metabolic Tumor Volume after 2 weeks of treatment were de-escalated from the standard radiotherapy total dose of 70 Gy in 35 fractions, to a total dose of 54 Gy in 27 fractions. The median patient age was 60 years and baseline characteristics showed that both standard and de-escalated cohorts had similar patient demographics and pathology. At the planned interim analysis, early toxicity and Patient Reported Outcomes (PROs) were examined.
Fifty percent (50%) of the patients met de-escalation criteria and received the lower radiation dose, leading to 20-30% reductions in radiation exposure to sensitive structures in the head and neck prone to toxicities such as larynx, constrictors, oral cavity and salivary glands. De-escalation from the standard radiotherapy resulted in significantly less acute toxicity, and at one month after treatment, patients who received de-escalated therapy lost less weight as a percentage of baseline, compared to standard treatment group (6% versus 11%; P<0.001) and had improved videofluoroscopic swallowing function following treatment, and fewer patients required feeding tube placement during treatment.
The authors concluded that although the trial remains ongoing, mid-treatment FDG-PET response adaptation allows for approximately 50% of early stage p16 positive Oropharyngeal cancer patients to be de-escalated to a total dose of 54 Gy. This in turn can result in approximately 25% reduction in dose delivered to organs known to affect toxicity and quality of life, with significantly better objective measures of toxicity and numerically improved Patient Related Outcomes.
Early Toxicity and Patient Reported Outcomes From a Phase 2 Trial of FDG-PET Response-Based De-Escalated Definitive Radiotherapy for p16+ Oropharynx Cancer. Allen SG, Rosen BS, Aryal MP, et al. 2022 Multidisciplinary Head and Neck Symposium; February 24-26, 2022; Phoenix, AZ. Abstract 1.