
The FDA on July 17, 2017 approved NERLYNX ® for the extended adjuvant treatment of adult patients with early stage HER2-overexpressed/amplified breast cancer, to follow adjuvant Trastuzumab-based therapy. NERLYNX ® is a product of Puma Biotechnology, Inc.
Tag: Breast Cancer
Weight Gain Increases the Risk for Postmenopausal Breast cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 255,180 new cases of invasive breast cancer will be diagnosed in 2017 and over 41,070 women will die of the disease. Obesity is an important contributing factor to postmenopausal breast cancer incidence and mortality. Based on recently published meta-analysis, in women diagnosed with breast cancer, there is an approximately 30% increased risk of disease recurrence or death in those who are obese compared to those with ideal body weight. Increasing physical activity may lower the risk of breast cancer recurrence. According to the consensus from the St Gallen Consensus Conference in 2015, obesity has been associated with poor breast cancer outcomes. Obesity is associated with alterations in insulin/glucose homeostasis, adipokines, and sex hormones, which may play a role in breast cancer outcomes. Weight loss can lead to reductions in C-reactive protein, insulin, glucose, and leptin. These mediators have all been implicated to have prognostic significance in breast cancer. 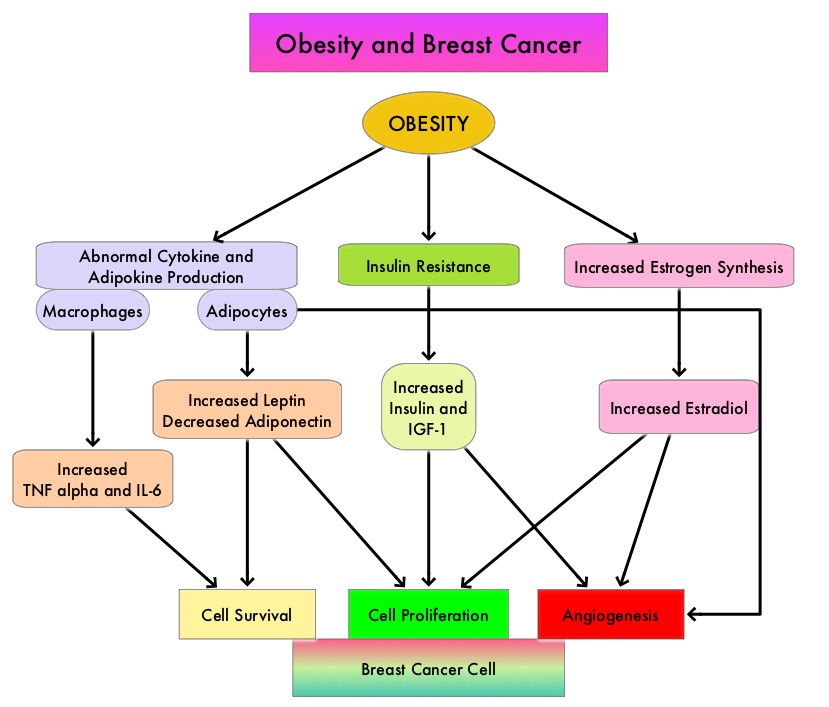
The Nurses’ Health Studies (NHS) are the largest and longest running investigations focused on women’s health. This was established in 1976 and the information provided by its 238,000 dedicated nurse-participants has allowed NHS to produce key advances impacting women’s health. These studies are conducted by researchers at Harvard School of Public Health and Brigham and Women's Hospital in Boston, Massachusetts. The authors conducted a clinical trial in this NHS cohort and studied the effects of weight and weight changes in early adulthood and risk of breast cancer later in life. A prospective observational study was conducted among 74,177 women from the Nurses' Health Study from 1980-2012. These women provided information on breast cancer risk factors such as reproductive factors, hormone therapy, anthropometric variable, benign breast disease, and family history of breast cancer. This information was updated every 2 years up to the time of data analysis. Each individual’s weight at age 18 was collected in 1980.
During the observation period, 4965 cases of invasive breast cancer were reported for the 74,177 women followed from 1980 to 2012. Weight gain over a long period of time from age 18, both during premenopause and postmenopause, were positively associated with postmenopausal breast cancer risk. However, premenopausal weight gain was not related to premenopausal breast cancer risk. Further, weight gain from age 18 yrs onwards was positively associated with ER+/PR+ postmenopausal breast cancer and there was a 50% increased risk for breast cancer with a weight gain of 30 kg. This direct association was not seen for ER+/PR- or ER-/PR- breast cancer. The authors noted that overall, 17% of ER+/PR+ postmenopausal breast cancer and 14% of total postmenopausal breast cancer are attributable to weight gain of more than 5 kg after age 18.
It was concluded that 14% of postmenopausal breast cancer could be prevented if women avoided excessive weight gain of more than 5 kg after age 18. This study adds new insights on weight gain during premenopausal years and risk for postmenopausal breast cancer. Weight and weight changes in early adulthood and later breast cancer risk. Rosner B, Eliassen AH, Toriola AT, et al. Int J Cancer. 2017 Jan 30. doi: 10.1002/ijc.30627 [Epub ahead of print]
Late Breaking Abstract – ASCO 2017 Adjuvant Dual HER2 Regimen of PERJETA® and HERCEPTIN® Improves Outcomes in Early Stage Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 255,180 new cases of invasive breast cancer will be diagnosed in 2017 and over 41,070 women will die of the disease. The HER or erbB family of receptors consist of HER1, HER2, HER3 and HER4. Approximately 15%-20% of invasive breast cancers overexpress HER2/neu oncogene, which is a negative predictor of outcomes without systemic therapy. HERCEPTIN® (Trastuzumab) is a humanized monoclonal antibody targeting HER2. Trastuzumab binds to subdomain IV of the HER2 extracellular domain and blocks the downstream cell signaling pathways (PI3K-AKT pathway) and induces Antibody Dependent Cellular Cytotoxicity (ADCC). Adjuvant chemotherapy given along with HERCEPTIN® reduces the risk of disease recurrence and death, among patients with HER2-positive early breast cancer.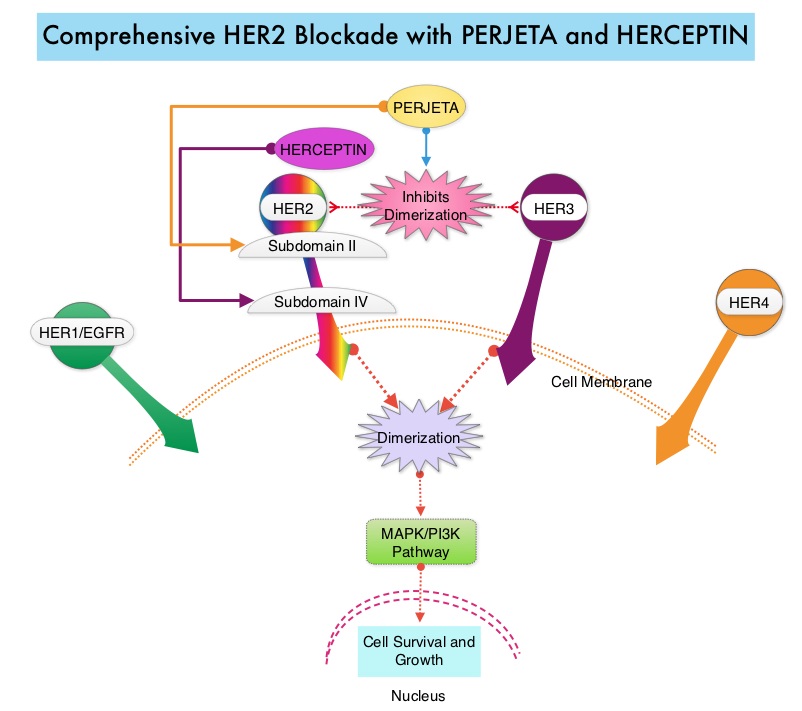
PERJETA® (Pertuzumab) is a recombinant humanized monoclonal antibody that binds to the HER2 at a different epitope of the HER2 extracellular domain (subdomain II) compared to HERCEPTIN® and prevents the dimerization of HER2 with HER3 receptor. PERJETA® induces ADCC similar to HERCEPTIN®. By combining HERCEPTIN® and PERJETA®, a more comprehensive blockade of HER2 signaling can be accomplished, as these two agents bind to different HER2 epitopes and may complement each other and improve efficacy. In the CLEOPATRA study, the addition of PERJETA® to HERCEPTIN® and Docetaxel resulted in significant improvement in Progression Free Survival (PFS) and Overall Survival (OS), in patients with HER-positive metastatic breast cancer. This triple drug combination also resulted in a significantly increased pathological Complete Response rate, when given in a neoadjuvant setting (NeoSphere trial).
Based on these previously published efficacy data, the authors in this study investigated whether the addition of PERJETA® to adjuvant HERCEPTIN® and chemotherapy, improves outcomes, among patients with HER2-positive early breast cancer. APHINITY is a prospective, randomized, multicenter, multinational, double-blind, placebo-controlled phase III trial in which a total of 4805 patients were randomly assigned in a 1:1 ratio, to receive standard adjuvant anthracycline or non-anthracycline chemotherapy regimen along with HERCEPTIN® plus either PERJETA® (2400 patients) or placebo (2405 patients). Anti-HER2 therapy was administered for a total of 1 year. Patients could receive radiotherapy and/or endocrine therapy following completion of adjuvant chemotherapy. Eligible patients had node-positive or high-risk node-negative (tumor diameter greater than 1.0 cm), HER2-positive, non-metastatic, adequately excised breast cancer. Both treatment groups were well balanced and about 37% of the patients had 1-3 positive lymph nodes and 25% of the patients had 4 or more positive lymph nodes. Two thirds of the patients were hormone receptor positive and about 78% of the patients received an anthracycline containing adjuvant chemotherapy regimen. The median follow up was 45.4 months and one year of treatment was completed by approximately 85% of the patients in both treatment groups. The primary end point was Disease Free Survival (DFS) from invasive breast cancer and secondary end points included Overall Survival (OS) and DFS from non-invasive breast cancers.
The addition of PERJETA® to chemotherapy and HERCEPTIN® resulted in a higher rate of DFS for invasive breast cancer with a 3-year invasive DFS of 94.1% in the PERJETA® group and 93.2% in the placebo group (HR=0.81; P=0.045), in favor of PERJETA®. Patients in the high risk subgroups benefited the most. The 3-year invasive DFS for patients with node-positive disease was 92.0% in the PERJETA® group, compared with 90.2% in the placebo group (HR=0.77; P=0.02). In the cohort of patients with hormone receptor negative tumors, the 3-year invasive DFS was 92.8% in the PERJETA® group and 91.2% in the placebo group (HR=0.76; P=0.08). The site of first distant recurrence was visceral or in the CNS rather than the bone. Cardiac toxicities were uncommon in both treatment groups and patients in the PERJETA® group had higher incidence of diarrhea while on concurrent chemotherapy.
It was concluded that for patients with HER2-positive early breast cancer, the addition of PERJETA® to standard postoperative HERCEPTIN® based adjuvant chemotherapy, significantly improved Disease Free Survival for invasive breast cancer. This benefit was more so for those patients with high risk disease. APHINITY trial (BIG 4-11): A randomized comparison of chemotherapy (C) plus trastuzumab (T) plus placebo (Pla) versus chemotherapy plus trastuzumab (T) plus pertuzumab (P) as adjuvant therapy in patients (pts) with HER2-positive early breast cancer (EBC). von Minckwitz G, Procter MJ, De Azambuja E, et al. J Clin Oncol. 2017;35(suppl; abstr LBA500).
Late Breaking Abstract – ASCO 2017 LYNPARZA® Improves Progression Free Survival in BRCA Positive Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 255,180 new cases of invasive breast cancer will be diagnosed in 2017 and over 41,070 women will die of the disease. DNA can be damaged due to errors during its replication or as a result of environmental exposure to ultraviolet radiation from the sun or other toxins. The tumor suppressor genes such as BRCA1 (Breast Cancer 1) and BRCA2 help repair damaged DNA and thus play an important role in maintaining cellular genetic integrity, failing which these genetic aberrations can result in malignancies. The BRCA1 gene is located on the long (q) arm of chromosome 17 whereas BRCA2 is located on the long arm of chromosome 13. Mutations in BRCA1 and BRCA2 account for about 20 to 25 percent of hereditary breast cancers and about 5 to 10 percent of all breast cancers. These mutations can be inherited from either of the parents and a child has a 50 percent chance of inheriting this mutation and the deleterious effects of the mutations are seen even when an individual’s second copy of the gene is normal. 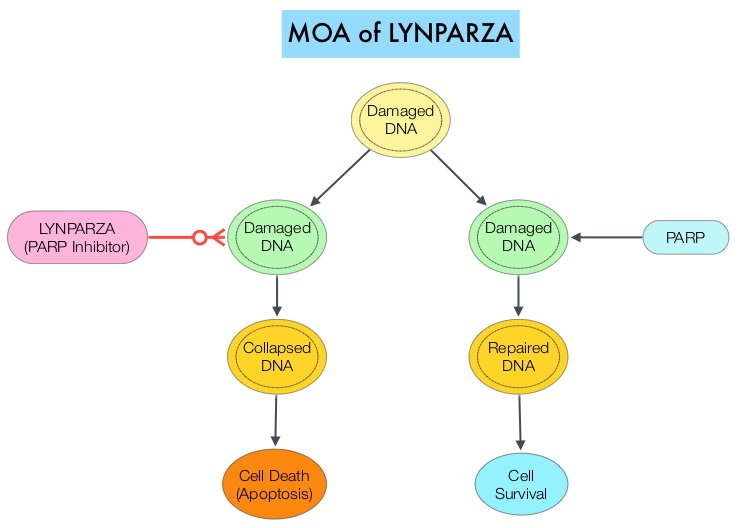
The PARP (Poly ADP Ribose Polymerase) family of enzymes which include PARP1 and PARP2, repair damaged DNA. LYNPARZA® (Olaparib) is a PARP enzyme inhibitor that causes cell death in tumors that already have a DNA repair defect, such as those with BRCA1 and BRCA2 mutations. The FDA approved LYNPARZA® (Olaparib) in 2014 as monotherapy for the treatment of patients with deleterious or suspected deleterious germline BRCA mutated advanced ovarian cancer.
OlympiAD is a randomized, open-label, phase III study that evaluated the efficacy and safety of LYNPARZA® (Olaparib) compared with physician’s choice of standard single agent chemotherapy (TPC), in patients with HER2-negative metastatic breast cancer, with inherited, germline BRCA mutations. In this study, 302 patients were randomized in a 2:1 ratio to receive LYNPARZA® tablets 300 mg PO BID (N=205) or physician’s choice of standard chemotherapy (N=97). The later included 21-day cycles of either XELODA® (Capecitabine) 2500 mg/m2 orally on days 1-14, NAVELBINE® (Vinorelbine) 30 mg/m2 IV days 1 and 8 or HALAVEN® (Eribulin)1.4 mg/m2 IV days 1 and 8. Treatment was continued until disease progression or unacceptable toxicity. The median age was 44 years, 50% of the patients had triple negative disease, 71% of the patients had prior chemotherapy for metastatic breast cancer, 28% had prior platinum based chemotherapy regimen and those with hormone receptor positive breast cancer had received hormonal therapy. The primary endpoint was Progression Free Survival (PFS). Secondary endpoints included Overall Survival, time to second progression or death, Objective Response Rate and effect on health-related Quality of Life.
At a median follow up of about 14 months, the median PFS was 7 months in the LYNPARZA® group versus 4.2 months with standard chemotherapy (HR=0.58; P=0.0009), suggesting a 42% reduced risk of cancer progression in the LYNPARZA® group compared to those who received chemotherapy. Following disease progression, the time to second progression (which meant duration of time before the cancer worsened again), was also longer in the LYNPARZA® group (HR 0.57), suggesting that recurrent disease was not more aggressive following progression on LYNPARZA®. The Objective Response Rate was 60% and 29% in LYNPARZA® and chemotherapy group respectively. Severe side effects were more common in chemotherapy treated patients (50%) compared with LYNPARZA® group (37%). The most common side effects in the LYNPARZA® group included nausea, fatigue and cytopenias, where as rash on hands and feet were most common in the chemotherapy group.
The authors concluded that LYNPARZA® monotherapy significantly improved Progression Free Survival in HER2-negative metastatic breast cancer patients, with inherited germline BRCA mutations, compared to standard chemotherapy. This “proof of the principle” study demonstrated that breast cancers with defects in a specific DNA damage repair pathway are sensitive to targeted therapy and this is the first of several phase III studies with PARP inhibitors that are underway. OlympiAD: Phase III trial of olaparib monotherapy versus chemotherapy for patients (pts) with HER2-negative metastatic breast cancer (mBC) and a germline BRCA mutation (gBRCAm). Robson ME, Im S-A, Senkus E, et al. J Clin Oncol 35, 2017 (suppl; abstr LBA4).
Final Overall Survival Results with KADCYLA® in Metastatic Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 255,180 new cases of invasive breast cancer will be diagnosed in 2017 and over 41,070 women will die of the disease. The HER or erbB family of receptors consist of HER1, HER2, HER3 and HER4. Approximately 15%-20% of invasive breast cancers overexpress HER2/neu oncogene, which is a negative predictor of outcomes without systemic therapy. HERCEPTIN® (Trastuzumab) is a humanized monoclonal antibody targeting HER2. It binds to the extracellular domain of the receptor and blocks the downstream cell signaling pathways (PI3K-AKT pathway) and induces Antibody Dependent Cellular Cytotoxicity (ADCC). HERCEPTIN® in combination with chemotherapy has been proven to significantly improve Progression Free Survival and Overall Survival in patients with advanced breast cancer. Despite this benefit, majority of these patients develop progressive disease within 18 months. The tumors in these patients continue to express HER2 although the lower sensitivity to HER2 targeted agents has been attributed to HER2 independent escape mechanisms. Treatment strategies for this patient population have included switching chemotherapy in subsequent lines of treatment and continuing HERCEPTIN®, combining another HER2 targeted agent, Lapatinib (TYKERB®) with Capecitabine (XELODA®) and dual HER2 inhibition with a combination of HERCEPTIN® and TYKERB®.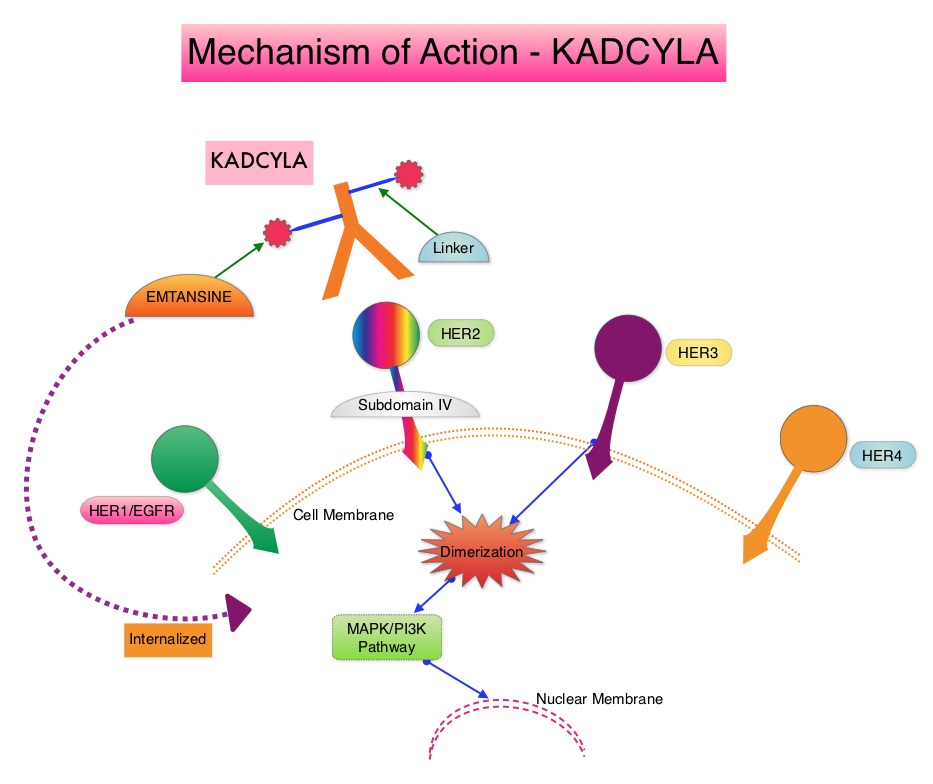
KADCYLA® (Ado-Trastuzumab Emtansine, T-DM1) is an Antibody-Drug Conjugate (ADC) comprised of the antibody HERCEPTIN® and the chemotherapy agent Emtansine, linked together. Upon binding to the HER2 receptor, it not only inhibits the HER2 signaling pathways but also delivers a chemotherapy agent Emtansine, a microtubule inhibitor, directly inside the tumor cells. This agent is internalized by lysosomes and destroys the HER2-positive tumor cells upon intracellular release. In the EMILIA trial, KADCYLA® was associated with significant increase in Overall Survival when compared with TYKERB® plus XELODA®, in HER2-positive metastatic breast cancer patients, who had previously received HERCEPTIN® and a taxane.
TH3RESA is an open label randomized phase III trial in which KADCYLA® was compared with treatment of physician’s choice, in patients with unresectable locally advanced, recurrent or metastatic breast cancer. Eligible patients had a left ventricular ejection fraction of 50% or more and had HER2-positive advanced breast cancer and had received two or more HER2-directed regimens in the advanced setting, and had progressed on both HERCEPTIN® and TYKERB® containing regimens in metastatic setting, and also had disease progression on a taxane, in any setting. Patients were randomized in a 2:1 ratio to receive either KADCYLA® 3.6 mg/kg IV every 21 days (N=404) or treatment of physician’s choice (N=198), which included HER2 directed therapy for the majority of patients. Treatment was continued until disease progression or unmanageable toxicity. The Co-primary endpoints were Progression Free Survival (PFS) and Overall Survival (OS). Secondary endpoints included Response Rates, Duration of Response, Safety and Quality of Life. The authors had previously reported a significant improvement in PFS with KADCYLA® compared with physician's treatment choice (6.2 months vs 3.3 months, HR= 0.528, P<0.0001) and an OS trend favoring KADCYLA®.
The authors now reported the results from the final Overall Survival analysis of the TH3RESA trial. At data cutoff, 47% of the patients in the physician's choice group had crossed over to KADCYLA®. The Overall Survival was significantly longer with KADCYLA® compared with treatment of physician's choice (median 22.7 months versus 15.8 months, HR=0.68, P=0.0007). This benefit was seen in all pre-specified subgroups. Patients in the KADCYLA® group had a lower incidence of grade 3 toxicities compared to the patients in the physician’s treatment choice group (40% vs 47%). Grade 3 thrombocytopenia however was more common in the KADCYLA® group compared to the physician’s choice group (6% vs 3%) and this has been attributed to the inhibition of megakaryocyte differentiation by KADCYLA®.
The authors concluded that for patients who had progressed on two or more HER2-directed regimens, treatment with KADCYLA® significantly improved Overall Survival, compared with treatment of physician's choice, thereby validating HER2 as a therapeutic target, even after multiple lines of previous therapy. Trastuzumab emtansine versus treatment of physician's choice in patients with previously treated HER2-positive metastatic breast cancer (TH3RESA): final overall survival results from a randomised open-label phase 3 trial. Krop IE, Kim SB, González-Martín A, et al. Lancet Oncol. DOI: http://dx.doi.org/10.1016/S1470-2045(17)30313-3
Late Breaking Abstract – ECCO 2017 Breast Conserving Therapy Better Than Mastectomy in Some Patients with Early Stage Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 255,180 new cases of invasive breast cancer will be diagnosed in 2017 and over 41,070 women will die of the disease. The National Surgical Adjuvant Breast and Bowel Project (NASBP) protocols B-04 and B-06 have clearly established after more than a 2 decades of evaluation and follow up that, in Stage I and II breast cancer, there is no significant difference in either distant Disease Free or Overall Survival between the Breast Conserving Therapy (BCT) and Breast Removal Surgery (Mastectomy). This data established Breast Conserving Therapy (BCT) as the preferred local-regional procedure. These trials however often excluded elderly patients or patients with co-morbidities. Radiotherapy after breast- conserving surgery significantly decreases the risk of local recurrence and improves Breast Cancer Specific Survival (BCSS) in certain subgroups of patients. According to the American Cancer Society, 42% of all invasive breast cancers in the US occur in women 65 years of age or older. These patients may have associated co-morbidities and may therefore be appropriate candidates for breast- conserving surgery rather than mastectomy. These patients also have better outcomes, as post-op recovery time is shorter. There is however limited data to confirm these findings, as most studies evaluated limited numbers of patients, lacked long term follow up and the cause of death in these patients could not be clearly determined.
To further address this question, the authors in this study compared breast-conserving surgery plus radiation therapy (BCT) with Mastectomy, for Breast Cancer Specific (BCSS) and Overall Survival (OS), in a population-based study of 129,692 breast cancer patients without metastatic disease, in the Netherlands. Patients were selected from the Netherlands Cancer Registry, who had T1-2, N0-2, M0 breast cancer, diagnosed between1999 and 2012. Patients were divided into two time cohorts: those diagnosed between 1999 and 2005 (long term follow up), and those diagnosed between 2006 and 2012, (contemporary adjuvant systemic therapy). The influence of prognostic factors such as age, stage, adjuvant systemic therapy, hormonal and HER2 receptor status and co-morbidities was studied in these two groups of patients, in order to identify possible prognostic factors, that might predict patient groups, who could benefit the most from Breast Conserving Therapy (BCT). Information on the cause of death was obtained from Statistics Netherlands, also known as the Dutch Central Bureau of Statistics.
It was noted that for patients in the long-term follow up cohort, Breast Conservation Therapy was associated with a statistically significant improvement in Breast Cancer Specific Survival and Overall Survival compared to Mastectomy in all T1-2, N0-2 stages. For patients diagnosed between 2006 to 2012 (contemporary adjuvant systemic therapy), Breast Conserving Therapy was again associated with a statistically significant improvement in Breast Cancer Specific Survival and Overall Survival for patients in the T1-2, N0-1 stage but not those with T1-2, N2 disease, and in this later group, Breast Cancer Specific Survival (BCSS) with conservation therapy was equal to that with mastectomy. Subgroup analyses in the T1-2, N0-1 subset showed superior BCSS with breast conservation in patients older than 50 years, those who did not receive chemotherapy and those who had co-morbid conditions, irrespective of hormone receptor or HER2 status. The Overall Survival (OS) results were similar. Among patients younger than 50 years of age without co-morbidities, and those who received chemotherapy, BCSS with breast conservation was equal to that with mastectomy, but OS was better with Breast Conservation Therapy than with Mastectomy.
It was concluded that in this large population of “real world” patients as seen in daily clinical practice, Breast Conserving Therapy is associated with superior Breast Cancer-Specific and Overall Survival when compared to Mastectomy in patients over 50 years of age, T1-2, N0-1 M0 stage, patients who had not received chemotherapy and patients with co-morbidities. This benefit was confirmed for patients in both time cohorts. This study information allows the Health Care Provider to decide which type of surgical treatment is best suited for some subtypes of Breast cancer. Breast conserving therapy and mastectomy revisited: Breast cancer-specific survival and the influence of prognostic factors in 129,692 patients. Lagendijk M, van Maaren MC, Saadatmand S, et al. ECCO2017 European Cancer Congress. Abstract number: 4LBA
IBRANCE® (Palbociclib)
The FDA on March 31, 2017 granted regular approval to IBRANCE® for the treatment of Hormone Receptor (HR) positive, Human Epidermal growth factor Receptor 2 (HER2) negative advanced or metastatic breast cancer, in combination with an Aromatase Inhibitor, as initial endocrine based therapy in postmenopausal women. IBRANCE® is marketed by Pfizer Inc.
Use of Adjuvant Bisphosphonates and Other Bone-Modifying Agents in Breast Cancer A Cancer Care Ontario and American Society of Clinical Oncology Clinical Practice Guideline
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop breast cancer during their life time. Approximately, 255,180 new cases of breast cancer will be diagnosed in 2017 and 41,070 women will die of the disease. Cancer Care Ontario and ASCO convened a Working Group and Expert Panel and following a systematic review of the literature, developed evidence-based recommendations regarding the use of bisphosphonates and other bone-modifying agents, as adjuvant therapy, for patients with breast cancer. These guidelines are based on several important findings noted in previously published studies and in the more recently published Oxford Overview (Early Breast Cancer Trialists’ Collaborative Group) analysis of individual patient data.
1) Adjuvant bisphosphonates were found to reduce bone recurrence and improve survival in postmenopausal patients with non-metastatic breast cancer (including those with natural menopause or menopause induced by ovarian suppression or ablation)
2) The absolute benefit with adjuvant bisphosphonates was greater in patients who were at a higher risk of recurrence, and almost all clinical trials were conducted in patients who also received systemic therapy.
3) Most studies evaluated ZOMETA® (Zoledronic acid) or BONEFOS® (Clodronate), and there was extremely limited data for other bisphosphonates. Although XGEVA® (Denosumab) was found to reduce fractures, long-term survival data is awaited.
The following is a summary of the panel’s recommendations:
Recommendation 1
a) Administration of bisphosphonates as adjuvant therapy should be considered for postmenopausal patients with breast cancer (including patients who are premenopausal before treatment and have menopause induced by ovarian suppression as detailed in Recommendation 5) deemed candidates for adjuvant systemic therapy.
b) The final decision of whether or not to administer bisphosphonates should be made during consultation between the patient and oncologist, taking into account patient and disease characteristics, including the risk of recurrence, and weighing the potential benefits and risks.
Recommendation 2
a) Zoledronic acid and Clodronate are the recommended bisphosphonates for adjuvant therapy in breast cancer.
b) There is a need for more information comparing different agents and schedules, and it is recommended that such trials be conducted to establish the utility and optimal administration of other bisphosphonates for adjuvant therapy.
Recommendation 3
a) There is insufficient evidence at this time to make any recommendation regarding the use of Denosumab in the adjuvant setting.
b) It is recommended that studies directly comparing Denosumab with bisphosphonates and evaluating administration schedules, be conducted.
Recommendation 4
a) For patients who will receive adjuvant bisphosphonates (Recommendation 1), Zoledronic acid 4 mg IV over 15 minutes (or longer) every 6 months for 3 to 5 years or Clodronate PO 1,600 mg daily for 2 to 3 years is recommended. Different durations may be considered.
b) More research is recommended comparing different bone-modifying agents, doses, dosing intervals, and durations.
Recommendation 5
For purposes of adjuvant bisphosphonate use, the definition of menopause should include natural menopause (at least 12 months of amenorrhea prior to initiation of chemotherapy or endocrine therapy) and menopause induced by ovarian ablation or suppression (but not the cessation of menses due to chemotherapy alone). In women aged 60 years or less with a previous hysterectomy and ovaries left in place, Luteinizing Hormone, Follicle Stimulating Hormone and Serum Estradiol should be in the postmenopausal range and measured prior to initiation of any systemic therapy, to receive adjuvant bisphosphonates.
Recommendation 6
a) A dental assessment is recommended prior to commencement of bisphosphonates, where feasible, and any pending dental or oral health problems should be dealt with prior to starting treatment, if possible. Patients should be informed of the risk of developing osteonecrosis of the jaw, especially with tooth extractions and other invasive dental procedures. Patients should inform their dental practitioner of their treatment. Patients with suspected osteonecrosis of the jaw should be referred to a dental practitioner with expertise in treating this condition. Recent guidelines or position papers by groups such as the International Task Force on Osteonecrosis of the Jaw, the American Association of Oral and Maxillofacial Surgeons, and the American Dental Association should be consulted.
b) Patients should have Serum Calcium measured prior to starting treatment. Patients receiving intravenous bisphosphonates (Zoledronic acid) should be monitored for renal function, prior to starting this treatment and for Serum Calcium and increase in Serum Creatinine, throughout the treatment period.
c) Calcium and vitamin D supplementation is recommended unless otherwise contraindicated. Oral bisphosphonates and Calcium should not be taken concurrently. Several monographs suggest an interval of at least 2 hours to allow for maximum absorption.
d) Symptoms such as ocular pain or loss of vision may be due to serious inflammatory conditions such as uveitis or scleritis and should be promptly evaluated by an ophthalmologist.
Use of Adjuvant Bisphosphonates and Other Bone-Modifying Agents in Breast Cancer: A Cancer Care Ontario and American Society of Clinical Oncology Clinical Practice Guideline. Dhesy-Thind S, Fletcher GG, Blanchette PS, et al. DOI: 10.1200/JCO.2016.70.7257 Journal of Clinical Oncology – published online before print March 6, 2017
FDA Approves KISQALI® for First-Line Treatment of Hormone Receptor Positive Advanced Breast cancer
SUMMARY: The FDA on March 13, 2017 approved KISQALI® (Ribociclib), a cyclin-dependent kinase 4/6 inhibitor, in combination with an Aromatase Inhibitor, as initial endocrine-based therapy for the treatment of postmenopausal women with Hormone Receptor (HR)-positive, Human Epidermal growth factor Receptor 2 (HER2)-negative advanced or metastatic breast cancer. Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop breast cancer during their life time. Approximately, 255,180 new cases of breast cancer will be diagnosed in 2017 and 41,070 women will die of the disease. Approximately 70% of breast tumors express Estrogen Receptors and/or Progesterone Receptors and these patients are often treated with anti-estrogen therapy as first line treatment. However, resistance to hormonal therapy occurs in a majority of the patients.
Cyclin Dependent Kinases (CDK) play a very important role to facilitate orderly and controlled progression of the cell cycle. Genetic alterations in these kinases and their regulatory proteins have been implicated in various malignancies. Cyclin Dependent Kinases 4 and 6 (CDK4 and CDK6), phosphorylate RetinoBlastoma protein (RB), and initiate transition from the G1 phase to the S phase of the cell cycle. RetinoBlastoma protein has antiproliferative and tumor-suppressor activity and phosphorylation of RB protein nullifies its beneficial activities. CDK4 and CDK6 are activated in hormone receptor positive breast cancer, promoting breast cancer cell proliferation. Further, there is evidence to suggest that endocrine resistant breast cancer cell lines depend on CDK4 for cell proliferation. The understanding of the role of Cyclin Dependent Kinases in the cell cycle, has paved the way for the development of CDK inhibitors.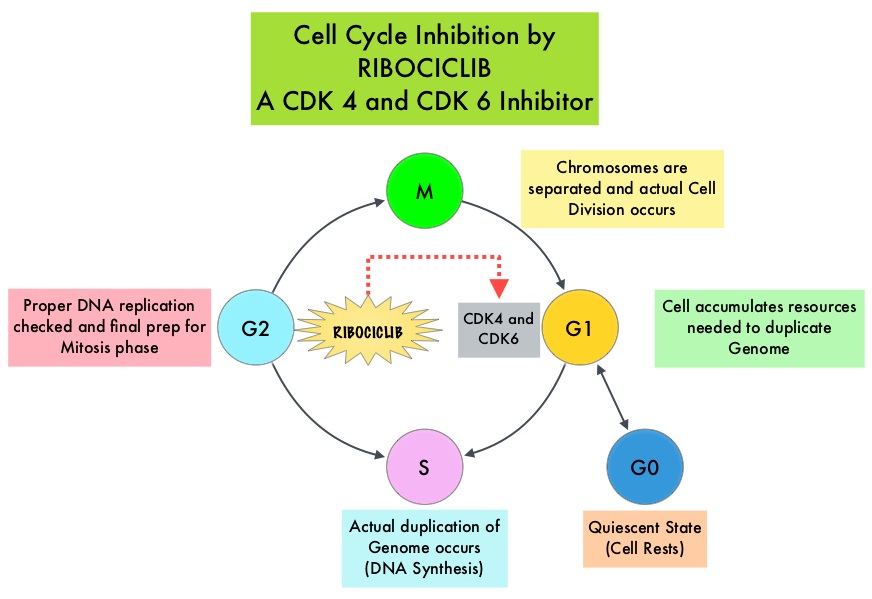
KISQALI® is an orally bioavailable, selective, small-molecule inhibitor of CDK4/6 that blocks the phosphorylation of RetinoBlastoma protein, thereby preventing cell-cycle progression and inducing G1 phase arrest. In a phase 1b study involving postmenopausal women with ER positive, HER2-negative advanced breast cancer, KISQALI® in combination with FEMARA® (Letrozole) demonstrated an Overall Response Rate (ORR) of 46% and a Clinical Benefit Rate of 79%, in treatment-naïve patients with advanced breast cancer.
MONALEESA-2 trial is a randomized, double-blind, placebo-controlled, phase III study in which 668 patients were randomly assigned in a 1:1 ratio to receive either KISQALI® plus FEMARA® (Letrozole) or placebo plus FEMARA®. Eligible patients included post-menopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer who had received no prior therapy for advanced disease. Treatment consisted of oral KISQALI® 600 mg daily on a 3-weeks on and 1-week off schedule, in 28-day treatment cycles plus FEMARA® 2.5 mg orally daily on a continuous schedule or placebo plus FEMARA®. Patients were stratified according to the presence or absence of liver or lung metastases and treatment was continued until disease progression or unacceptable toxicity. No treatment crossover was allowed. The median age was 62 years and close to 60% of the patients had visceral metastases. The primary end point was Progression Free Survival (PFS) and secondary end points included Overall Survival (OS), Overall Response Rate (ORR), Clinical Benefit Rate (Overall Response plus stable disease lasting 24 weeks or more), safety, and Quality of Life assessments.
A pre-planned interim efficacy analysis demonstrated a significant improvement in the PFS amongst the KISQALI® group compared to the placebo group (HR=0.56; P<0.0001). The median duration of follow-up was 15.3 months. The estimated median PFS had not been reached in the KISQALI® group and was 14.7 months in the placebo containing arm. The Overall Response Rate (ORR) in patients with measurable disease was 52.7% in the KISQALI® group and 37.1% in the placebo plus FEMARA® group (P<0.001). Overall Survival data was mature at the time of this analysis. The rates of discontinuation because of adverse events were 7.5% in the KISQALI® group and 2.1% in the placebo group. The most common adverse reactions observed in patients taking KISQALI® were myelosuppression, nausea, vomiting, diarrhea and fatigue, as well as abnormal liver function tests. KISQALI® has been shown to prolong the QT interval in a dose-dependent manner and prolongation of the QT interval occurred in 3.3% of patients treated at the 600 mg dose, with changes mostly occurring within the first 4 weeks of treatment.
The authors concluded that among patients receiving initial systemic treatment for HR-positive, HER2-negative advanced breast cancer, the addition of KISQALI® to FEMARA® significantly prolonged PFS compared to FEMARA® alone, with a higher rate of myelosuppression noted in the KISQALI® group. Ribociclib as First-Line Therapy for HR-positive, Advanced Breast Cancer. Hortobagyi GN, Stemmer SM, Burris HA, et al. N Engl J Med 375:1738-1748, 2016.
KISQALI® (Ribociclib)
The FDA on March 13, 2017 approved KISQALI®, a cyclin-dependent kinase 4/6 inhibitor, in combination with an Aromatase Inhibitor, as initial endocrine-based therapy for the treatment of postmenopausal women with Hormone Receptor (HR)-positive, Human Epidermal Growth Factor receptor 2 (HER2)-negative advanced or metastatic breast cancer. KISQALI®is a product of Novartis Pharmaceuticals Corp