
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 147,950 new cases of CRC will be diagnosed in the United States in 2020 and about 53,200 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23. Advanced colon cancer is often incurable and standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab), as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC (mCRC), whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now also clear that even among the KRAS Wild Type patient group about 15-20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Patients with Stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations. KRAS mutations are predictive of resistance to EGFR targeted therapy. Approximately 5-20% of all metastatic CRC tumors present with BRAF V600E mutations and BRAF V600E is recognized as a marker of poor prognosis in this patient group. These patients tend to have aggressive disease with a higher rate of peritoneal metastasis and do not respond well to standard treatment intervention. Approximately 20% of the BRAF-mutated population in the metastatic setting has MSI-High tumors, but MSI-High status does not confer protection to this patient group.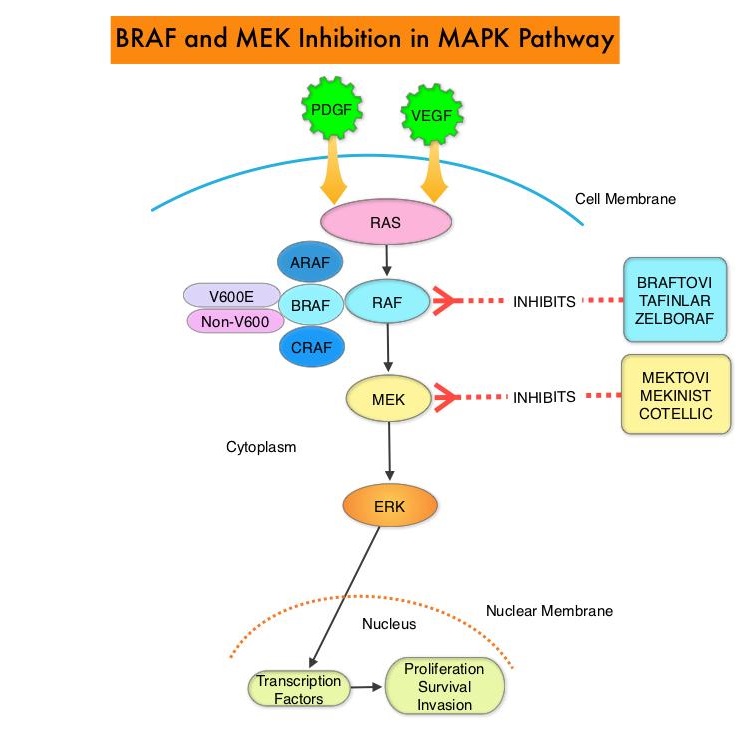
The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. The BRAF V600E mutations results in constitutive activation of the MAP kinase pathway. Inhibiting BRAF can transiently reduce MAP kinase signaling. However, this can result in feedback upregulation of EGFR signaling pathway, which can then reactivate the MAP kinase pathway. This aberrant signaling can be blocked by dual inhibition of both BRAF and EGFR. However, BRAF V600E-mutated CRC is inherently less sensitive to BRAF inhibition than melanoma. BRAFTOVI® (Encorafenib) is a BRAF inhibitor and has target binding characteristics that differ from other BRAF inhibitors such as ZELBORAF® (Vemurafenib) and TAFINLAR® (Dabrafenib), with a prolonged target dissociation half-life and higher potency. The combination of BRAFTOVI® along with anti-EGFR monoclonal antibody ERBITUX® (Cetuximab) showed promising activity in early-phase clinical trials.
The BEACON CRC (Binimetinib, Encorafenib, and Cetuximab Combined to Treat BRAF-Mutant Colorectal Cancer) trial is an international, multicenter, randomized, open-label, Phase III study in which the efficacy and safety of BRAFTOVI® plus ERBITUX® with or without a MEK inhibitor MEKTOVI® (Binimetinib), was compared with the investigators’ choice of ERBITUX® combined with either Irinotecan or Fluorouracil, Folinic acid, and Irinotecan, in patients with BRAF V600E-mutant mCRC, whose disease has progressed after one or two prior regimens. In this trial, 665 patients were randomly assigned in a 1:1:1 ratio to receive either triplet therapy of BRAFTOVI® 300 mg orally daily, MEKTOVI® 45 mg orally twice daily, and ERBITUX® 400 mg/m2 IV as an initial dose, then 250 mg/m2 IV weekly (N=224), doublet-therapy of BRAFTOVI® and ERBITUX® administered in the same doses and on the same schedule as the triplet regimen (N=220) or investigators’ choice of ERBITUX® combined with either Irinotecan or Fluorouracil, Folinic acid, and Irinotecan (N=221). Patients were stratified according to previous Irinotecan use and treatment was administered in 28-day cycles until disease progression. The co-Primary end points were Overall Survival (OS) in the triplet-therapy group as compared with the control group and Secondary end points included OS in the doublet-therapy group as compared with the control group, as well as PFS, Duration of Response, and Safety in all groups. This study was not powered to compare the triplet-therapy group against the doublet-therapy group.
At the time of prespecified interim analysis, with a median duration of follow up for survival at 7.8 months across the three groups, the median OS was 9.0 months in the triplet-therapy group and 5.4 months in the control group (HR for death=0.52; P<0.001). This represented 48% reduction in the risk of death in the triplet-therapy group. The confirmed Response Rate was 26% in the triplet-therapy group and 2% in the control group (P<0.001). The median OS in the doublet-therapy group was 8.4 months (HR for death versus control=0.60; P<0.001).
The authors in this updated analysis focused on the patient-reported Quality of Life (QOL) assessments from this study. QOL assessments using 4 validated QOL measures were secondary endpoints in the trial. They included EORTC QOL Questionnaire (QLQ C30), Functional Assessment of Cancer Therapy Colon Cancer (FACT C), EuroQol 5D 5L, and Patient Global Impression of Change (PGIC). The risk of QOL deterioration was reduced by 45% (HR=0.55) and 44% (HR=0.56), using EORTC QLQ C30 and FACT C assessments respectively, in favor of the triplet regimen over control. Similar findings were observed when the doublet-therapy regimen was compared with the regimen in the control group, and when QOL assessments were made using the other two QOL measures (EuroQol 5D 5L and PGIC). There was however no significant differences in QOL when the triplet and doublet regimen groups were compared.
It was concluded based on this updated analysis of the BEACON CRC trial, that among patients with BRAF V600E-mutant metastatic Colorectal Cancer, a combination of BRAFTOVI® plus ERBITUX® with or without a MEK inhibitor MEKTOVI®, demonstrated longer maintenance of QOL on patient-reported assessments, compared to the current standard of care. Encorafenib plus cetuximab with or without binimetinib for BRAF V600E-mutant metastatic colorectal cancer: Quality-of-life results from a randomized, three-arm, phase III study versus the choice of either irinotecan or FOLFIRI plus cetuximab (BEACON CRC). Kopetz S, Grothey A, Van Cutsem E, et al. J Clin Oncol. 2020;38(suppl 4; abstr 8).
Tag: Colon Cancer
Circulating Tumor DNA in the Peripheral Blood Predicts Recurrence Risk After Surgery and Adjuvant Chemotherapy in Stage III Colon Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 145,600 new cases of CRC were diagnosed in the United States in 2019 and about 51,020 patients died of the disease. The lifetime risk of developing CRC is about 1 in 23. Adjuvant chemotherapy for patients with resected, locally advanced, node-positive (Stage III) colon cancer has been the standard of care since the 1990s. Adjuvant treatment with an ELOXATIN® (Oxaliplatin) based chemotherapy regimen has been considered standard intervention since 2004, for patients with Stage III colon cancer, following surgical resection, and has been proven to decrease the chance of recurrent disease. Chemotherapy regimens have included (FOLFOX – Leucovorin, 5-FluoroUracil, ELOXATIN®) or CAPOX/XELOX (XELODA®/Capecitabine and ELOXATIN®), given over a period of 6 months. In spite of these advancements, defining patient subsets at high risk of recurrence following standard adjuvant therapy remains challenging and treatment failure can only be acknowledged when clinical recurrence is documented.
Cell-free DNA (cfDNA) refers to DNA molecules that circulate in the bloodstream after cell apoptosis or necrosis. A specific portion of cfDNA that originates from tumor cells is referred to as circulating tumor DNA (ctDNA), which can be detected in the cell-free component of peripheral blood samples in almost all patients with advanced solid tumors including advanced colorectal cancer. ctDNA is a valuable biomarker and allows early detection of relapse. Several studies have shown that detectable ctDNA following surgery for early stage cancers, is associated with a very high risk of recurrence. The authors in this publication report on the results of a correlative biomarker study in patients with Stage III colon cancer, undergoing standard adjuvant chemotherapy.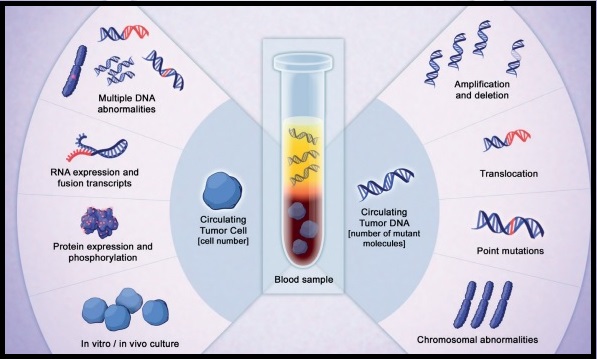
A multicenter, population-based, cohort study was conducted to determine whether serial post-surgical and post-chemotherapy ctDNA analysis could provide a real-time indication of efficacy of adjuvant therapy in Stage III colon cancer. In this study, 100 patients with newly diagnosed Stage III colon cancer who were planned to receive 24 weeks of adjuvant chemotherapy were enrolled. Patients had R0 resection with no evidence of metastatic disease on staging CT of the chest, abdomen, and pelvis before surgery. The chemotherapy regimen was chosen by the treating physician, who was blinded to the ctDNA result. High-risk patients were defined as those having pT4 and/or pN2 disease according to the pTNM staging system. Blood samples for ctDNA and CEA (CarcinoEmbryonic Antigen) analysis were collected 4-10 weeks after surgery prior to commencement of adjuvant chemotherapy and at the completion of adjuvant therapy, within 6 weeks of the final cycle of chemotherapy. All patients had a surveillance CT scan 4-8 weeks after completion of adjuvant chemotherapy. Follow up surveillance included clinical exam every 3 months along with CEA measurement and annual CT imaging for 3 years. Serial plasma samples were collected after surgery and after chemotherapy. Somatic mutations in individual patient tumors were identified by massively parallel sequencing of 15 genes commonly mutated in colorectal cancer, and personalized assays were designed to quantify ctDNA. For each patient, one mutation identified in the tumor tissue was assessed in the plasma for the presence of ctDNA. The median duration of follow up was 28.9 months and the primary aim of this study was to demonstrate the association between postsurgical and post-chemotherapy ctDNA detection and the risk of recurrence.
Among the 96 evaluable patients, circulating tumor DNA was detectable in 20 of 96 (21%) post-surgical samples and these patients had an increased risk of recurrence with associated inferior Recurrence-Free Survival, (HR=3.8; P<0.001). The estimated 3 year Recurrence Free Interval (RFI) for patients with positive ctDNA findings was 47% and for those with ctDNA-negative findings was 76%. Circulating tumor DNA was detectable in 15 of 88 (17%) post-chemotherapy samples. The estimated 3 year RFI was 30% when ctDNA was detectable after chemotherapy and 77% when ctDNA was undetectable (HR=6.8; P<0.001). Postsurgical ctDNA status was an independent predictor of disease recurrence after adjusting for known clinicopathologic risk factors (HR=7.5; P<0.001).
The authors concluded that post-surgical and post-chemotherapy circulating tumor DNA analyses is a promising prognostic marker in Stage III colon cancer, and may identify patients at high risk of recurrence, despite completing standard adjuvant treatment. This high-risk population presents a unique opportunity to explore additional therapeutic approaches. Circulating Tumor DNA Analyses as Markers of Recurrence Risk and Benefit of Adjuvant Therapy for Stage III Colon Cancer. Tie J, Cohen JD, Wang Y, et al. JAMA Oncol. 2019;5:1710-1717.
NCCN updates Colorectal Cancer Testing and Treatment Guidelines
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 145,600 new cases of CRC will be diagnosed in the United States in 2019 and about 51,020 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23. Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable with a 5-year survival rate of 11%.
The 2019 NCCN guideline update for colon cancer has expanded the scope of personalized medicine and clinical diagnostics by incorporating biomarker testing to guide treatment. With the identification of new biomarkers and expansion of biomarker testing to guide treatment among patients with colorectal cancer, studies are underway to classify colorectal cancer (CRC) based on comprehensive gene expression profiles. The Consensus Molecular Subtypes (CMS) is one of the most robust transcriptome-based classification of colorectal cancer (CRC). The CMS subtype may influence the efficacy of chemotherapy and CMS might be a new predictive factor for the efficacy of chemotherapy against mCRCs. The CRC Subtyping Consortium (CRCSC) initiated by 15 institutions analyzed more than 30 different gene expression sets across multiple platforms and sample preparation methods and identified four different molecular subtypes, CMS1, CMS2, CMS3 and CMS4. This covers approximately 87% of all CRC cases, thus leaving approximately 13% of cases molecularly uncharacterized.
CMS1: Approximately 14 percent of all CRC are considered CMS1, of which approximately 12 percent are sporadic (non-inherited), while the remaining patients have inherited disease (Lynch Syndrome). Tumors are located in the proximal colon, have a high BRAF V600E mutation rate and are associated with impaired DNA mismatch repair (MMR). Patients in this group tend to have a lower rate of relapse and if relapse does occur, they are associated with poor outcomes (about 9 months). The 5-year survival rate for this group is about 73%.
CMS2: This is the most common CRC subtype with approximately 39% of the CRC patients belonging to this group. Majority of the tumors are located in the left colon and tumors are characterized by the initial loss of APC, a tumor suppressor gene, followed by an activating mutation in KRAS and loss of TP53. Patients in this group have higher survival rates (35 months) after relapse. The 5-year survival rate for this group is 77%, the best among the four different CRC subtypes.
CMS3: Approximately 13 percent of CRC patients belong to this group. KRAS mutations are most frequently found in this patient group (68%) and approximately 3% of patients in this group overexpress HER2. Patients in this group have the second highest survival rates, with a 5-year survival rate of 75%.
CMS4: These tumors are characterized by MSS (MicroSatellite Stable) with frequent mutation of genes such as APC, KRAS, PIK3CA, and TP53. Patients in this group often have poor prognosis as they are diagnosed at advanced stages. They have little or no benefit from systemic adjuvant therapy and those with metastatic disease are often resistant to EGFR inhibitors, independent of KRAS mutation status. They have the worst 5-year Overall Survival (62%) of any molecular subtype.
The following are the key 2019 NCCN guideline updates
KRAS, NRAS and BRAF Mutation Testing
All patients with metastatic colorectal cancer should have tumor tissue genotyped for KRAS, NRAS and BRAF mutations individually or as a part of Next Generation Sequencing (NGS) panel
MicroSatellite Instability (MSI) or MisMatch Repair (MMR) Testing
1) The presence of BRAF V600E mutation in the setting of absence of MLH1 would preclude the diagnosis of Lynch Syndrome in a majority of cases. However, approximately 1% of cancers with BRAF V600E mutation and loss of MLH-1 are Lynch Syndrome and therefore, caution should be exercised, in excluding patients with a strong family history from germline screening in the case of BRAF V600E mutations
2) ImmunoHistoChemistry (IHC) refers to staining of tumor tissue for protein expression of the four mismatch repair MMR genes, MLH1, MSH2, MSH6, and PMS2, known to be mutated in Lynch Syndrome. A normal IHC test implies that all 4 MMR proteins are normally expressed or retained. An abnormal or positive IHC test implies loss or absence of expression of one or more of the 4 MMR proteins. When IHC is reported as positive, caution should be exercised to ensure that positive IHC refers to absence of mismatch expression and not presence of expression. Loss of expression by IHC in any of the MMR genes should then be followed up with genetic testing. Abnormal MLH1 on IHC should be followed by tumor testing for BRAF V600E mutation. The presence of BRAF V600 E mutation is consistent with sporadic cancer.
mFOLFOXIRI + EGFR
mFOLFOXIRI with EGFR inhibitor VECTIBIX® (Panitumumab) or ERBITUX® (Cetuximab) was added as a treatment option for unresectable stage IV mCRC that are left-sided and are KRAS/NRAS/BRAF wild-type.
mFOLFOX + EGFR
The combination regimen FOLFOX + VECTIBIX® or ERBITUX® was added for KRAS/NRAS/BRAF wild-type tumors.
Immunotherapy
Patients with advanced or metastatic CRC who are not appropriate candidates for intensive therapy may be offered OPDIVO® (Nivolumab) or KEYTRUDA® (Pembrolizumab), as a single agent or a combination of OPDIVO® and YERVOY® (Ipilimumab), only for tumors that are MMR deficient and MSI High (Category 2B). These same immunotherapy options are also listed in the guidelines as second and third-line options for MMR deficient and MSI High patients.
NTRK Gene Fusion
Tumors should be tested for Neurotrophic Receptor Tyrosine Kinase (NTRK) gene fusion, and VITRAKVI® (Larotrectinib) is now a second-line treatment option for patients with metastatic CRC that is NTRK gene fusion positive.
BRAF and MEK
BRAF wild-type was added as an indication for treatment, where KRAS and NRAS wild-type are noted. Combination therapies added to the guidelines as second-line options include
1) TAFINLAR® (Dabrafenib) targeting BRAF plus MEKINIST® (Trametinib) targeting MEK along with ERBITUX® or VECTIBIX® which are EGFR targeted monoclonal antibodies
2) BRAFTOVI® (Encorafenib) targeting BRAF plus MEKTOVI® (Binimetinib) targeting MEK along with ERBITUX® or VECTIBIX®.
NCCN Guidelines Updates: Management of Metastatic Colorectal Cancer. Messersmith WA. Presented at 2019 NCCN Annual Conference; March 21-23, 2019; Orlando, FL.
Duration of Oxaliplatin-Containing Adjuvant Therapy for Stage III Colon Cancer ASCO Clinical Practice Guideline
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 145,600 new cases of CRC will be diagnosed in the United States in 2019 and about 51,020 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Adjuvant chemotherapy for patients with resected, locally advanced, node-positive (Stage III) Colon Cancer, has been the standard of care since the 1990s. Adjuvant treatment with an ELOXATIN® (Oxaliplatin) based chemotherapy regimen has been considered standard intervention since 2004, for patients with Stage III colon cancer, following surgical resection, and has been proven to decrease the chance of recurrent disease. Chemotherapy regimens have included (FOLFOX – Leucovorin, 5-FluoroUracil, ELOXATIN®) or CAPOX/XELOX (XELODA®/Capecitabine and ELOXATIN®), given over a period of 6 months. ELOXATIN® can however be associated with neuropathy which can be long lasting or permanent, depending on the duration of therapy. Additional toxicities with longer duration of chemotherapy include diarrhea, fatigue as well as more office visits.
This ASCO Clinical Practice Guideline was based on the IDEA Collaboration, which is a prospective, pre-planned pooled analysis of 6 concurrently conducted randomized phase III trials, which included 12,834 patients from 12 countries. The goal of this study was to determine if 3 months of adjuvant chemotherapy would be as effective as 6 months of therapy and would be non-inferior. Approximately, 40% of patients received CAPOX regimen and 60% received FOLFOX regimen. The Primary endpoint was Disease Free Survival (DFS).
In an exploratory subgroup analyses by risk of recurrence within the high-risk group defined in the IDEA Collaboration (T4 – tumor invades through the visceral peritoneum including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum or tumor directly invades or adheres to other adjacent organs or structures and/or N2 – metastasis in 4 or more regional lymph nodes), superior DFS was found with 6 months versus 3 months duration of ELOXATIN® based adjuvant chemotherapy. In the low-risk group however, (T1-tumor invades submucosa, T2-tumor invades muscularis propria, or T3-tumor invades through the muscularis propria into the pericolorectal tissues and N1-metastasis in 1-3 regional lymph nodes), DFS was noninferior with 3 months versus 6 months duration of adjuvant chemotherapy.
In prespecified subgroup analysis by type of ELOXATIN®-based chemotherapy, 3 months of treatment was non-inferior to 6 months for patients treated with CAPOX regimen. However, 3 months of treatment was inferior to 6 months, for patients treated with FOLFOX regimen. It has been hypothesized that the protracted delivery of a Fluoropyrimidine with CAPOX might have been more effective than the twice-monthly 5-FUinfusions with FOLFOX as an adjuvant therapy. Grade 2 or more neurotoxicity was significantly lower for patients who received 3 months of adjuvant therapy versus 6 months (P <0.0001), regardless of the treatment regimen (17% vs 48% for FOLFOX and 15% vs 45% for CAPOX/XELOX, respectively).
It was concluded from this study that a risk-based approach has to be taken when making adjuvant chemotherapy recommendations for patients with Stage III Colon Cancer, taking into consideration choice of treatment regimen and duration of therapy. In patients treated with adjuvant CAPOX/XELOX regimen, 3 months of therapy was as effective as 6 months, particularly in the low risk subgroup. In patients treated with FOLFOX, 6 months of adjuvant therapy compared to 3 months, resulted in a higher rate of Disease Free Survival, particularly in the high-risk subgroup.
Guideline Question: What is the optimal duration (3 months vs 6 months) of ELOXATIN®-based chemotherapy for patients with completely resected Stage III Colon Cancer?
Target Population: Patients with completely resected Stage III Colon Cancer. Target Audience: Medical oncologists, general surgeons, colorectal surgeons, surgical oncologists, and oncology Advanced Practice Providers who treat patients with Colon Cancer.
Methods: A multidisciplinary Expert Panel which included clinicians with expertise in colorectal surgery and medical oncology as well as a patient representative and an ASCO guidelines health research expert, was convened to develop clinical practice guideline recommendations, based on a systematic review of the medical literature from April 2004 to August 2018, for Phase III randomized clinical trials (RCTs) that included a comparison of two or more durations of treatment with FOLFOX or CAPOX chemotherapy.
Recommendations for patients with Stage III resected Colon Cancer who are being offered treatment with ELOXATIN®-based chemotherapy.
Recommendation 1: For patients with High-risk (T4 and/or N2) Stage III resected Colon Cancer, adjuvant ELOXATIN®-based chemotherapy should be offered for a duration of 6 months.
Recommendation 2: For patients with Low-risk (T1, T2, or T3 and N1) Stage III resected Colon Cancer, adjuvant ELOXATIN®-based chemotherapy may be offered for a duration of 3 months or 6 months, after a discussion with the patient of the potential benefits and risks of harm associated with the options for treatment duration.
Recommendation 3: A shared decision-making approach should be used for duration of ELOXATIN®-based chemotherapy for patients with Stage III resected Colon Cancer, taking into account a patient’s tumor characteristics, completeness of surgical resection, number of lymph nodes examined, comorbidities, functional status, performance status, values and preferences, age at diagnosis, life expectancy, potential years at risk for long-term sequelae of treatment, and including a discussion of the potential for benefit and risks of harm associated with treatment duration.
Duration of Oxaliplatin-Containing Adjuvant Therapy for Stage III Colon Cancer: ASCO Clinical Practice Guideline.Lieu C, Kennedy EB, Bergsland E, J Clin Oncol. 2019;37:1436-1447.
Dramatic Increase in ColoRectal Cancer Incidence among Young Adults
Even though the incidence of Colorectal cancer (CRC) in the United States has been rapidly declining overall, primarily driven by screening, the incidence however has been increasing among adults younger than 50 years of age, according to data in the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program. Based on these findings, the American Cancer Society in 2018 updated its guidelines to include a “qualified recommendation” to begin CRC screening at the age of 45 yrs.
In a recently published retrospective study, the proportion of the total number of patients diagnosed with CRC under the age of 50 yrs rose from 10% in 2004 to 12.2% in 2015 (P<0.0001). Younger adults presented with more advanced stage of disease (Stage III/IV) than those 50 yrs or older (51.6% versus 40.0% respectively). When racial and ethnic groups were stratified by sex, among men with a diagnosis of CRC before age 50, non‐Hispanic whites showed a proportional increase in diagnosis (P<0.0001), whereas among women, both Hispanic whites (P<0.05) and non‐Hispanic whites (P<0.001) had increases in the proportion of CRC diagnosed before age 50. The rates of CRC diagnosis in young adults increased over time, regardless of income level (P<0.001).The highest proportion of young adult CRC diagnoses occurred in the highest income group. The proportion of CRC cases diagnosed in younger individuals rose in urban areas (P<0.001), but not in rural areas. Health Care Providers should be mindful of these data, when screening guidelines are discussed with patients.
Dramatic Increase in ColoRectal Cancer Incidence among Young Adults
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 145,600 new cases of CRC will be diagnosed in the United States in 2019 and about 51,020 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Even though the incidence of Colorectal cancer (CRC) in the United States has been rapidly declining overall, primarily driven by screening, the incidence however has been increasing among adults younger than 50 years of age, according to data in the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) program. Based on these findings, the American Cancer Society in 2018 updated its guidelines to include a “qualified recommendation” to begin CRC screening at the age of 45 yrs. The US Preventive Services Task Force (USPSTF) and other major US organizations have however not yet changed their recommendations. The increase in the incidence of CRC in young adults has been attributed to western style, high carbohydrate, high fat, low fiber diet, which can initiate inflammation and proliferation in the colonic mucosa within two weeks. Other lifestyle factors associated with CRC include obesity, high consumption of processed meat and alcohol, low levels of physical activity and cigarette smoking.
The authors in this publication performed a retrospective study examining the National Cancer Data Base (NCDB) registry to determine whether the trends seen through 2013, as published from SEER program had continued to worsen through 2015 (the most recent available data from the NCDB). The National Cancer Data Base is one of the largest cancer registries in the world and includes more than 70% of newly diagnosed cancer cases in the United States and more than 34 million historical records. The researchers also examined available demographic and socioeconomic factors to determine whether they were related to CRC in young adults and further compared clinical characteristics of CRC tumors among age groups, to determine whether younger patients had differences in clinical presentation. A total of 1,185,763 cases were included in the study of whom 130,165 patients were diagnosed at an age younger than 50 yrs and 1,055,598 patients were diagnosed at the age of 50 yrs or older. The proportion of patients diagnosed before the age of 50 yrs was chosen as the Primary endpoint, as most current guidelines recommend screening starting at an age of 50 yrs.
The proportion of the total number of patients diagnosed with CRC under the age of 50 yrs rose from 10% in 2004 to 12.2% in 2015 (P<0.0001). Younger adults presented with more advanced stage of disease (Stage III/IV) than those 50 yrs or older (51.6% versus 40.0% respectively). When racial and ethnic groups were stratified by sex, among men with a diagnosis of CRC before age 50, nonâ€Hispanic whites showed a proportional increase in diagnosis (P<0.0001), whereas among women, both Hispanic whites (P<0.05) and nonâ€Hispanic whites (P<0.001) had increases in the proportion of CRC diagnosed before age 50. The rates of CRC diagnosis in young adults increased over time, regardless of income level (P<0.001).The highest proportion of young adult CRC diagnoses occurred in the highest income group. The proportion of CRC cases diagnosed in younger individuals rose in urban areas (P<0.001), but not in rural areas.
It was concluded that based on this study, that the proportion of individuals diagnosed with CRC at an age younger than 50 years, has continued to increase over the past decade in the US. Younger adults also present with more advanced disease and Health Care Providers should be mindful of these data, when screening guidelines are discussed with patients. This study however does not capture oncogenic mutations or tumor laterality, which are known to affect the prognosis. The authors pointed out that the National Cancer Data Base which provided the patient information for this study currently captures laterality only for paired organs. Recent trends in the age at diagnosis of colorectal cancer in the US National Cancer Data Base, 2004â€2015. Virostko J, Capasso A, Yankeelov TE, et al. First published: 22 July 2019. https://doi.org/10.1002/cncr.32347
BRAFTOVI®, MEKTOVI® and ERBITUX® Triplet Therapy for Patients with BRAF V600E-Mutant Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 145,600 new cases of CRC will be diagnosed in the United States in 2019 and about 51,020 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23. Advanced colon cancer is often incurable and standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC (mCRC), whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now also clear that even among the KRAS Wild Type patient group about 15-20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Patients with stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations. KRAS mutations are predictive of resistance to EGFR targeted therapy. Approximately 8-15% of all metastatic CRC tumors present with BRAF V600E mutations and BRAF V600E is recognized as a marker of poor prognosis in this patient group. These patients tend to have aggressive disease with a higher rate of peritoneal metastasis and do not respond well to standard treatment intervention. Approximately 20% of the BRAF-mutated population in the metastatic setting has MSI-High tumors, but MSI-High status does not confer protection to this patient group.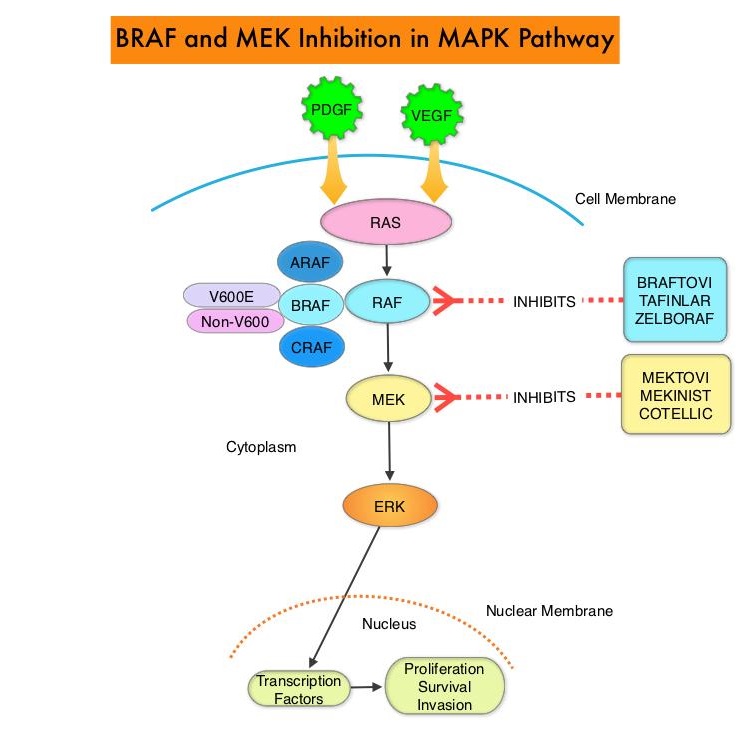
The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. The BRAF V600E mutations results in constitutive activation of the MAP kinase pathway. Inhibiting BRAF can transiently reduce MAP kinase signaling. However, this can result in feedback upregulation of EGFR signaling pathway, which can then reactivate the MAP kinase pathway. This aberrant signaling can be blocked by dual inhibition of both BRAF and EGFR. However, BRAF V600E-mutated CRC is inherently less sensitive to BRAF inhibition than melanoma.
The FDA approved BRAFTOVI® (Encorafenib) and MEKTOVI® (Binimetinib) in combination for the first-line treatment of patients with BRAF V600-mutant melanoma, in June 2018. In a recent Phase II study among previously treated patients with BRAF V600E-mutant mCRC, treatment with a combination of BRAFTOVI® plus ERBITUX® resulted in an Objective Response Rate (ORR) of 24%, PFS of 4.2 months, and OS of 9.3 months. These results were significantly better than the standard of care, as well as other BRAF, MEK, and EGFR-inhibitor triplet combinations. Preclinical data suggests that BRAFTOVI® has target binding characteristics that differ from other BRAF inhibitors such as ZELBORAF® (Vemurafenib) and TAFINLAR® (Dabrafenib), with a prolonged target dissociation half-life and higher potency. This may explain the superior efficacy of BRAFTOVI® over other BRAF inhibitors in BRAF V600E-mutated CRC. These encouraging results with the BRAFTOVI® plus ERBITUX® doublet led to the initiation of the Phase III BEACON CRC study.
The BEACON Colorectal Cancer trial is an open-label, randomized, three-arm, Phase III study in which the efficacy and safety of BRAFTOVI® plus ERBITUX® with or without MEKTOVI® was compared with the investigators’ choice of ERBITUX® combined with either Irinotecan or Fluorouracil, Folinic acid, and Irinotecan, in patients with BRAF V600E-mutant mCRC whose disease has progressed after one or two prior regimens. At the time BEACON CRC was initiated, the triplet combination of MEKTOVI®, BRAFTOVI®, and ERBITUX® had not been clinically evaluated. The authors therefore conducted a Safety Lead-In (SLI) to determine the Safety, tolerability, and preliminary efficacy of this triplet combination at the same doses planned for the randomized portion of the trial.
The randomized portion of the trial was ongoing at the time of this analysis. The BEACON trial included patients with mCRC whose tumor tissue was positive for the presence of BRAF V600E mutation. Majority of the patients had right-sided disease as is characteristic of BRAF V600E-mutant mCRC, with a high frequency of nodal and peritoneal metastasis. Liver however, was the most frequent site of metastasis. Enrolled patients must have had progressive disease on one, but no more than two prior treatment regimens, in the metastatic setting. Enrolled patients received BRAFTOVI® 300 mg PO daily plus MEKTOVI® 45 mg PO BID along with ERBITUX® 400 mg/m2 IV, followed by 250 mg/m2 IV weekly every 28 days. The Safety Lead-In was initiated before the randomized portion of the BEACON trial and included 30 patients with disease characteristics and treatment schedule as described above. The Primary end point was Safety, including the incidence of dose-limiting toxicities. Efficacy end points included Overall Response Rate, Progression Free Survival, and Overall Survival.
The median follow up was 18.2 months, and the median time on study drug was 7.9 months. The confirmed Overall Response Rate was 48%, median Duration of Response was 5.5 months, median Progression Free Survival was 8.0 months, and median Overall Survival was 15.3 months. Approximately 79% of responding patients achieved a response within 2 months. The most common adverse events were nausea, diarrhea, fatigue and dermatitis. Approximately 6% of patients experienced serous retinopathy without loss of visual acuity.
It was concluded that in this Safety Lead-In, the combination regimen of BRAFTOVI®, MEKTOVI® and ERBITUX® resulted in promising results compared with available therapies, among patients with previously treated BRAF V600E-mutant mCRC, and if confirmed in the randomized portion of the trial, could become the new standard of care in this patient group. Binimetinib, Encorafenib, and Cetuximab Triplet Therapy for Patients With BRAF V600E–Mutant Metastatic Colorectal Cancer: Safety Lead-In Results From the Phase III BEACON Colorectal Cancer Study. Van Cutsem E, Huijberts S, Grothey A, et al. Journal of Clinical Oncology 2019; 37:1460-1469.
STIVARGA® Dose Optimization Improves Outcomes in Patients with Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of CRC will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%). Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable. STIVARGA® (Regorafenib), is an oral multi-kinase inhibitor and inhibits multiple kinases including VEGF1, VEGF2, VEGF3, PDGFR, FGFR involved in tumor angiogenesis and KIT, RET, RAF-1, BRAF involved in oncogenesis. STIVARGA® is approved by the FDA for the treatment of patients with metastatic CRC, who have progressed on 5FU, ELOXATIN® (Oxaliplatin), CAMPTOSAR® (Irinotecan), anti-VEGF and anti-EGFR therapies, at a dose of 160 mg orally, once daily for the first 21 days of each 28-day cycle. The approval was based on a phase III trial in which patients receiving STIVARGA® had a statistically significant improvement in the Overall Survival (OS) and Progression Free Survival (PFS), compared to placebo.
The starting dose of STIVARGA® has been an obstacle and toxicities such as Palmar-Plantar Erythrodysesthesia Syndrome (PPES) commonly occurring during the first 2 weeks, as well as fatigue and hypertension have limited its use. Various dosing schedules have been implemented into clinical practice, despite the absence of reliable supportive data. There is therefore a need to optimize the dose of STIVARGA® in patients with refractory mCRC to maintain efficacy, while improving the tolerability profile. CORRELATE study looked at the data from the real-world setting of refractory mCRC regarding the dosing of STIVARGA® and safety, whereas the ReDos study evaluated a dose-escalation strategy, starting with a lower dose of STIVARGA®.
CORRELATE is a prospective, international observational study conducted in 13 countries to evaluate the use STIVARGA® in a real-world setting, based on safety and efficacy. The primary objective of this study was to assess safety. This final analysis describes the real-world dosing of STIVARGA® in mCRC.
Of the 1037 patients included in this study, 57% started treatment at 160 mg, 30% at 120 mg, and 13% at 80 mg or less. The mean dose administered was 75% of the approved dose. The median patient age was 65 years and majority of the patients had an ECOG performance status (PS) of 0-1 (87%). Dose reductions were more frequent in the 160 versus 120 mg group and treatment modifications were most commonly due to treatment related adverse events (66%). Most treatment discontinuations (49%) were due to radiologic disease progression, whereas 19% were due to STIVARGA® related adverse events. Treatment related adverse events of any grade occurred in 95% of patients, and 80% were attributed to STIVARGA®. Median overall survival (OS) was 7.6 months and the estimated 1-year OS was 34%.
It was concluded from this real-world, observational study that the starting dose of STIVARGA® for nearly half of patients was less than 160 mg/day and the common treatment related adverse events were generally consistent with the known safety profile of STIVARGA® in mCRC. Despite the dose modifications of STIVARGA®, there was no significant impact on its efficacy in terms of the median OS and median PFS.
ReDOS is a randomized phase II study in which STIVARGA® dose-escalation strategy beginning at a lower starting dose of 80 mg daily and ending at 160 mg daily was compared with the standard dose, in patients with refractory mCRC. In this dose escalation study, patients in Arm A (N=54) received STIVARGA® 80 mg daily, with weekly dose escalation up to 160 mg daily, if no significant drug-related toxicities were experienced, where as in Arm B (N=62), patients received the standard dose of STIVARGA® 160 mg daily, for 21 days of a 28-day cycle. The median age was 61 years and both treatment groups were well balanced. The Primary endpoint was the proportion of patients who completed 2 cycles of treatment and initiated the 3rd cycle if there was no progression.
The study met its primary endpoint with 43% of patients on Arm A initiating the 3rd cycle versus only 25% of patients on Arm B (P=0.028). The median Overall Survival (OS) was improved in Arm A versus Arm B (9 months versus 5.9 months ; P=0.094). The median Progression Free Survival (PFS) was 2.5 months for Arm A and 2 months for Arm B (P=0.55). Overall grade 3 and 4 toxicities were lower on Arm A versus Arm B and multiple Quality Of Life parameters were improved in Arm A versus Arm B, at week 2 of the first cycle.
It was concluded that weekly dose escalation of STIVARGA® from 80 mg to 160 mg daily was superior to a starting dose of 160 mg daily. Based on this study, the NCCN has updated its ColoRectal Cancer (CRC) guidelines, recommending a weekly STIVARGA® dose-escalation strategy beginning at 80 mg and ending at 160 mg, for previously treated patients with metastatic ColoRectal Cancer.
Real-world dosing of regorafenib (REG) in metastatic colorectal cancer (mCRC): final results from the prospective, observational CORRELATE study. O'Connor JM, Ducreux M, Petersen LN, et al. Ann Oncol. 2018;29 (suppl_8): viii150-viii204. 10.1093/annonc/mdy281
Regorafenib dose optimization study (ReDOS): Randomized phase II trial to evaluate dosing strategies for regorafenib in refractory metastatic colorectal cancer (mCRC)-an ACCRU Network study. Bekaii-Saab TS, Ou FS, Anderson DM, et al. J Clin Oncol. 2018;36(suppl 4S; abstr 611)
BRAF V600E Mutation is a Very Poor Prognostic Factor in Metastatic Colorectal Carcinoma
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of CRC will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%). Advanced colon cancer is often incurable and standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC, whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now also clear that even among the KRAS Wild Type patients, about 15-20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Patients with stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations. KRAS mutations are predictive of resistance to Epidermal Growth Factor Receptor (EGFR) targeted therapy. Approximately 5-10% of all metastatic CRC tumors present with BRAF V600E mutations and BRAF V600E is recognized as a marker of poor prognosis in this patient group. These patients tend to have aggressive disease with a higher rate of peritoneal metastasis and do not respond well to standard treatment intervention. Approximately 25% of the BRAF-mutated population in the metastatic setting has MSI-High tumors, but MSI-High status does not confer protection to this patient group.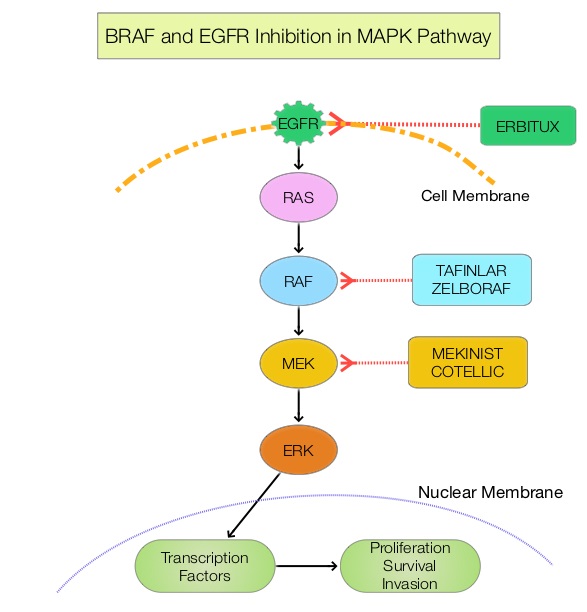
The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. The BRAF V600E mutations results in constitutive activation of the MAP kinase pathway. Inhibiting BRAF can transiently reduce MAP kinase signaling. However, this can result in feedback upregulation of EGFR signaling pathway, which can then reactivate the MAP kinase pathway. This aberrant signaling can be blocked by dual inhibition of both BRAF and EGFR.
ZELBORAF® (Vemurafenib), is a selective oral inhibitor of mutated BRAF whereas ERBITUX® is a monoclonal antibody targeting Epidermal Growth Factor Receptor (EGFR). In a phase II SWOG trial (SWOG 1406), the addition of ZELBORAF® to the combination of CAMPTOSAR® (Irinotecan) and ERBITUX® resulted in a 58% reduction in the risk of disease progression and a higher Disease Control Rate, suggesting that simultaneous EGFR and BRAF inhibition (Dual Inhibition) is effective in BRAF V600 mutated ColoRectal Cancer.
Unlike primary colorectal cancer, the association of BRAF V600E and non-V600E mutations with survival and tumor recurrence after resection of ColoRectal Liver Metastases (CRLM), has remained unclear. This present study was conducted to investigate the prognostic association of BRAF mutations with survival and recurrence independently, and to understand how BRAF mutations compared with other prognostic determinants, such as KRAS mutations. This cohort study enrolled 853 patients with colorectal tumors and liver metastases, of whom 849 patients were evaluable and included in the study analyses. All patients underwent resection of their ColoRectal Liver Metastases with a curative intent from January 1, 2000, through December 31, 2016, at institutions participating in the International Genetic Consortium for Colorectal Liver Metastasis and had available data on BRAF and KRAS mutational status. The median age was 60 years, and 60% were male. The main outcomes and measures were the association of BRAF V600E and non-V600E mutations with Disease Free Survival (DFS) and Overall Survival (OS).
Forty three patients (5.1%) had a mutated BRAF (V600E and non-V600E) /wild-type KRAS genotype, 480 patients (56.5%) had wild-type BRAF/wild-type KRAS genotype; and 326 patients (38.4%) had a wild-type BRAF/mutated KRAS genotype. Compared with the wild-type BRAF/wild-type KRAS genotype group, patients with a mutated BRAF/wild-type KRAS genotype more frequently were female (62.8% vs 35.2%) and 65 years or older (51.2% vs 36.9%), had right-sided primary tumors (62.8% vs 17.4%), and presented with a metachronous liver metastasis (64.3% vs 46.8%). The median follow up was 28.3 months.
On multivariable analysis, the presence of BRAF V600E but not non-V600E mutation was associated with significantly poor Overall Survival (HR=2.76; P<0.001) and Disease Free Survival (HR=2.04; P=0.002). Compared with KRAS mutation, the BRAF V600E mutation had a stronger association with OS and DFS than the KRAS mutations.
It was concluded that the presence of BRAF V600E mutation was associated with worse prognosis and increased risk of recurrence, and BRAF V600E mutation was not only a stronger prognostic factor than KRAS but also was the strongest prognostic determinant in the overall cohort. It remains to be seen if BRAF V600E mutated metastatic colorectal tumors would have better outcomes with targeted triplet combination therapies such as ZELBORAF® CAMPTOSAR® and ERBITUX® or TAFINLAR® (Dabrafenib-BRAF inhibitor), MEKINIST® (Trametinib-MEK inhibitor) and VECTIBIX®. Association of BRAF Mutations With Survival and Recurrence in Surgically Treated Patients With Metastatic Colorectal Liver Cancer. Margonis, GA, Buettner, S, Andreatos, N, et al. JAMA Surg. 2018;153(7):e180996. doi:10.1001/jamasurg.2018.0996
MicroRNA-31-3p Expression is a Predictive Biomarker of Anti-EGFR Efficacy in Patients with RAS Wild-type Metastatic Colorectal Cancer
Advanced ColoRectal Cancer (CRC) is often incurable and standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC, whose tumors do not harbor RAS mutations. It is now becoming clear that among these pan RAS wild type tumors, a predictive biomarker, MiR-31-3p expression in tumors, may further determine who would benefit from Anti-EGFR targeted therapy.
In a recently published study (Clin Cancer Res 2018), tumors with Low MiR-31-3p expression benefited from ERBITUX® combination compared to AVASTIN® for PFS (HR=0.74;P=0.05), OS (HR=0.61;P<0.01) and Objective Response Rate (P<0.01). There was however no difference in outcomes among High MiR-31-3p expressors between the two treatment groups. This study suggested that only low MiR-31-3p expressing tumors among the pan RAS wild type CRC patients benefit from Anti-EGFR targeted therapies.