
The IDEA Collaboration is a prospective, pre-planned pooled analysis of 6 concurrently conducted randomized phase III trials, which included 12,834 patients from 12 countries. They concluded that a risk-based approach has to be taken when making adjuvant chemotherapy recommendations for patients with stage III colon cancer. Three months of adjuvant chemotherapy is adequate for patients with T1-3, N1 disease. This study data was presented at 2017 ASCO Annual Meeting.
Category: Hem/Onc Updates
FDA Approves Subcutaneous RITUXAN® Formulation for CD20-Positive Hematologic Malignancies
SUMMARY: The US FDA on June 22, 2017, granted regular approval to the combination of RITUXAN® (Rituximab) and Hyaluronidase human (RITUXAN HYCELA®) for adult patients with Follicular Lymphoma, Diffuse Large B-Cell Lymphoma, and Chronic Lymphocytic Leukemia. RITUXAN HYCELA® is a combination of RITUXAN® and Hyaluronidase human (ENHANZE® technology), for SubCutaneous (SC) injection in multiple hematological malignancies. ENHANZE® is a drug delivery technology platform which removes limitations on the volume of biologics and drugs that can be delivered SubCutaneously, thereby significantly reducing the time required for drug administration.
RITUXAN® is a first generation type I, chimeric, monoclonal antibody that targets the CD20 antigen expressed on the surface of pre-B and mature B-lymphocytes. Upon binding to CD20, RITUXAN® mediates B-cell lysis. Possible mechanisms of cell lysis include Complement Dependent Cytotoxicity (CDC) and Antibody Dependent Cell mediated Cytotoxicity (ADCC).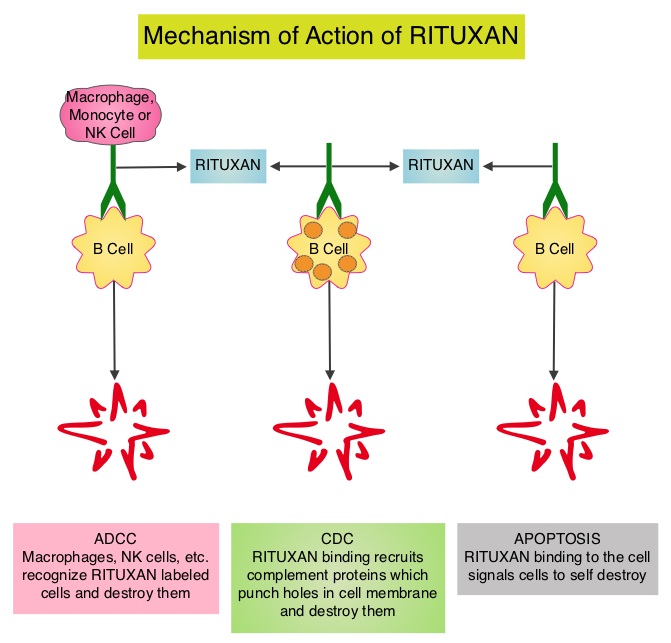 Hyaluronan is a polysaccharide present in the extracellular matrix of the subcutaneous tissue and is depolymerized by the naturally occurring enzyme Hyaluronidase. Hyaluronidase human increases permeability of the subcutaneous tissue locally for a period of 24-48 hrs, by temporarily depolymerizing Hyaluronan.
Hyaluronan is a polysaccharide present in the extracellular matrix of the subcutaneous tissue and is depolymerized by the naturally occurring enzyme Hyaluronidase. Hyaluronidase human increases permeability of the subcutaneous tissue locally for a period of 24-48 hrs, by temporarily depolymerizing Hyaluronan.
The approval of RITUXAN HYCELA® was based on several randomized clinical trials that demonstrated Non-inferior pharmacokinetics of SubCutaneous RITUXAN HYCELA® compared with IV RITUXAN® as well as comparable efficacy and safety results. The following are the specific trials included in the clinical development program:
MabEase phase III trial is an open label study which evaluated SubCutaneous (N=381) versus IV (N=195) RITUXAN® formulation plus CHOP chemotherapy, in treatment naïve patients with CD20-positive Diffuse Large B-Cell Lymphoma. There was no significant difference noted in the Objective Response Rate, Complete Response rates, Progression Free Survival and Overall Survival, between the two treatment groups.
SABRINA is a randomized phase III study that enrolled a total of 410 patients with previously untreated, CD20-positive Follicular Lymphoma and patients were randomized (1:1) to receive either a SC or IV RITUXAN® formulation in combination with CHOP or CVP chemotherapy. There was again no significant difference noted in the Objective Response Rate, Complete Response rates, Progression Free Survival and Overall Survival, between the two treatment groups
The SAWYER study is a phase Ib open label trial which compared the SC and IV formulations of RITUXAN® in combination with Fludarabine and Cyclophosphamide chemotherapy, in 176 treatment naïve patients with Chronic Lymphocytic Leukemia. There was no significant difference noted in the Objective Response Rate, Complete Response rates, Progression Free Survival and Overall Survival, between the two treatment groups.
SparkThera is a phase Ib study which investigated the pharmacokinetics and safety of SubCutaneous (SC) versus IV RITUXAN® formulations as maintenance therapy, in previously untreated or relapsed Follicular Lymphoma. It was noted that the pharmacokinetics of SC RITUXAN® formulation was Non-inferior to IV RITUXAN® formulation, with a comparable safety profile.
PrefMab is a randomized, open label, phase IIIb study which evaluated patient preference for SC or IV RITUXAN® formulation, in previously untreated CD20-positive Follicular lymphoma and Diffuse Large B-Cell Lymphoma. In this study, most patients preferred SC compared with IV formulation of RITUXAN®, mainly due to reduction in the duration and discomfort of administration.
Treatment with RITUXAN HYCELA® should be initiated only after patients had received at least one full dose RITUXAN® by intravenous infusion. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/761064s000lbl.pdf
FDA Approves TAFINLAR® and MEKINIST® Combination for BRAF Positive Non Small Cell Lung Cancer
SUMMARY: The FDA on June 22, 2017, granted regular approvals to TAFINLAR® (Dabrafenib) and MEKINIST® (Trametinib) administered in combination, for patients with metastatic Non Small Cell Lung Cancer (NSCLC), with BRAF V600E mutation, as detected by an FDA-approved test. These are the first FDA approvals specifically for treatment of patients with BRAF V600E mutation-positive metastatic NSCLC.
The FDA also approved the Oncomine® Dx Target Test, a next generation sequencing (NGS) test to detect multiple gene mutations for lung cancer in a single test from a single tissue specimen. This test detects the presence of BRAF, ROS1, and EGFR gene mutations or alterations in tumor tissue of patients with NSCLC. This test can be used to select patients with NSCLC with the BRAF V600E mutation for treatment with the combination of TAFINLAR® and MEKINIST®. This is the first NGS oncology panel test approved by the FDA for multiple companion diagnostic indications.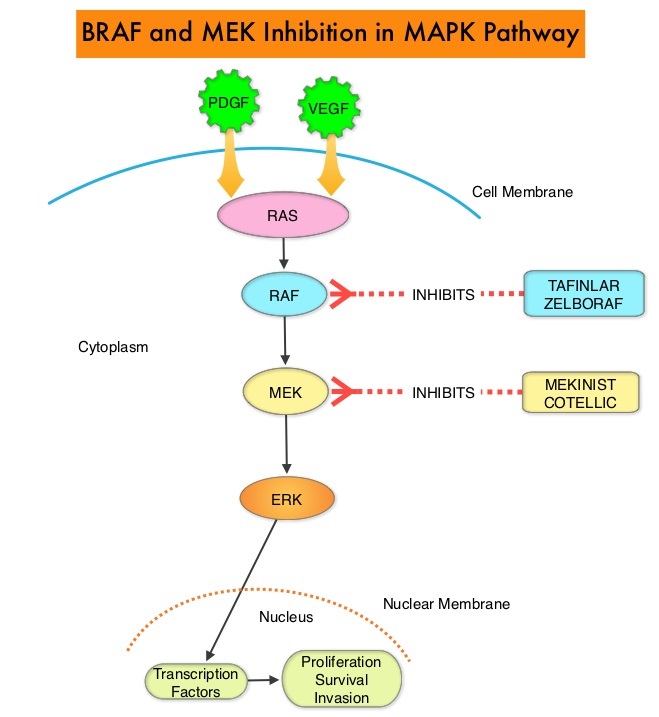
Combining MEKINIST® (Trametinib) with TAFINLAR® (Dabrafenib) to treat patients with NSCLC, was based on the understanding of the biological pathways of this malignancy. The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. This pathway has been implicated in the development of multiple malignancies including NSCLC and Melanoma. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. BRAF mutations have been demonstrated in 6-8% of all malignancies. TAFINLAR® is a selective oral BRAF inhibitor and MEKINIST® is a potent and selective inhibitor of MEK gene, which is downstream from RAF in the MAPK pathway.
The approval of TAFINLAR® and MEKINIST® combination, for patients with metastatic NSCLC was based on an international, multicenter, three-cohort, non-randomized, open-label trial, in patients with locally confirmed BRAF V600E mutation-positive, metastatic NSCLC. In this phase II trial, 93 patients were treated with the combination of TAFINLAR® 150 mg orally twice daily and MEKINIST® 2 mg orally once daily. Of these 93 patients, 36 patients had received no prior systemic therapy for metastatic NSCLC and 57 patients received at least one prior platinum-based chemotherapy regimen and had disease progression. The third cohort in this phase II trial included 78 previously treated patients with BRAF V600E mutation-positive metastatic NSCLC, who received single-agent TAFINLAR®. The primary endpoint was Overall Response Rate (ORR).
It was noted that in the previously treated group, the ORR for the combination treatment based on independent review was 63% with a median Duration of Response of 12.6 months. In the treatment-naive group, the ORR for the combination was 61% and this group had not reached the endpoint for median Duration of Response and therefore was not estimable. However, among those who responded to treatment, 59% of the responders had response durations greater than 6 months. The ORR for patients who received single agent TAFINLAR® was 27% and the median Duration of Response was 9.9 months. The most common Grade 3-4 adverse reactions were pyrexia, fatigue, dyspnea, vomiting, rash, hemorrhage, and diarrhea.
It was concluded that TAFINLAR® plus MEKINIST® combination represents a new targeted therapy for patients with BRAF V600E mutation¬-positive metastatic NSCLC, who tend to respond less favorably to standard chemotherapy. This approval marks the fourth actionable genomic biomarker in metastatic NSCLC along with EGFR, ALK and ROS-1. Dabrafenib plus trametinib in patients with previously treated BRAF(V600E)-mutant metastatic non-small cell lung cancer: an open-label, multicentre phase 2 trial. Planchard D, Besse B, Groen HJ et al. Lancet Oncol. 2016 Jul;17(7):984-93. doi: 10.1016/S1470-2045(16)30146-2. Epub 2016 Jun 6.
Late Breaking Abstract – ASCO 2017 Adjuvant Dual HER2 Regimen of PERJETA® and HERCEPTIN® Improves Outcomes in Early Stage Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 255,180 new cases of invasive breast cancer will be diagnosed in 2017 and over 41,070 women will die of the disease. The HER or erbB family of receptors consist of HER1, HER2, HER3 and HER4. Approximately 15%-20% of invasive breast cancers overexpress HER2/neu oncogene, which is a negative predictor of outcomes without systemic therapy. HERCEPTIN® (Trastuzumab) is a humanized monoclonal antibody targeting HER2. Trastuzumab binds to subdomain IV of the HER2 extracellular domain and blocks the downstream cell signaling pathways (PI3K-AKT pathway) and induces Antibody Dependent Cellular Cytotoxicity (ADCC). Adjuvant chemotherapy given along with HERCEPTIN® reduces the risk of disease recurrence and death, among patients with HER2-positive early breast cancer.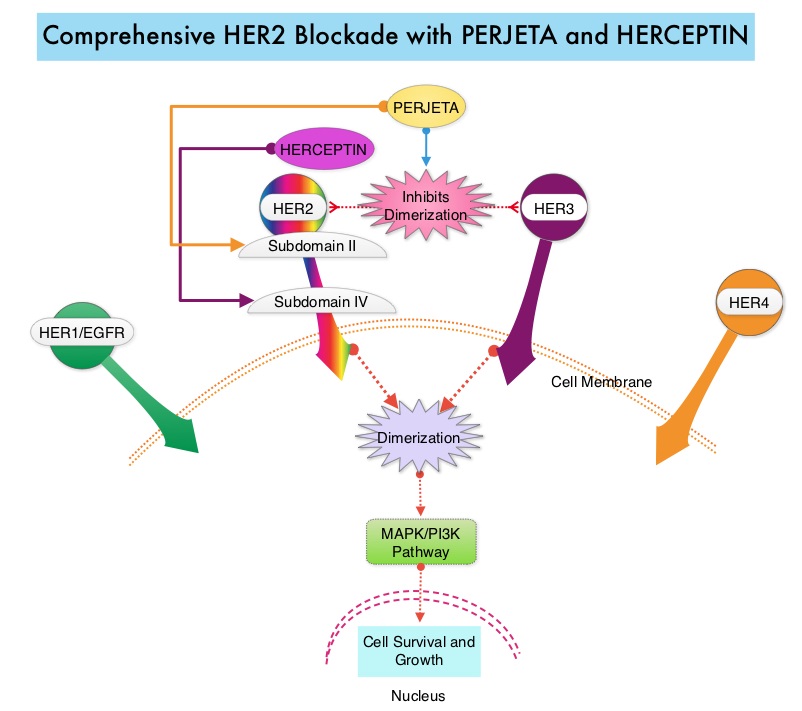
PERJETA® (Pertuzumab) is a recombinant humanized monoclonal antibody that binds to the HER2 at a different epitope of the HER2 extracellular domain (subdomain II) compared to HERCEPTIN® and prevents the dimerization of HER2 with HER3 receptor. PERJETA® induces ADCC similar to HERCEPTIN®. By combining HERCEPTIN® and PERJETA®, a more comprehensive blockade of HER2 signaling can be accomplished, as these two agents bind to different HER2 epitopes and may complement each other and improve efficacy. In the CLEOPATRA study, the addition of PERJETA® to HERCEPTIN® and Docetaxel resulted in significant improvement in Progression Free Survival (PFS) and Overall Survival (OS), in patients with HER-positive metastatic breast cancer. This triple drug combination also resulted in a significantly increased pathological Complete Response rate, when given in a neoadjuvant setting (NeoSphere trial).
Based on these previously published efficacy data, the authors in this study investigated whether the addition of PERJETA® to adjuvant HERCEPTIN® and chemotherapy, improves outcomes, among patients with HER2-positive early breast cancer. APHINITY is a prospective, randomized, multicenter, multinational, double-blind, placebo-controlled phase III trial in which a total of 4805 patients were randomly assigned in a 1:1 ratio, to receive standard adjuvant anthracycline or non-anthracycline chemotherapy regimen along with HERCEPTIN® plus either PERJETA® (2400 patients) or placebo (2405 patients). Anti-HER2 therapy was administered for a total of 1 year. Patients could receive radiotherapy and/or endocrine therapy following completion of adjuvant chemotherapy. Eligible patients had node-positive or high-risk node-negative (tumor diameter greater than 1.0 cm), HER2-positive, non-metastatic, adequately excised breast cancer. Both treatment groups were well balanced and about 37% of the patients had 1-3 positive lymph nodes and 25% of the patients had 4 or more positive lymph nodes. Two thirds of the patients were hormone receptor positive and about 78% of the patients received an anthracycline containing adjuvant chemotherapy regimen. The median follow up was 45.4 months and one year of treatment was completed by approximately 85% of the patients in both treatment groups. The primary end point was Disease Free Survival (DFS) from invasive breast cancer and secondary end points included Overall Survival (OS) and DFS from non-invasive breast cancers.
The addition of PERJETA® to chemotherapy and HERCEPTIN® resulted in a higher rate of DFS for invasive breast cancer with a 3-year invasive DFS of 94.1% in the PERJETA® group and 93.2% in the placebo group (HR=0.81; P=0.045), in favor of PERJETA®. Patients in the high risk subgroups benefited the most. The 3-year invasive DFS for patients with node-positive disease was 92.0% in the PERJETA® group, compared with 90.2% in the placebo group (HR=0.77; P=0.02). In the cohort of patients with hormone receptor negative tumors, the 3-year invasive DFS was 92.8% in the PERJETA® group and 91.2% in the placebo group (HR=0.76; P=0.08). The site of first distant recurrence was visceral or in the CNS rather than the bone. Cardiac toxicities were uncommon in both treatment groups and patients in the PERJETA® group had higher incidence of diarrhea while on concurrent chemotherapy.
It was concluded that for patients with HER2-positive early breast cancer, the addition of PERJETA® to standard postoperative HERCEPTIN® based adjuvant chemotherapy, significantly improved Disease Free Survival for invasive breast cancer. This benefit was more so for those patients with high risk disease. APHINITY trial (BIG 4-11): A randomized comparison of chemotherapy (C) plus trastuzumab (T) plus placebo (Pla) versus chemotherapy plus trastuzumab (T) plus pertuzumab (P) as adjuvant therapy in patients (pts) with HER2-positive early breast cancer (EBC). von Minckwitz G, Procter MJ, De Azambuja E, et al. J Clin Oncol. 2017;35(suppl; abstr LBA500).
Late Breaking Abstract – ASCO 2017 Dacomitinib Superior to IRESSA® in EGFR Mutant Non-Small Cell Lung Cancer
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2017 about 222,500 new cases of lung cancer will be diagnosed and over 155,000 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 25% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large cell carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer. Approximately 10% to 15% of Caucasian patients and 50% of Asian patients with Adenocarcinomas, harbor activating EGFR (Epidermal Growth Factor Receptor) mutations and 90% of these mutations are either Exon 19 deletions or L858R point mutations in Exon 21. EGFR Tyrosine Kinase Inhibitors (TKIs) such as TARCEVA® (Erlotinib), IRESSA® (Gefitinib) and GILOTRIF® (Afatinib), have demonstrated a 60% to 70% response rate as monotherapy when administered as first line treatment, in patients with metastatic NSCLC, who harbor the sensitizing EGFR mutations.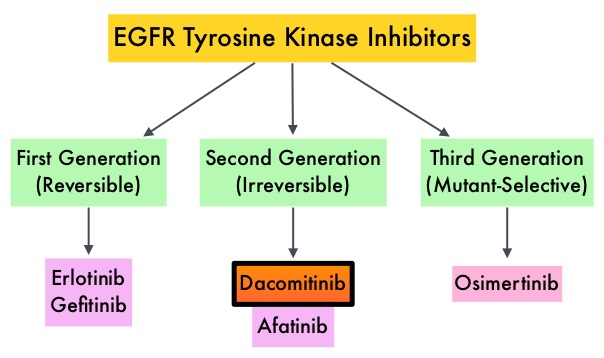
Dacomitinib is a potent, irreversible, second-generation EGFR Tyrosine Kinase Inhibitor and inhibits three members of the ErbB protein family, including EGFR/HER1, HER2 and HER4. Based on the encouraging clinical activity of Dacomitinib in treatment naïve patients with advanced NSCLC, harboring activating EGFR mutations, in a phase II study (The Lancet Oncology 2014;15:1433-1441), the authors conducted a randomized phase III trial, comparing Dacomitinib with IRESSA®, as first line therapy in this patient population . This study (ARCHER 1050) randomized 452 patients in a 1:1 ratio to either receive Dacomitinib 45 mg PO daily (N=227) or IRESSA® 250 mg PO daily (N=225). Eligible patients had newly diagnosed stage IIIB/IV or recurrent NSCLC, harboring an activating EGFR mutation (Exon 19 deletions or L858R point mutations in Exon 21, with or without Exon 20 T790M mutations). Treatments groups were well balanced and patients were stratified by race and EGFR mutation subtype. The Primary endpoint was Progression Free Survival (PFS) and Secondary endpoints included Overall Survival (OS), Objective Response Rate (ORR) and Duration of Response (DoR).
The median PFS for patients who received Dacomitinib was 14.7 months compared with 9.2 months for the group who received IRESSA® (HR=0.59; P<0.0001). This meant a 41% reduction in the risk of cancer progression or death with Dacomitinib compared with IRESSA®. The median Duration of Response was 14.8 months with Dacomitinib versus 8.3 months with IRESSA® (HR= 0.40; P<0.0001). As expected, patients in the Dacomitinib group experienced more side effects such as skin rash and diarrhea and this has been attributed to the stronger suppression of the EGFRs in the normal healthy tissues.
The authors concluded that ARCHER 1050 is the first phase III trial comparing EGFR TKIs head-to-head, and this study demonstrated clinically meaningful superiority of Dacomitinib, when compared to IRESSA®, in treatment naïve NSCLC patients, with activating EGFR mutations. Further, the PFS achieved with Dacomitinib in this study is among the highest observed, when compared with other EGFR Tyrosine Kinase Inhibitors, for this cancer type. Dacomitinib versus gefitinib for the first-line treatment of advanced EGFR mutation positive non-small cell lung cancer (ARCHER 1050): A randomized, open-label phase III trial. Mok T, Cheng Y, Zhou X, et al. J Clin Oncol 35, 2017 (suppl; abstr LBA9007)
Late Breaking Abstract – ASCO 2017 ALECENSA® Superior to XALKORI® in Untreated ALK-Positive Non Small Cell Lung Cancer
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2017 about 222,500 new cases of lung cancer will be diagnosed and over 155,000 patients will die of the disease. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 25% are Squamous cell carcinomas, 40% are Adenocarcinomas and 10% are Large cell carcinomas. The discovery of rearrangements of the Anaplastic Lymphoma Kinase (ALK) gene in some patients with advanced NSCLC and adenocarcinoma histology, led to the development of agents such as XALKORI® (Crizotinib), ZYKADIA® (Ceritinib), ALECENSA® (Alectinib) and now ALUNBRIG® (Brigatinib), with promising results. It has become clear that appropriate, molecularly targeted therapy for tumors with a molecular abnormality, results in the best outcomes. According to the US Lung Cancer Mutation Consortium (LCMC), two thirds of patients with advanced adenocarcinoma of the lung, have a molecular driver abnormality. The most common oncogenic drivers in patients with advanced adenocarcinoma of the lung are, KRAS in 25%, EGFR in 21% and ALK in 8% as well as other mutations in BRAF, HER2, AKT1 and fusions involving RET and ROS oncogenes. These mutations are mutually exclusive and the presence of two simultaneous mutations, are rare.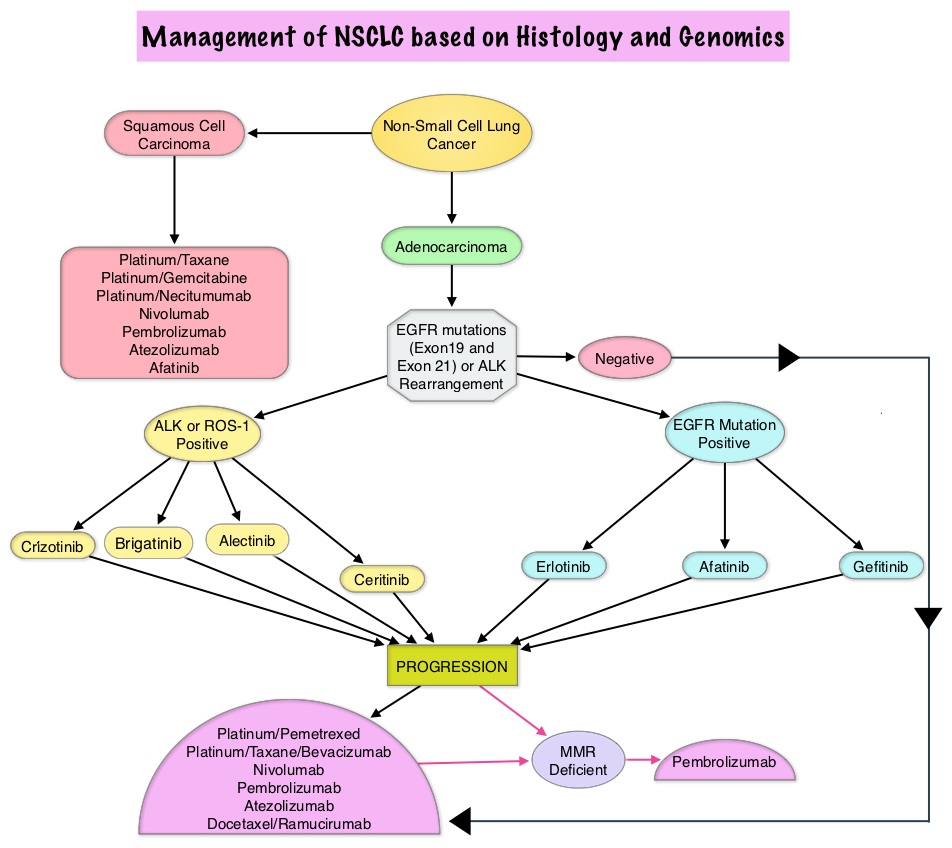
Patients with advanced NSCLC harboring ALK gene rearrangements often receive XALKORI® as first line therapy and can expect a median Progression Free Survival of approximately 11 months. These patients however are at a high lifetime risk of CNS metastases. ALECENSA® (Alectinib) is a potent ALK Tyrosine Kinase Inhibitor, and is effective against several ALK mutations that confer resistance to XALKORI® Further, unlike XALKORI®, ALECENSA® can cross the blood-brain barrier and is not a substrate of P-glycoprotein, a key efflux transporter located at the blood-brain barrier.
The ALEX trial is an international, randomized, open-label, phase III study which compared ALECENSA® with XALKORI®, in patients with previously untreated, advanced ALK-positive NSCLC, including those with asymptomatic CNS disease. In this trial, 303 previously untreated patients were randomly assigned in a 1:1 ratio to receive ALECENSA® at 600 mg twice daily (N=152) or XALKORI® at 250 mg PO twice daily (N=151). Treatment was continued until disease progression or unacceptable toxicities. Patients with isolated asymptomatic CNS progression could receive a local therapy at the investigator’s discretion, followed by continued trial treatment until systemic disease progression. Patients were stratified and the primary end point was Investigator-assessed Progression Free Survival. Secondary end points were Independent Review Committee (IRC)–assessed Progression Free Survival, time to CNS progression, Objective Response Rate, and Overall Survival.
At the time of primary analysis, ALECENSA® was significantly superior to XALKORI®, reducing the risk of progression/death by 53% (HR= 0.47; P<0.0001). The median PFS for ALECENSA® was Not Reached versus 11.1 months for XALKORI®. The median Progression Free Survival assessed by the IRC was 25.7 months for ALECENSA® vs 10.4 months for XALKORI® (HR=0.50, P< 0.001). The magnitude of the benefit with ALECENSA® was generally consistent across all the subgroups although this benefit was lower in the subgroups of active smokers and patients with poor Performance Status. Objective Response Rate was 82.9% in the ALECENSA® group versus 75.5% in the XALKORI® group (P=0.09). The rate of CNS progression was 12% in the ALECENSA® group compared with 45% in the XALKORI® group (HR=0.16; P<0.001). Among patients with measurable or non-measurable CNS lesions at baseline, a CNS response occurred in 59% of the patients in the ALECENSA® group versus 26% in the XALKORI® group. Further, 45% of the patients in the ALECENSA® group had a complete CNS response, as compared with 9% in the XALKORI® group. Grade 3-5 adverse events were less frequent with ALECENSA® (41%) versus 50% with XALKORI®.
It was concluded that ALECENSA® showed superior efficacy and lower toxicity compared with XALKORI®, and should be a new standard of care for treatment-naïve patients with ALK-positive NSCLC. Alectinib versus crizotinib in treatment-naive advanced ALK-positive non–small cell lung cancer (NSCLC): primary results of the global phase III ALEX study. Shaw AT, Peters S, Mok T, et al. J Clin Oncol. 2017;35 (suppl; abstr LBA9008).
Adjuvant Therapy with XELODA® Improves Overall Survival in Biliary Tract Cancer
SUMMARY: Bile Duct cancer (Cholangiocarcinoma), comprise about 30% of all primary liver tumors and includes both intrahepatic and extrahepatic bile duct cancers. About 8,000 people in the US are diagnosed with bile duct cancer each year. The average age of an individual in the US diagnosed with bile duct cancer is 71 years and approximately 20% of the cases are suitable for surgical resection. The 5-year survival is less than 10%. There is no standard adjuvant therapy for patients with resectable bile duct cancer, although adjuvant intervention in a previously reported meta-analysis showed improved Overall Survival (Horgan AM, Amir E, Walter T, et al. JCO 2012;30:1934-1940).
The BILCAP trial is a phase III study conducted to determine whether XELODA® (Capecitabine) improved Overall Survival (OS) compared to Observation, following radical surgery. In this trial, 447 patients were randomized to receive XELODA® (N=223) or Observation (N=224). Eligible patients had completely resected, cholangiocarcinoma or gallbladder cancer (including liver and pancreatic resection, as appropriate), with a R0 resection (microscopically negative margin resection) for 62% and R1 resection (removal of all macroscopic disease, but microscopic margins are positive for tumor) for 38% and with negative lymph nodes in 46% of the patients. The primary disease sites were extrahepatic cholangiocarcinoma (35%), hilar (28%), intrahepatic (19%), and muscle-invasive gallbladder cancers (18%). Patients were randomized in a 1:1 ratio to receive XELODA® 1250 mg/m2, D1-14 every 21 days, for 8 cycles or Observation. The median age was 63 years and the follow up was at least 36 months in more than 80% of the surviving patients. The primary end point was Overall Survival in the Intent to Treat population and the primary analysis was performed with at least 24 months of follow up.
The median Overall Survival with XELODA® was 51 months compared with 36 months for Observation, and this was not statistically significant (P=0.097). In the sensitivity analyses however, with adjustment for nodal status, gender and grade of the disease, there was a 29% reduction in the risk of death with adjuvant XELODA®, when compared with Observation (HR=0.71; P < 0.01). In the per-protocol analysis which included 430 patients, the median Overall Survival was 53 months with adjuvant XELODA® versus 36 months with Observation, resulting in a 25% reduction in the risk of death with XELODA®, and these results were statistically significant (HR=0.75; P=0.028). The most common adverse events related to XELODA® as anticipated were, palmar plantar erythema, fatigue and diarrhea.
The authors concluded that single agent XELODA® improves Overall Survival in Biliary Tract Cancer, when used as adjuvant therapy, without a negative impact on Quality of Life. They added that this is the first phase III study to show a survival benefit in the adjuvant setting, and should become standard of care. Adjuvant capecitabine for biliary tract cancer: The BILCAP randomized study. Primrose JN, Fox R, Palmer DH, et al. J Clin Oncol 35, 2017 (suppl; abstr 4006)
Late Breaking Abstract – ASCO 2017 Three Months of Adjuvant Therapy Adequate for Stage III Colon Cancer Patients with T1-3, N1 Disease
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. Adjuvant chemotherapy for patients with resected, locally advanced, node-positive (stage III) colon cancer, has been the standard of care since 1990s. Adjuvant treatment with an ELOXATIN® (Oxaliplatin) based chemotherapy regimen has been considered standard intervention since 2004, for patients with stage III colon cancer following surgical resection and has been proven to decrease the chance of recurrent disease. Chemotherapy regimens have included (FOLFOX – Leucovorin, 5-FluoroUracil, ELOXATIN®) or CAPOX/XELOX (XELODA®/Capecitabine and ELOXATIN®/Oxaliplatin), given over a period of 6 months. ELOXATIN® can however be associated with neuropathy which can be long lasting or permanent, depending on the duration of therapy. Additional toxicities with longer duration of chemotherapy include diarrhea, fatigue as well as more office visits.
The IDEA Collaboration is a prospective, pre-planned pooled analysis of 6 concurrently conducted randomized phase III trials which included 12,834 patients from 12 countries. The goal of this study was to determine if 3 months of adjuvant chemotherapy would be as effective as 6 months of therapy and would be Non Inferior. Of the enrolled patients with Stage III disease, 13% had T1-2 disease, 66% had T3 disease, and 21% had T4 tumors. Twenty eight percent (28%) of the patients had N2 disease and 40% of the patients received XELOX chemotherapy. Approximately 60% had low-risk disease (T1-3, N1) and 40% had high-risk (T4 or N2). The primary endpoint was Disease Free Survival (DFS). The median follow up was 39 months.
It was noted that a shorter 3 month course of adjuvant chemotherapy was associated with a less than 1% lower risk of recurrence at 3 years compared to the standard 6 month course of therapy (74.6% versus 75.5%). In the subset of patients considered to be at low risk of cancer recurrence (1-3 positive lymph nodes and tumor not completely penetrating through the bowel wall), there was almost no difference in the DFS between a 3-month versus 6-month course of therapy (83.1% vs 83.3%). Even though Non Inferiority was not established for the overall cohort of patients, patients with stage T1-3 N1 disease showed Non Inferiority for 3 months versus 6 month course of adjuvant therapy. Further, 3 months of XELOX adjuvant therapy was Non Inferior to 6 months of ELOXATIN® based adjuvant therapy. Grade 2 or more neurotoxicity was significantly lower for patients who received 3 months of adjuvant therapy versus 6 months (P <0.0001), regardless of the treatment regimen (17% vs 48% for FOLFOX and 15% vs 45% for XELOX, respectively).
It was concluded by the IDEA collaboration that, a risk-based approach has to be taken when making adjuvant chemotherapy recommendations for patients with stage III colon cancer. Three months of adjuvant chemotherapy is adequate for patients with T1-3, N1 disease. For patients with T4 and/or N2 disease or other high risk factors, the duration of adjuvant therapy has to be determined based on patient preference, assessment of recurrent risk and tolerability. Prospective pooled analysis of six phase III trials investigating duration of adjuvant (adjuv) oxaliplatin-based therapy (3 vs 6 months) for patients (pts) with stage III colon cancer (CC): The IDEA (International Duration Evaluation of Adjuvant chemotherapy) collaboration. Shi Q, Sobrero AF, Shields AF, et al. J Clin Oncol 35, 2017 (suppl; abstr LBA1)
Late Breaking Abstract – ASCO 2017 LYNPARZA® Improves Progression Free Survival in BRCA Positive Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 255,180 new cases of invasive breast cancer will be diagnosed in 2017 and over 41,070 women will die of the disease. DNA can be damaged due to errors during its replication or as a result of environmental exposure to ultraviolet radiation from the sun or other toxins. The tumor suppressor genes such as BRCA1 (Breast Cancer 1) and BRCA2 help repair damaged DNA and thus play an important role in maintaining cellular genetic integrity, failing which these genetic aberrations can result in malignancies. The BRCA1 gene is located on the long (q) arm of chromosome 17 whereas BRCA2 is located on the long arm of chromosome 13. Mutations in BRCA1 and BRCA2 account for about 20 to 25 percent of hereditary breast cancers and about 5 to 10 percent of all breast cancers. These mutations can be inherited from either of the parents and a child has a 50 percent chance of inheriting this mutation and the deleterious effects of the mutations are seen even when an individual’s second copy of the gene is normal. 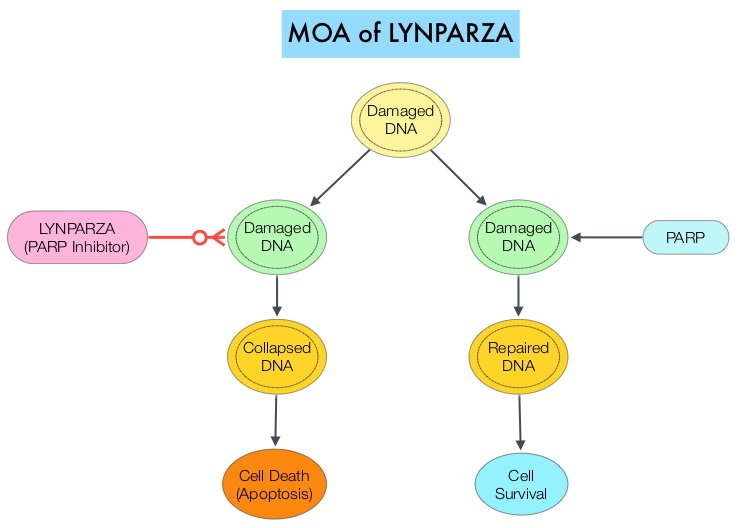
The PARP (Poly ADP Ribose Polymerase) family of enzymes which include PARP1 and PARP2, repair damaged DNA. LYNPARZA® (Olaparib) is a PARP enzyme inhibitor that causes cell death in tumors that already have a DNA repair defect, such as those with BRCA1 and BRCA2 mutations. The FDA approved LYNPARZA® (Olaparib) in 2014 as monotherapy for the treatment of patients with deleterious or suspected deleterious germline BRCA mutated advanced ovarian cancer.
OlympiAD is a randomized, open-label, phase III study that evaluated the efficacy and safety of LYNPARZA® (Olaparib) compared with physician’s choice of standard single agent chemotherapy (TPC), in patients with HER2-negative metastatic breast cancer, with inherited, germline BRCA mutations. In this study, 302 patients were randomized in a 2:1 ratio to receive LYNPARZA® tablets 300 mg PO BID (N=205) or physician’s choice of standard chemotherapy (N=97). The later included 21-day cycles of either XELODA® (Capecitabine) 2500 mg/m2 orally on days 1-14, NAVELBINE® (Vinorelbine) 30 mg/m2 IV days 1 and 8 or HALAVEN® (Eribulin)1.4 mg/m2 IV days 1 and 8. Treatment was continued until disease progression or unacceptable toxicity. The median age was 44 years, 50% of the patients had triple negative disease, 71% of the patients had prior chemotherapy for metastatic breast cancer, 28% had prior platinum based chemotherapy regimen and those with hormone receptor positive breast cancer had received hormonal therapy. The primary endpoint was Progression Free Survival (PFS). Secondary endpoints included Overall Survival, time to second progression or death, Objective Response Rate and effect on health-related Quality of Life.
At a median follow up of about 14 months, the median PFS was 7 months in the LYNPARZA® group versus 4.2 months with standard chemotherapy (HR=0.58; P=0.0009), suggesting a 42% reduced risk of cancer progression in the LYNPARZA® group compared to those who received chemotherapy. Following disease progression, the time to second progression (which meant duration of time before the cancer worsened again), was also longer in the LYNPARZA® group (HR 0.57), suggesting that recurrent disease was not more aggressive following progression on LYNPARZA®. The Objective Response Rate was 60% and 29% in LYNPARZA® and chemotherapy group respectively. Severe side effects were more common in chemotherapy treated patients (50%) compared with LYNPARZA® group (37%). The most common side effects in the LYNPARZA® group included nausea, fatigue and cytopenias, where as rash on hands and feet were most common in the chemotherapy group.
The authors concluded that LYNPARZA® monotherapy significantly improved Progression Free Survival in HER2-negative metastatic breast cancer patients, with inherited germline BRCA mutations, compared to standard chemotherapy. This “proof of the principle” study demonstrated that breast cancers with defects in a specific DNA damage repair pathway are sensitive to targeted therapy and this is the first of several phase III studies with PARP inhibitors that are underway. OlympiAD: Phase III trial of olaparib monotherapy versus chemotherapy for patients (pts) with HER2-negative metastatic breast cancer (mBC) and a germline BRCA mutation (gBRCAm). Robson ME, Im S-A, Senkus E, et al. J Clin Oncol 35, 2017 (suppl; abstr LBA4).
Late Breaking Abstract – ASCO 2017 Targeted Therapy Based on Genomic Profiling Improves Overall Survival
SUMMARY: Tumor genomic profiling enables the identification of specific genomic alterations and thereby can provide personalized treatment options with targeted therapies that are specific for those molecular targets. A genomic test can be performed on a tumor specimen or on cell-free DNA in plasma (“liquid biopsy”) or an ImmunoHistoChemistry (IHC) test can be performed on tumor tissue for protein expression that demonstrates a genomic variant known to be a drug target, or to predict sensitivity to a chemotherapeutic drug. Next-generation sequencing (NGS) platforms or second-generation sequencing unlike the first-generation sequencing, known as Sanger sequencing, perform massively parallel sequencing, which allows sequencing of millions of fragments of DNA from a single sample. With this high-throughput sequencing, the entire genome can be sequenced in less than 24 hours. Recently reported genomic profiling studies performed in patients with advanced cancer suggest that actionable mutations are found in 20-40% of patients’ tumors.
ProfiLER is an ongoing, molecular profiling clinical trial, developed to guide treatment by exploring genomic alterations in cancer cells of patients with advanced malignancy. DNA extracted from either archival or fresh tumor tissue was analyzed by next-generation sequencing of 60 cancer-related genes and whole-genome comparative genomic hybridization, a methodology for rapidly comparing DNA samples. A multidisciplinary board of experts in genomic profiling analyzed the genomic test results data and recommended molecular targeted therapies, when actionable mutations were found. These therapies were either commercially available drugs or those being tested in early clinical trials.
This study enrolled 2,676 patients to date and 1,944 tumors were analyzed. They included colorectal, gynecologic, breast, brain, and head and neck cancers, as well as sarcomas. Actionable mutations were found in 1,004 tumor samples (52%), 609 patients had only 1 actionable mutation, and 394 patients had 2-6 actionable mutations. The most common actionable mutation involved the PI3K/mTOR pathway. The molecular tumor board recommended molecularly targeted treatments to 676 patients (35% of 1,944 patients tested). Of these 676 patients, 143 received the recommended treatment, mostly through enrollment in a clinical trial. The rest of the 533 patients were unable to receive the recommended treatment because of poor health, rapid tumor progression, not meeting eligibility criteria for a clinical trial, or difficulty obtaining off-label commercially available drugs.
The Overall Survival rates for the 143 patients who received targeted therapies based on genomic testing was then compared with the 533 patients who did not. The Overall Survival rate at 3 years for those patients who received the recommended molecular targeted therapy was 53.7% compared with 46.1% for those patients who did not. The 5-year Overall Survival rate was also higher for patients who received molecular targeted therapy compared to those who did not (34.8% versus 28.1%).
This study validated that comprehensive genomic profiling can be performed in routine clinical practice, to select patients for targeted cancer therapies. The TAPUR (Targeted Agent and Profiling Utilization Registry) study conducted by ASCO is underway and is aimed at collecting “real-world” data on clinical outcomes, to help learn additional uses of molecularly-targeted cancer drugs, outside of indications approved by the FDA. Routine molecular screening of advanced refractory cancer patients: An analysis of the first 2490 patients of the ProfilER Study. Tredan O, Corset V, Wang Q, et al. J Clin Oncol 35, 2017 (suppl; abstr LBA100)