SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease largely due to metastatic recurrence. Carcinoma in situ of the breast also known as Ductal Carcinoma In Situ (DCIS) is defined as a malignant proliferation of ductal epithelial cells that are confined to the milk ducts without invasion of the basement membrane, and is a precursor lesion to invasive carcinoma. DCIS accounts for approximately 25% of all newly diagnosed breast cancers. Patients with small, screening-detected lesions, are often treated with breast-conserving surgery (to prevent the development of invasive breast cancer), followed by adjuvant radiation and hormonal therapy, although neither of the latter two interventions have been shown to improve survival outcomes. As such, a significant number of patients are over treated. DCIS in itself is not life-threatening but can potentially progress to invasive breast cancer. The two important goals of DCIS treatment therefore are, to prevent invasive ipsilateral cancer recurrence and to prevent death from breast cancer. There remains a large unmet need, to distinguish relatively benign DCIS from DCIS that will develop into invasive breast cancer.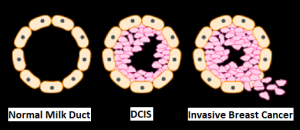
In a previously published meta-analysis (Cancer Epidemiol Biomarkers Prev. 2019;28:835-845), researchers identified six prognostic factors that were statistically significant and were associated with a 36% to 84% increase in the relative risk of recurrence of invasive disease after a DCIS diagnosis. These six factors included-
1) African American race (43% higher risk)
2) Premenopausal status (59% higher risk)bre
3) Detection by palpation (84% higher risk)
4) Positive margins (63% higher risk)
5) High histologic grade (36% higher risk)
6) High p16 expression (51% higher risk).
This present large cohort study was conducted to determine the risk of death from breast cancer, following diagnosis and treatment of DCIS, compared with the mortality risk among cancer-free women, in the general population. This study included a total of 144,524 women diagnosed with first primary DCIS between 1995 and 2014, from the Surveillance, Epidemiology and End Results (SEER) registries database. Patients with DCIS with microinvasion, Lobular Carcinoma In Situ (LCIS), nonepithelial histological presentations, Paget disease of the nipple, diffuse DCIS, unknown laterality, no surgical intervention on the primary tumor, DCIS diagnosis in women younger than 25 years or aged 80 years or older, were all excluded. Patients with DCIS underwent surgical treatment, and approximately half of these patients also received radiotherapy. These patients were followed from the date of DCIS diagnosis until death from breast cancer, or date of last follow up. These patients were compared with women in the general population without a diagnosis of breast cancer (control group). The mean age at diagnosis was 57.4 years. The Primary outcome was death from breast cancer. Standardized Mortality Ratios (SMR) were estimated by comparing deaths from breast cancer among women diagnosed with DCIS, with expected deaths from breast cancer among women in the general population who did not have cancer.
At a mean follow up period of 9.2 years, the incidence of ipsilateral invasive recurrence events was 3.1%, resulting in a 20-year actuarial risk of 13.9%. There was a 3.8% incidence of contralateral invasive breast cancer events during this follow up period, resulting in a 20-year actuarial risk of 11.3%. The 20-year actuarial risk of breast cancer death among women with DCIS was 3.3%.
The Standardized Mortality Ratio (SMR) for death from breast cancer given a diagnosis of DCIS was 3.36, but varied based on age and race. The SMR for women younger than 40 years was much higher at 11.95, whereas the SMR for women aged 40 to 49 years was 4.15. The SMR for White women was 3.03, for Black women was 7.56, and for East Asian women was 1.89. The SMR for Black women diagnosed with DCIS before age 50 years was 12.10, and the SMR for White women diagnosed with DCIS before age 50 years was 4.21, suggesting that Black women did worse than White woman.
All women with DCIS underwent surgical treatment, and 47.1% also received radiotherapy. Among those patients who were not treated with radiotherapy, the SMR was 4.12, for those treated with unilateral mastectomy and 4.14 for those treated with bilateral mastectomies. Among women who underwent lumpectomy, the SMR was 2.81 for women treated with radiotherapy and 3.42 for those who underwent surgical treatment alone. There were 1540 women who died of breast cancer in the cohort, of whom 45.7% experienced an ipsilateral invasive recurrence or contralateral invasive breast cancer in the interval between DCIS and death from breast cancer. Among the patients who died, 27.8% were known to have undergone a mastectomy.
The annual mortality rate from breast cancer over the entire period of follow up was, 0.12% per year. The mortality rate increased for the first 10 years of the follow-up period and remained constant through years 15 thru 20. The cumulative 20-year risk of breast cancer-specific mortality following DCIS was 3.3% overall, but for Black women diagnosed before age 50 years, the 20-year risk of breast cancer-specific mortality was 8.1%. It has been postulated that the highest risk for recurrence among women who underwent mastectomy may be related to them having more extensive disease with close margins or may have genetic mutations that increase the likelihood of recurrence. Further, patients with DCIS undergoing bilateral mastectomies generally are not treated with endocrine therapy.
It was concluded from this cohort study that women with DCIS had a 3-fold increased risk of death from breast cancer after surgical treatment. The Standardized Mortality Ratio was lower among women who received lumpectomy plus radiation compared with women who received lumpectomy alone. The rate of breast cancer death was nearly 12-fold higher among women diagnosed with DCIS before age 40 years and 7-fold higher in Black women diagnosed with DCIS, compared with the general population.
Association of a Diagnosis of Ductal Carcinoma In Situ With Death From Breast Cancer. Giannakeas V, Sopik V and Narod SA. JAMA Netw Open. 2020;3(9):e2017124. doi:10.1001/jamanetworkopen.2020.17124

 and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2020, about 228, 820 new cases of lung cancer will be diagnosed and 135,720 patients will die of the disease.
and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2020, about 228, 820 new cases of lung cancer will be diagnosed and 135,720 patients will die of the disease.