
The FDA granted accelerated approval to KEYTRUDA® (Pembrolizumab), a humanized anti PD-1 antibody, for the treatment of patients with advanced Metastatic Melanoma, who have disease progression following YERVOY® (Ipilimumab) and if BRAF V600 mutation positive, a BRAF inhibitor. KEYTRUDA® produced significant and durable responses in patients with advanced Melanoma, regardless of prior therapy with YERVOY® and this benefit was accomplished with minimal toxicities. This new entry will revolutionize the treatment of advanced Melanoma.
Tag: Malignant Melanoma of the Skin
Efficacy and safety of the anti-PD-1 monoclonal antibody MK-3475 in 411 patients (pts) with melanoma (MEL)
SUMMARY: It is estimated that in the US, approximately 76,000 new cases of melanoma will be diagnosed and close to 8000 individuals will die of the disease in 2014. The incidence of melanoma has been on the rise for the past three decades. Unlike other malignancies, the role of chemotherapy for the treatment of melanoma has been limited. Treatment of advanced melanoma with immunotherapy using a cytokine, Interleukin-2 (IL-2) produced by T cells during an immune response, was first explored in the mid 1970’s. Durable responses were noted in a very small percentage of patients but this was associated with significant toxicities. This however opened the doors for the development of various immunotherapies, with a better understanding of the Immune checkpoints. Immune checkpoints are cell surface inhibitory proteins/receptors that harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response, by switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or Gate Keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1 (Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. The Food and Drug Administration in May 2014, granted Pembrolizumab a Priority Review designation under its Accelerated Approval Program. Pembrolizumab was previously granted a Breakthrough Therapy designation for advanced melanoma. The authors in this largest phase I clinical trial ever done in patients with malignant melanoma, evaluated the efficacy and safety of Pembrolizumab (formerly known as MK-3475, Lambrolizumab), a humanized monoclonal IgG4 anti PD-1 antibody, in a pooled analysis of 411 patients with advanced melanoma. Of these patients, 221 patients had prior therapy with Ipilimumab (YERVOY® ) and 190 patients were YERVOY® naïve. In this study, three different dosing schedules for Pembrolizumab were utilized – 2 mg/kg every three weeks (N=162), 10 mg/kg every three weeks (N=192) and 10 mg/kg every two weeks (N=57). At the time of this analysis, all patients had at least 6 months of follow up and 75% of the patients had been followed up for at least 9 months. The Overall Response Rate was 40% in the YERVOY® naïve group and 28% in the YERVOY® treated group. Responses were durable and ongoing (88% ongoing) at the time of this analysis. The duration of responses ranged from 6 to 76 weeks, and the median response duration has not yet been reached. The median Progression Free Survival was 24 weeks in YERVOY® naïve group and 23 weeks in the YERVOY® treated group. The median Overall Survival has not been reached at the time of this analysis and the estimated 1 year Overall Survival rate for all patients was 71%. The activity with Pembrolizumab was demonstrated across all dose levels and patient subgroups, irrespective of prior YERVOY® therapy, performance status, LDH levels, BRAF mutation status, tumor stage, and number, as well as type of prior therapies. The most common adverse events of any grade were fatigue, pruritus and rash. Only 4% of the patients discontinued treatment due to a drug related toxicities and overall, 12% of patients experienced grade 3/4 adverse events. The authors concluded that the PD-1 targeting antibody, Pembrolizumab, produced durable responses in patients with advanced melanoma, regardless of prior therapy with YERVOY® and this benefit was accomplished with minimal toxicities. This efficacy data is comparable to another PD-1 targeted monoclonal antibody, Nivolumab. Because of the lack of cross resistance between anti PD-1 antibodies and YERVOY®, combining PD-1 targeted monoclonal antibody with a CTLA-4 targeted antibody such as YERVOY®, could potentially be synergistic, with better outcomes. Ribas A, Hodi FS, Kefford R, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA 9000)</s
The Food and Drug Administration in May 2014, granted Pembrolizumab a Priority Review designation under its Accelerated Approval Program. Pembrolizumab was previously granted a Breakthrough Therapy designation for advanced melanoma. The authors in this largest phase I clinical trial ever done in patients with malignant melanoma, evaluated the efficacy and safety of Pembrolizumab (formerly known as MK-3475, Lambrolizumab), a humanized monoclonal IgG4 anti PD-1 antibody, in a pooled analysis of 411 patients with advanced melanoma. Of these patients, 221 patients had prior therapy with Ipilimumab (YERVOY® ) and 190 patients were YERVOY® naïve. In this study, three different dosing schedules for Pembrolizumab were utilized – 2 mg/kg every three weeks (N=162), 10 mg/kg every three weeks (N=192) and 10 mg/kg every two weeks (N=57). At the time of this analysis, all patients had at least 6 months of follow up and 75% of the patients had been followed up for at least 9 months. The Overall Response Rate was 40% in the YERVOY® naïve group and 28% in the YERVOY® treated group. Responses were durable and ongoing (88% ongoing) at the time of this analysis. The duration of responses ranged from 6 to 76 weeks, and the median response duration has not yet been reached. The median Progression Free Survival was 24 weeks in YERVOY® naïve group and 23 weeks in the YERVOY® treated group. The median Overall Survival has not been reached at the time of this analysis and the estimated 1 year Overall Survival rate for all patients was 71%. The activity with Pembrolizumab was demonstrated across all dose levels and patient subgroups, irrespective of prior YERVOY® therapy, performance status, LDH levels, BRAF mutation status, tumor stage, and number, as well as type of prior therapies. The most common adverse events of any grade were fatigue, pruritus and rash. Only 4% of the patients discontinued treatment due to a drug related toxicities and overall, 12% of patients experienced grade 3/4 adverse events. The authors concluded that the PD-1 targeting antibody, Pembrolizumab, produced durable responses in patients with advanced melanoma, regardless of prior therapy with YERVOY® and this benefit was accomplished with minimal toxicities. This efficacy data is comparable to another PD-1 targeted monoclonal antibody, Nivolumab. Because of the lack of cross resistance between anti PD-1 antibodies and YERVOY®, combining PD-1 targeted monoclonal antibody with a CTLA-4 targeted antibody such as YERVOY®, could potentially be synergistic, with better outcomes. Ribas A, Hodi FS, Kefford R, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA 9000)</s
Survival, Durable Tumor Remission, and Long-Term Safety in Patients With Advanced Melanoma Receiving Nivolumab
SUMMARY: It is estimated that in the US, approximately 76,000 new cases of melanoma will be diagnosed and close to 8000 individuals will die of the disease, in 2014. The incidence of melanoma has been on the rise for the past three decades. Unlike other malignancies, the role of chemotherapy for the treatment of melanoma has been limited. Treatment of advanced melanoma with immunotherapy using a cytokine, Interleukin-2 (IL-2), produced by T cells during an immune response, was first explored in the mid 1970’s. Durable responses were noted in a very small percentage of patients but this was associated with significant toxicities. This however opened the doors for the development of various immunotherapies with a better understanding of the Immune checkpoints. Immune checkpoints are cell surface inhibitory proteins/receptors that harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation . The T cells of the immune system play a very important role in modulating the immune system.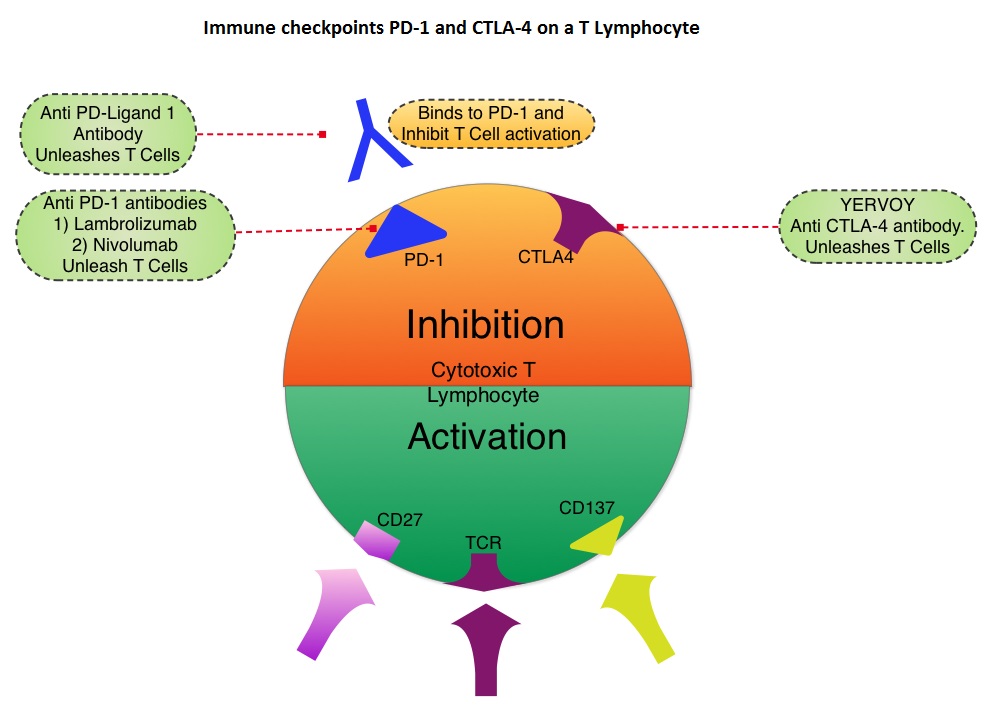 Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. In a previous publication, the authors reported the efficacy results of Nivolumab, a PD-1 targeted, fully human, immunoglobulin G4 monoclonal antibody, which demonstrated an objective response in 20% – 25% of patients with advanced Non Small Cell Lung Cancer, Melanoma and Renal Cell Carcinoma, with favorable toxicities. In this article, the authors reported the outcomes in 107 patients with advanced metastatic melanoma, from the pooled cohort of patients, enrolled between 2008 and 2012. Two thirds of these patients had at least 2 prior treatments, for their advanced disease. These patients received Nivolumab IV, once every 2 weeks, given in an outpatient setting, for up to 96 weeks. Patients were evaluated for Overall Survival, long term safety with treatment and response duration after the treatment was discontinued. The median Overall Survival in those treated with Nivolumab was 16.8 months and 1 and 2-year survival rates were 62% and 43%, respectively. This survival benefit is comparable to that seen following treatment with other agents that are presently available for this patient population, such as YERVOY® (Ipilimumab), ZELBORAF® (Vemurafenib) and combination of BRAF and MEK inhibitors. BRAF mutational status did not impact efficacy of Nivolumab. About 30% of the patients had objective responses and the median response duration was 2 years. The authors hypothesize that the ongoing tumor response following Nivolumab discontinuation, and unlike following chemotherapy, may be due to PD-1 blockade, resulting in the establishment of immune memory response, as is seen after antigen exposure against specific infectious organisms. The most common adverse events of any grade were fatigue, rash and diarrhea. These toxicities were not cumulative. The authors concluded that Nivolumab improved Overall Survival in patients with advanced melanoma and the clinical benefit was durable and persisted even after the drug was discontinued. Studies are underway combining Nivolumab with a different checkpoint inhibitor, YERVOY®. The synergy between these two agents may result in even better outcomes. Topalian SL, Sznol M, McDermott DF, et al. J Clin Oncol 2014;32:1020-1030
Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. In a previous publication, the authors reported the efficacy results of Nivolumab, a PD-1 targeted, fully human, immunoglobulin G4 monoclonal antibody, which demonstrated an objective response in 20% – 25% of patients with advanced Non Small Cell Lung Cancer, Melanoma and Renal Cell Carcinoma, with favorable toxicities. In this article, the authors reported the outcomes in 107 patients with advanced metastatic melanoma, from the pooled cohort of patients, enrolled between 2008 and 2012. Two thirds of these patients had at least 2 prior treatments, for their advanced disease. These patients received Nivolumab IV, once every 2 weeks, given in an outpatient setting, for up to 96 weeks. Patients were evaluated for Overall Survival, long term safety with treatment and response duration after the treatment was discontinued. The median Overall Survival in those treated with Nivolumab was 16.8 months and 1 and 2-year survival rates were 62% and 43%, respectively. This survival benefit is comparable to that seen following treatment with other agents that are presently available for this patient population, such as YERVOY® (Ipilimumab), ZELBORAF® (Vemurafenib) and combination of BRAF and MEK inhibitors. BRAF mutational status did not impact efficacy of Nivolumab. About 30% of the patients had objective responses and the median response duration was 2 years. The authors hypothesize that the ongoing tumor response following Nivolumab discontinuation, and unlike following chemotherapy, may be due to PD-1 blockade, resulting in the establishment of immune memory response, as is seen after antigen exposure against specific infectious organisms. The most common adverse events of any grade were fatigue, rash and diarrhea. These toxicities were not cumulative. The authors concluded that Nivolumab improved Overall Survival in patients with advanced melanoma and the clinical benefit was durable and persisted even after the drug was discontinued. Studies are underway combining Nivolumab with a different checkpoint inhibitor, YERVOY®. The synergy between these two agents may result in even better outcomes. Topalian SL, Sznol M, McDermott DF, et al. J Clin Oncol 2014;32:1020-1030
Combined BRAF and MEK Inhibition in Melanoma with BRAF V600 Mutations
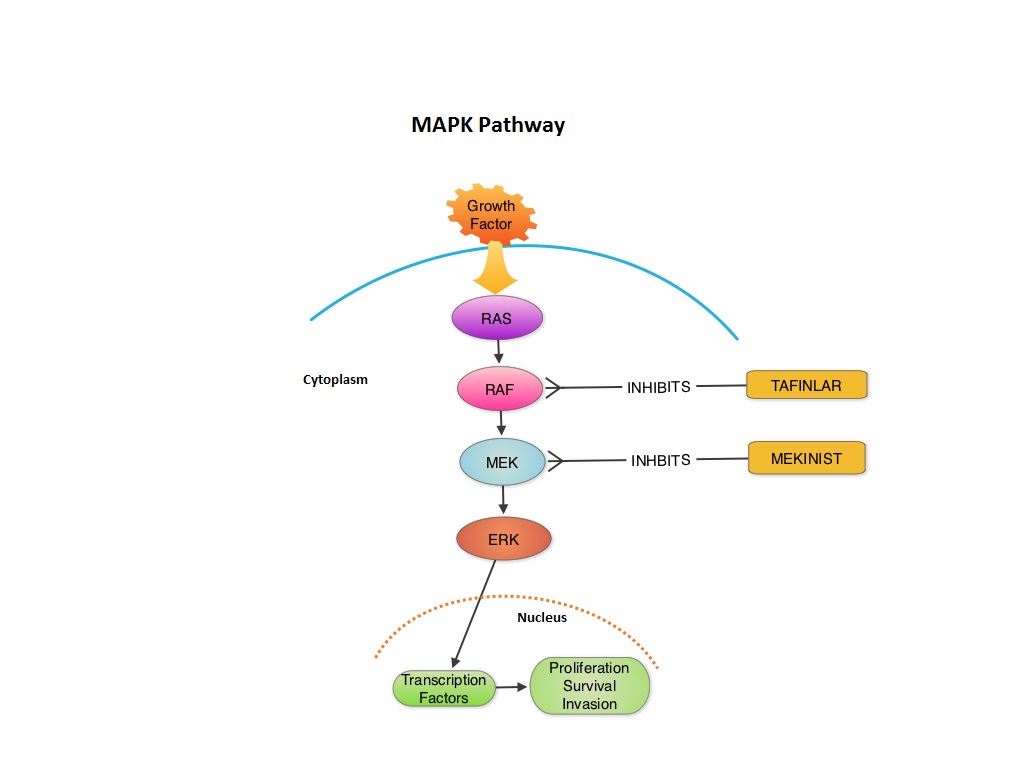
SUMMARY:The FDA granted accelerated approval in January 2014, for a combination of MEKINIST® (Trametinib) and TAFINLAR® (Dabrafenib), to treat patients with advanced melanoma, based on the understanding of the biological pathways of this malignancy. The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. BRAF mutations have been demonstrated in 6%-8% of all malignancies. The most common BRAF mutation in melanoma is at the V600E site and is detected in approximately 50% of melanomas. In the BREAK-3 randomized phase III trial, TAFINLAR®, a selective oral BRAF inhibitor demonstrated a statistically significant improvement in Progression Free Survival (PFS) and Response Rate (RR) compared to Dacarbazine (DTIC) in patients with advanced BRAF V600E mutated melanoma. Squamous cell carcinoma’s were seen in 6% of the patients. In the METRIC phase III study, MEKINIST®, a potent and selective inhibitor of MEK gene (which is downstream from RAF in the MAPK pathway) was compared with either Dacarbazine or TAXOL® (Paclitaxel) in advanced melanoma patients with BRAF V600E/K mutations. Patients in the MEKINIST® group had a significantly improved PFS, RR and Overall Survival. Based on the understanding of the biological pathways of the disease and different mechanisms of action (MOA) of these two agents, a phase I and II trial was conducted combining TAFINLAR® and MEKINIST®. In this study, 162 treatment naïve patients with unresectable or metastatic melanoma, with BRAF V600E or V600K mutations received either TAFINLAR® 150 mg plus MEKINIST® 1 or 2 mg or TAFINLAR® alone. Treatment was given until disease progression or side effects were intolerable. The primary end points were the incidence of Cutaneous Squamous-cell carcinoma, PFS and RR. Secondary end points included Overall Survival and pharmacokinetic activity. The combination treatment resulted in a lower incidence of Cutaneous Squamous-cell carcinoma (7% vs 19% in those receiving monotherapy, P=0.09), improved median PFS (9.4 months vs 5.8 months in the monotherapy group, HR=0.39, P<0.001) and superior complete or partial responses (76% compared with 54% with monotherapy (P=0.03). Pyrexia was however more common in the combination group than in the monotherapy group (71% vs. 26%). The authors concluded that by combining two agents with different MOA’s targeting two different tyrosine kinases in the RAS/RAF/MEK/ERK pathway, PFS was significantly improved. Further, development of resistance can be overcome in BRAF mutation positive melanoma patients and the incidence of secondary skin cancers found with BRAF inhibitor monotherapy can be reduced as well. Flaherty KT, Infante JR, Daud A, et al. N Engl J Med 2012;367:1694-1703
MEKINIST® (Trametinib) in combination with TAFINLAR® (Dabrafenib)
The FDA on January 10, 2014 approved the use of MEKINIST® in combination with TAFINLAR® for the treatment of patients with unresectable or metastatic melanoma with BRAF V600E or V600K mutation, as detected by an FDA-approved test. Both MEKINIST® and TAFINLAR® are products of GlaxoSmithKline, LLC.
Safety and Tumor Responses with Lambrolizumab (Anti–PD-1) in Melanoma
SUMMARY:Lambrolizumab (MK-3475) is a humanized anti–PD-1 monoclonal antibody. The programmed death 1 (PD-1) receptor is an inhibitory receptor expressed on activated T-cells in the tumor micro environment. The anti–PD-1 antibody by blocking the PD-1 receptor essentially unleashes the immune system to fight off cancer cells. One hundred and thirty five patients with advanced melanoma regardless of their prior therapy with YERVOY® (Ipilimumab) received IV Lambrolizumab every 2-3 weeks. There was no difference in the response rates between patients who had prior therapy with YERVOY® and those who did not (38%). Majority of these patients had a rapid and durable response. The median progression-free survival was more than 7 months. The most common adverse events, mostly low grade were, fatigue, rash, pruritus, and diarrhea. The authors concluded that Lambrolizumab can significantly benefit patients with advanced Malignant Melanoma, regardless of their prior therapy with anti-CTLA 4 antibody, YERVOY® and with minimal toxicity. Hamid O, Robert C, Daud A, et al. N Engl J Med 2013; 369:134-144
MEKINIST® (Trametinib)
MEKINIST® (Trametinib): The FDA on May 29, 2013 approved the use of MEKINIST® tablet for the treatment of patients with unresectable or metastatic melanoma with BRAF V600E or V600K mutation, as detected by an FDA-approved test. The FDA also approved the THxID BRAF assay (bioMerieux, Inc.) for detection of BRAF V600E and V600K mutations. MEKINIST® is not indicated for treatment of patients who had received prior BRAF inhibitor therapy. MEKINIST® is a product of GlaxoSmithKline, LLC.
TAFINLAR® (Dabrafenib)
TAFINLAR® (Dabrafenib): The FDA on May 29, 2013 approved the use of TAFINLAR® capsule for the treatment of patients with unresectable or metastatic melanoma with BRAF V600E mutation as detected by an FDA-approved test. TAFINLAR® is not indicated for the treatment of patients with wild-type BRAF melanoma because of the potential risk of tumor proliferation. The FDA also approved the THxID BRAF assay (bioMerieux, Inc.) for detection of BRAF V600E mutations. TAFINLAR® is a product of GlaxoSmithKline, LLC.
Phase III, randomized, open-label, multicenter trial (BREAK-3) comparing the BRAF kinase inhibitor dabrafenib (GSK2118436) with dacarbazine (DTIC) in patients with BRAFV600E-mutated melanoma
SUMMARY:The Mitogen- Activated Protein kinase pathway (MAP kinase pathway) is an important signaling pathway which enables the cell to respond to external stimuli. There are a number of MAP kinase pathways, which share different proteins at each step. The MAP kinase pathway plays a dual role regulating cytokine production and participating in cytokine dependent signaling cascade. The MAP kinase pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAS family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. BRAF mutations have been demonstrated in 6%-8% of all malignancies. The most common BRAF mutation in melanoma is at the V600E site and is detected in approximately 50% of melanomas.The BREAK-3 trial is a randomized phase III trial, with the study design similar to that of the Vemurafenib BRIM-3 trial. Dabrafenib is a selective oral BRAF inhibitor. Patients with advanced BRAFV600E mutated melanoma were randomized to receive either Dabrafenib or Dacarbazine (DTIC). Primary endpoint was Progression Free Survival (PFS) and secondary endpoints included Overall Survival (OS), Response Rate (RR) and duration of response. The median PFS was 5.1 months for Dabrafenib and 2.7 months for DTIC (hazard ratio = 0.30; P< 0.0001). RR was 53% for Dabrafenib and 19% for DTIC. OS data was not mature for analysis. Squamous cell carcinomas were seen in 6% of the patients. Hauschild A, Grob JJ, Demidov LV, et al. J Clin Oncol. 2012:30(suppl; abstr LBA8500).
METRIC phase III study Efficacy of trametinib (T), a potent and selective MEK inhibitor (MEKi), in progression-free survival (PFS) and overall survival (OS), compared with chemotherapy (C) in patients (pts) with BRAFV600E/K mutant advanced or metastatic melanoma (MM)
SUMMARY: The Mitogen- Activated Protein kinase pathway (MAP kinase pathway) is an important signaling pathway which enables the cell to respond to external stimuli. There are a number of MAP kinase pathways, which share different proteins at each step. The MAP kinase pathway plays a dual role regulating cytokine production and participating in cytokine dependent signaling cascade. The MAP kinase pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAS family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. BRAF mutations have been demonstrated in 6%-8% of all malignancies. The most common BRAF mutation in melanoma is at the V600E site and is detected in approximately 50% of melanomas. Vemurafenib is a novel oral inhibitor of mutated BRAF. However, Vemurafenib may increase the risk of developing a secondary malignancy (squamous cell carcinoma). Trametinib is a very potent and selective inhibitor of MEK gene and by seeking out this mechanism of action, there is probably a lower risk of another activated event ie. secondary malignancies. This is because MEK is downstream from RAF in the MAP Kinase pathway. In a phase III trial, patients with advanced melanoma with BRAF V600E/K mutations and without brain metastases were randomized to receive Trametinib or chemotherapy (either dacarbazine or paclitaxel). Patients receiving chemotherapy were allowed to crossover to receive Trametinib if they had documented progression. Primary endpoint was Progression Free Survival (PFS) and secondary endpoints included Overall Survival (OS), Response Rate (RR) and safety. The outcomes were in favor of Trametinib with a PFS of 4.8 months vs 1.4 months (HR =0.44; P<0.0001), RR of 24% vs 7%, with a 47% reduction in the risk of death compared to chemotherapy. Robert C, Flaherty KT, Hersey P, et al. J Clin Oncol. 2012:30(suppl; abstr LBA8509).