
SUMMARY: The FDA on December 19, 2017 granted accelerated approval to BOSULIF® (Bosutinib) for treatment of patients with newly diagnosed Chronic Phase Philadelphia chromosome positive (Ph+) Chronic Myelogenous Leukemia (CML). Chronic Myeloid Leukemia (CML) constitutes a little over 10% of all new cases of leukemia. The American Cancer Society estimates that about 8,950 new CML cases will be diagnosed in the United States in 2017 and about 1,080 patients will die of the disease. The hallmark of CML, the Philadelphia Chromosome (Chromosome 22), is a result of a reciprocal translocation between chromosomes 9 and 22, wherein the ABL gene from chromosome 9 fuses with the BCR gene on chromosome 22. As a result, the auto inhibitory function of the ABL gene is lost and the BCR-ABL fusion gene is activated resulting in cell proliferation and leukemic transformation of hematopoietic stem cells. The presently available Tyrosine Kinase Inhibitors (TKI’s) approved in the United States including GLEEVEC® (Imatinib), share the same therapeutic target, which is BCR-ABL kinase. BOSULIF® is a potent, dual Abl and Src tyrosine kinase inhibitor and was approved by the FDA in 2012 for the treatment of adult patients with chronic, accelerated, or blast phase Philadelphia chromosome positive (Ph+) Chronic Myelogenous Leukemia (CML) with resistance or intolerance to prior therapy.
 This new approval for BOSULIF® was based on the efficacy and safety data from BFORE trial, which is an ongoing randomized, open-label, multicenter, phase III study in which in 487 patients with Ph+ newly diagnosed Chronic Phase CML were randomized to receive either BOSULIF® 400 mg once daily (N=246) or GLEEVEC® (Imatinib) 400 mg once daily (N=241). The median age of patients was 53 years, the Sokal risk group was intermediate and high for 40% and 21% of patients, respectively, and over two thirds of the patients had an ECOG PS score of 0. Sokal score is calculated using a formula that includes Age, Spleen size, Platelet count and percentage of Myeloblasts and has three risk groups: Low-risk (Sokal score<0.8), Intermediate-risk (Sokal score 0.8-1.2) and High-risk (Sokal score >1.2). The Primary endpoint was Major Molecular Response (MMR) at 12 months, defined as BCR-ABL ratio on International Scale of 0.1% or less, which corresponded to 3 or more log reduction from standardized baseline.
This new approval for BOSULIF® was based on the efficacy and safety data from BFORE trial, which is an ongoing randomized, open-label, multicenter, phase III study in which in 487 patients with Ph+ newly diagnosed Chronic Phase CML were randomized to receive either BOSULIF® 400 mg once daily (N=246) or GLEEVEC® (Imatinib) 400 mg once daily (N=241). The median age of patients was 53 years, the Sokal risk group was intermediate and high for 40% and 21% of patients, respectively, and over two thirds of the patients had an ECOG PS score of 0. Sokal score is calculated using a formula that includes Age, Spleen size, Platelet count and percentage of Myeloblasts and has three risk groups: Low-risk (Sokal score<0.8), Intermediate-risk (Sokal score 0.8-1.2) and High-risk (Sokal score >1.2). The Primary endpoint was Major Molecular Response (MMR) at 12 months, defined as BCR-ABL ratio on International Scale of 0.1% or less, which corresponded to 3 or more log reduction from standardized baseline.
After 12 or more months of follow up, the MMR at 12 months was 47.2% in the BOSULIF® group and 36.9% in the GLEEVEC® group (P=0.02) and the time to achieve a MMR was shorter in the BOSULIF® group (P<0.02). The Complete Cytogenetic Response (CCyR) at 12 months was also significantly higher with BOSULIF® versus GLEEVEC® (77.2% vs 66.4%; P< 0.008), with the time to achieve a CCyR, shorter for BOSULIF® (P<0.001). The most common adverse reactions in the BOSULIF® group included rash, nausea, diarrhea, abdominal discomfort, thrombocytopenia, increased ALT and AST levels.
It was concluded that BOSULIF® is an important and useful treatment option for patient with newly diagnosed Chronic Phase CML. Bosutinib (BOS) versus imatinib (IM) for newly diagnosed chronic myeloid leukemia (CML): Initial results from the BFORE trial. Cortes JE, Gambacorti-Passerini C, Deininger MWN, et al. J Clin Oncol. 2017;35 (suppl; abstr 7002).
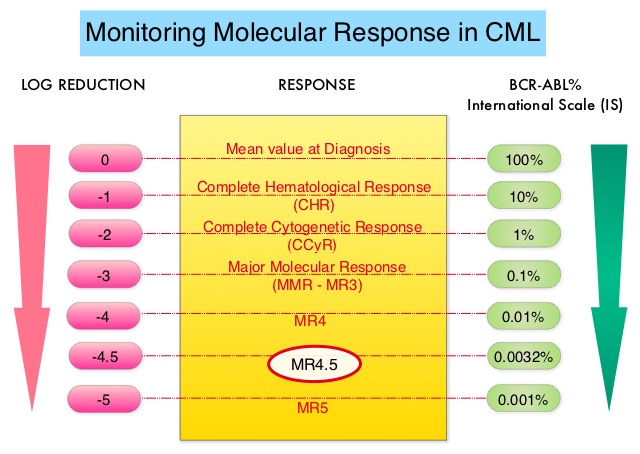
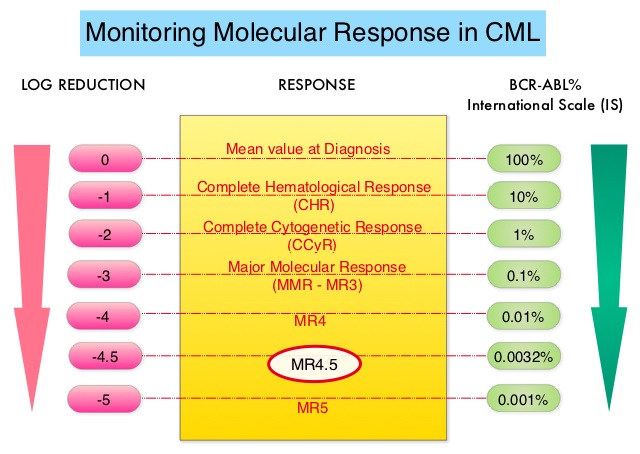
 The presently available Tyrosine Kinase Inhibitors (TKI’s) approved in the United States including GLEEVEC®, share the same therapeutic target, which is BCR-ABL kinase. Resistance to TKI’s can occur as a result of mutations in the BCR-ABL kinase domain or amplification of the BCR-ABL gene. With the availability of newer therapies for CML, monitoring response to treatment is important. This is best accomplished by measuring the amount of residual disease using Reverse Transcription-Polymerase Chain Reaction (RT-PCR). Molecular response in CML is expressed using the International Scale (IS) as BCR-ABL%, which is the ratio between BCR-ABL and a control gene. BCR-ABL kinase domain point mutations are detected, using the mutational analysis by Sanger sequencing. Majority of the patients receiving a TKI following diagnosis of CML achieve a Complete Cytogenetic Response (CCyR) within 12 months following commencement of therapy and these patients have a life expectancy similar to that of their healthy counterparts. Previously published studies have shown that deep molecular response (MR4.5) is a new molecular predictor of long term survival in CML patients and was achieved in a majority of patients treated with optimized dose of GLEEVEC®. It has been hypothesized based on previous observations, that a subgroup of CML patients experiencing deeper responses (MR3, MR4, and MR4.5), may stay in unmaintained remission even after treatment discontinuation. Despite this observation, stopping CML therapy is currently not a clinical recommendation and should only be considered in the context of a clinical trial.
The presently available Tyrosine Kinase Inhibitors (TKI’s) approved in the United States including GLEEVEC®, share the same therapeutic target, which is BCR-ABL kinase. Resistance to TKI’s can occur as a result of mutations in the BCR-ABL kinase domain or amplification of the BCR-ABL gene. With the availability of newer therapies for CML, monitoring response to treatment is important. This is best accomplished by measuring the amount of residual disease using Reverse Transcription-Polymerase Chain Reaction (RT-PCR). Molecular response in CML is expressed using the International Scale (IS) as BCR-ABL%, which is the ratio between BCR-ABL and a control gene. BCR-ABL kinase domain point mutations are detected, using the mutational analysis by Sanger sequencing. Majority of the patients receiving a TKI following diagnosis of CML achieve a Complete Cytogenetic Response (CCyR) within 12 months following commencement of therapy and these patients have a life expectancy similar to that of their healthy counterparts. Previously published studies have shown that deep molecular response (MR4.5) is a new molecular predictor of long term survival in CML patients and was achieved in a majority of patients treated with optimized dose of GLEEVEC®. It has been hypothesized based on previous observations, that a subgroup of CML patients experiencing deeper responses (MR3, MR4, and MR4.5), may stay in unmaintained remission even after treatment discontinuation. Despite this observation, stopping CML therapy is currently not a clinical recommendation and should only be considered in the context of a clinical trial.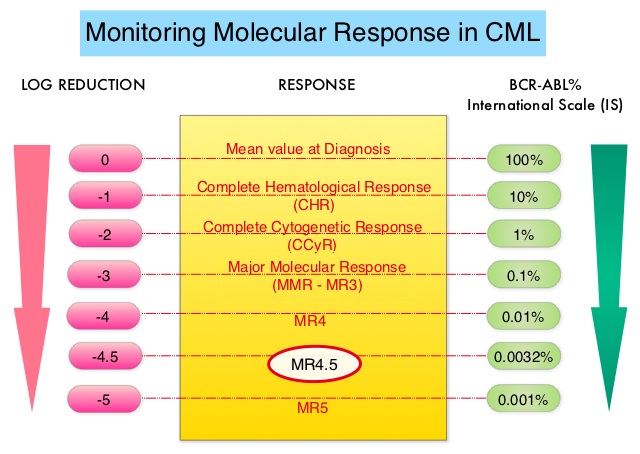


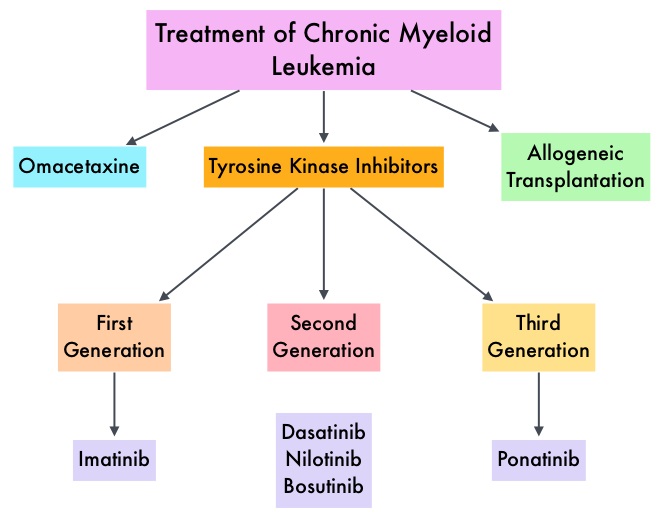
 Gleevec® (Imatinib) inhibits the BCR-ABL tyrosine kinase and is the standard first line treatment, of Ph chromosome positive (Ph+) leukemias. Lack of response due to resistance to GLEEVEC® and in some instances drug intolerance, has led to the development of newer agents including Second and Third generation Tyrosine Kinase Inhibitors (TKIs). Resistance to Gleevec® and other TKIs sharing the same therapeutic target (BCR-ABL kinase), has been attributed to point mutations in the ABL kinase domain, amplification of the BCR-ABL gene as well as other BCR- ABL independent mechanisms such as upregulation of SRC kinases. Mutation analysis at the time of TKI failure, utilizing high sensitivity sequencing techniques such as Next Generation Sequencing, can give clinically relevant information related to low level mutations and compound mutations and this information in turn, can dictate choice of second line therapy.
Gleevec® (Imatinib) inhibits the BCR-ABL tyrosine kinase and is the standard first line treatment, of Ph chromosome positive (Ph+) leukemias. Lack of response due to resistance to GLEEVEC® and in some instances drug intolerance, has led to the development of newer agents including Second and Third generation Tyrosine Kinase Inhibitors (TKIs). Resistance to Gleevec® and other TKIs sharing the same therapeutic target (BCR-ABL kinase), has been attributed to point mutations in the ABL kinase domain, amplification of the BCR-ABL gene as well as other BCR- ABL independent mechanisms such as upregulation of SRC kinases. Mutation analysis at the time of TKI failure, utilizing high sensitivity sequencing techniques such as Next Generation Sequencing, can give clinically relevant information related to low level mutations and compound mutations and this information in turn, can dictate choice of second line therapy.  The Second generation TKIs, TASIGNA® (Nilotinib) and SPRYCEL® (Dasatinib) although initially approved for second line treatment of CML after GLEEVEC® resistance or intolerance, are now FDA approved for the treatment of newly diagnosed Chronic Phase CML. This approval was based on the rapid and superior Major Molecular Responses (MMR) noted, when compared to GLEEVEC®. Now, that the Second generation TKIs are being used as first line therapy, the choice of second line therapy after failure with Second generation TKIs has become more nebulous. It is clear however that, patients with primary cytogenetic resistance to ï¬rst and second line therapy do not beneï¬t from sequential therapy with Second generation TKIs and BCR-ABL mutation analysis should be performed in all patients who develop TKI resistant disease. Before switching from a Second to a Third generation TKI such as Ponatinib, the following considerations should be taken into account
The Second generation TKIs, TASIGNA® (Nilotinib) and SPRYCEL® (Dasatinib) although initially approved for second line treatment of CML after GLEEVEC® resistance or intolerance, are now FDA approved for the treatment of newly diagnosed Chronic Phase CML. This approval was based on the rapid and superior Major Molecular Responses (MMR) noted, when compared to GLEEVEC®. Now, that the Second generation TKIs are being used as first line therapy, the choice of second line therapy after failure with Second generation TKIs has become more nebulous. It is clear however that, patients with primary cytogenetic resistance to ï¬rst and second line therapy do not beneï¬t from sequential therapy with Second generation TKIs and BCR-ABL mutation analysis should be performed in all patients who develop TKI resistant disease. Before switching from a Second to a Third generation TKI such as Ponatinib, the following considerations should be taken into account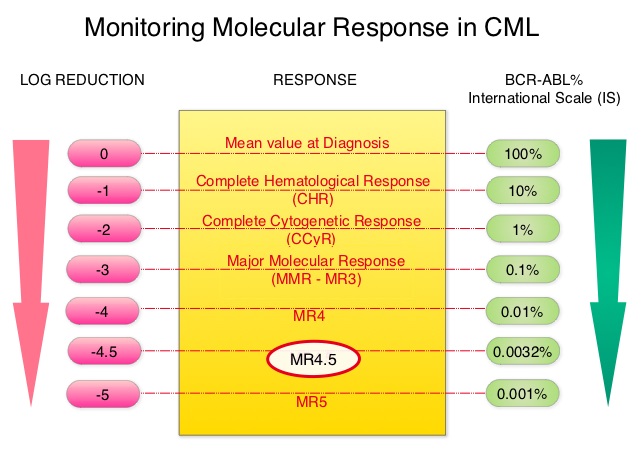 This is expressed using the International Scale (IS) as BCR-ABL%, which is the ratio between BCR-ABL and a control gene. BCR-ABL kinase domain point mutations are detected, using the mutational analysis by Sanger sequencing. Majority of the patients receiving a TKI following diagnosis of CML achieve a Complete Cytogenetic Response (CCyR) within 12 months following commencement of therapy and these patients have a life expectancy similar to that of their healthy counterparts. However, some patients have deeper responses (MR3, MR4, and MR4.5) and it is presumed that this subgroup of patients with CML may stay in unmaintained remission even after treatment discontinuation. Moreover, it is not clear what proportion of patients with CML achieve deeper responses and deeper responses have not been shown to increase survival beyond that associated with CCyR. To address these questions, the authors in this report analyzed the data from the randomized CML – Study IV to characterize the frequency and impact of deep molecular response on survival with different treatment modalities. The study is a five arm trial in which the treatment groups included high dose Imatinib (GLEEVEC® 800 mg/day), GLEEVEC® 400 mg/day, GLEEVEC® 400 mg/day in combination with Interferon alfa (IFN), GLEEVEC® 400 mg/day in combination with Cytarabine, and GLEEVEC® 400 mg/day after IFN failure. The analysis included a total of 1538 patients and the principal objective of CML – Study IV was to determine the impact of MMR (Major Molecular Response) on survival, remission rates and survival probabilities. After a median follow up of 67.5 months, 5 year overall survival was 90%, 8 year overall survival was 86% and 5 year PFS was 87.5%. The cumulative rate of MR4.5, irrespective of treatment group (defined as 4.5 or more log reduction in BCR-ABL transcripts), was 66% at 8 years and 70% at 9 years and the median time to reaching MR4.5 was 4.9 years. High dose GLEEVEC® therapy and early Major Molecular Remission predicted deep molecular response (MR4.5). High dose GLEEVEC® resulted in a more rapid MR4.5 than with GLEEVEC® 400 mg/day (P = .016). Finally, this analysis showed that a confirmed MR4.5 at 4 years predicted significantly higher 8 year overall survival probability compared to CCyR (Complete Cytogenetic response: IS 1%) or MMR (major molecular response: IS 0.1%) – 92% versus 83%, P=0.047. The authors concluded that deep molecular response (MR4.5) is a new molecular predictor of long term survival in CML patients and is achieved in a majority of patients treated with GLEEVEC®, and is achieved more rapidly with optimized high-dose GLEEVEC®. The authors further pointed out that none of the patients with confirmed MR4.5 had disease progression and this may therefore provide a therapeutic rationale for discontinuing treatment in this subset of patients with CML. These findings may also justify the use of more effective second generation TKI’s to induce early and deep molecular responses. Hehlmann R, Müller MC, Lauseker M, et al. J Clin Oncol 2014;32:415-423
This is expressed using the International Scale (IS) as BCR-ABL%, which is the ratio between BCR-ABL and a control gene. BCR-ABL kinase domain point mutations are detected, using the mutational analysis by Sanger sequencing. Majority of the patients receiving a TKI following diagnosis of CML achieve a Complete Cytogenetic Response (CCyR) within 12 months following commencement of therapy and these patients have a life expectancy similar to that of their healthy counterparts. However, some patients have deeper responses (MR3, MR4, and MR4.5) and it is presumed that this subgroup of patients with CML may stay in unmaintained remission even after treatment discontinuation. Moreover, it is not clear what proportion of patients with CML achieve deeper responses and deeper responses have not been shown to increase survival beyond that associated with CCyR. To address these questions, the authors in this report analyzed the data from the randomized CML – Study IV to characterize the frequency and impact of deep molecular response on survival with different treatment modalities. The study is a five arm trial in which the treatment groups included high dose Imatinib (GLEEVEC® 800 mg/day), GLEEVEC® 400 mg/day, GLEEVEC® 400 mg/day in combination with Interferon alfa (IFN), GLEEVEC® 400 mg/day in combination with Cytarabine, and GLEEVEC® 400 mg/day after IFN failure. The analysis included a total of 1538 patients and the principal objective of CML – Study IV was to determine the impact of MMR (Major Molecular Response) on survival, remission rates and survival probabilities. After a median follow up of 67.5 months, 5 year overall survival was 90%, 8 year overall survival was 86% and 5 year PFS was 87.5%. The cumulative rate of MR4.5, irrespective of treatment group (defined as 4.5 or more log reduction in BCR-ABL transcripts), was 66% at 8 years and 70% at 9 years and the median time to reaching MR4.5 was 4.9 years. High dose GLEEVEC® therapy and early Major Molecular Remission predicted deep molecular response (MR4.5). High dose GLEEVEC® resulted in a more rapid MR4.5 than with GLEEVEC® 400 mg/day (P = .016). Finally, this analysis showed that a confirmed MR4.5 at 4 years predicted significantly higher 8 year overall survival probability compared to CCyR (Complete Cytogenetic response: IS 1%) or MMR (major molecular response: IS 0.1%) – 92% versus 83%, P=0.047. The authors concluded that deep molecular response (MR4.5) is a new molecular predictor of long term survival in CML patients and is achieved in a majority of patients treated with GLEEVEC®, and is achieved more rapidly with optimized high-dose GLEEVEC®. The authors further pointed out that none of the patients with confirmed MR4.5 had disease progression and this may therefore provide a therapeutic rationale for discontinuing treatment in this subset of patients with CML. These findings may also justify the use of more effective second generation TKI’s to induce early and deep molecular responses. Hehlmann R, Müller MC, Lauseker M, et al. J Clin Oncol 2014;32:415-423