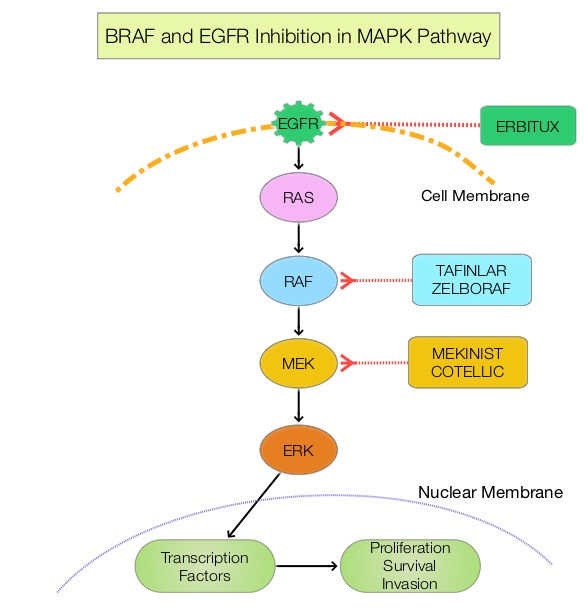
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of CRC will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%). Advanced colon cancer is often incurable and standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC, whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now also clear that even among the KRAS Wild Type patients, about 15-20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents.
MicroRNAs (MiRNA) are small non-coding RNA molecules that play a key role in the regulation of intracellular processes through post-transcriptional regulation of gene expression. It has been shown that MicroRNAs controlling expression of oncogenes and tumor suppressor genes are frequently deregulated in cancer cells. One MiRNA which is frequently deregulated in a variety of cancers is MiR-31, which is frequently overexpressed in colorectal cancer, with high expression correlating with advanced disease. A mature sequence of MiR-31, MiR-31-3p, has been shown to predict outcomes among for colorectal cancer patients treated with anti-EGFR therapy such as ERBITUX® and VECTIBIX®.
FIRE-3 is an open-label, randomized Phase III trial in which FOLFIRI plus ERBITUX® was compared with FOLFIRI plus AVASTIN®, as first line treatment in patients with metastatic ColoRectal Cancer (CRC). This study suggested that patients with KRAS exon 2 wild-type metastatic CRC had a longer Overall Survival (OS) when treated with FOLFIRI plus ERBITUX® compared with FOLFIRI plus AVASTIN®.
Based on the premise that MiR-31-3p expression has been shown to be associated with response to anti-EGFR therapy, in previously published studies, the authors investigated the predictive role of this biomarker in the FIRE-3 study patient population, in its ability to differentiate outcomes between patients receiving anti-EGFR and anti-VEGF therapy. In this study, MiR-31-3p expression was measured in primary tumors obtained from 340 RAS wild-type mCRC patients enrolled in the FIRE-3 Trial. The study population included 164 patients randomized to receive FOLFIRI plus ERBITUX® and 176 patients to FOLFIRI plus AVASTIN®. Patients were divided into subgroups, defined by Low or High MiR-31-3p expression.
It was noted that patients with Low MiR-31-3p expression benefited from ERBITUX® combination compared to AVASTIN® for PFS (HR=0.74;P=0.05), OS (HR=0.61;P<0.01) and Objective Response Rate (P<0.01). There was however no difference in outcomes among High MiR-31-3p expressors between the two treatment groups.
It was concluded that MiR-31-3p expression level is a validated predictive biomarker of anti EGFR therapy efficacy for RAS wild-type mCRC patients, and can enable clinicians to identify patients who would benefit from first-line anti-EGFR treatment. MiRNAs are well preserved in Formalin-Fixed Paraffin-Embedded (FFPE) tissues and MiR-31- 3p expression levels can be measured using RT qPCR. Validation of miR-31-3p Expression to Predict Cetuximab Efficacy When Used as First-Line Treatment in RAS Wild-Type Metastatic Colorectal Cancer. Laurent-Puig P, Grisoni ML, Heinemann V, et al. Clin Cancer Res. 2018 Aug 14. pii: clincanres.1324.2018. doi: 10.1158/1078-0432.CCR-18-1324. [Epub ahead of print]