
The FDA on October 29, 2024, granted accelerated approval to SCEMBLIX® (Asciminib) for adult patients with newly diagnosed Philadelphia chromosome-positive Chronic Myeloid Leukemia (Ph+ CML) in Chronic Phase (CP). SCEMBLIX® is a product of Novartis AG.
Tag: Chronic Myeloid Leukemia
FDA Grants Accelerated Approval to SCEMBLIX® for Newly Diagnosed Chronic Myeloid Leukemia
SUMMARY: The FDA on October 29, 2024, granted accelerated approval to Asciminib (SCEMBLIX®), for adult patients with newly diagnosed Philadelphia Chromosome-positive Chronic Myeloid Leukemia (CML) in chronic phase. The American Cancer Society estimates that about 9,280 new CML cases will be diagnosed in the United States in 2024 and about 1,280 patients will die of the disease. Chronic Myeloid Leukemia constitutes about 15% of all new cases of leukemia and the average age at diagnosis of CML is around 64 years. The hallmark of CML, the Philadelphia Chromosome (Chromosome 22), is a result of a reciprocal translocation between chromosomes 9 and 22, wherein the ABL gene from chromosome 9 fuses with the BCR gene on chromosome 22. As a result, the auto inhibitory function of the ABL gene is lost and the BCR-ABL fusion gene is activated resulting in cell proliferation and leukemic transformation of hematopoietic stem cells.
The Tyrosine Kinase Inhibitors (TKIs) approved for newly diagnosed chronic phase CML in the United States share the same therapeutic target, which is the ATP-binding site of BCR-ABL1 kinase. They include first-generation TKI Imatinib (GLEEVEC®) or second-generation TKIs Nilotinib (TASIGNA®), Dasatinib (SPRYCEL®), or Bosutinib (BOSULIF®). Imatinib is associated with lower patient response and a higher incidence of disease progression than those with second-generation TKIs, whereas treatment with second-generation TKIs can result in faster, deeper molecular responses than Imatinib in frontline therapy, but are associated with more adverse events, necessitating dose modifications and switching treatments. Further, close to 50% of clinical resistance is associated with the acquisition of mutations in this region of the kinase, resulting in conformational changes that render TKIs inactive. Therefore, resistance to one of the TKIs, will likely result in resistance to the others as well. Further, the “gatekeeper” T315I mutation, which has been reported in 20% of patients with mutations, confers resistance to all clinically available TKIs except Ponatinib (ICLUSIG®). There is therefore an unmet need for safe and effective frontline therapy for patients with newly diagnosed chronic phase CML
Asciminib (SCEMBLIX®) is a novel, first-in-class, potent and specific, oral BCR-ABL1 inhibitor that does not bind to the ATP-binding site of the kinase. Instead, it specifically targets the ABL1 myristoyl pocket, also known as a STAMP (Specifically Targeting the ABL Myristoyl Pocket) inhibitor, with activity against native unmutated BCR-ABL1, and all clinically observed ATP-site mutants, including T315I. In a Phase I study, Asciminib was active in heavily pretreated patients with CML who had resistance to or unacceptable side effects from TKIs, including patients in whom Ponatinib had failed, and those with a T315I mutation.
Asciminib was previously approved by the FDA in the US for the treatment of adults with Philadelphia Chromosome positive chronic phase CML who have previously been treated with two or more TKIs. It is also approved in patients with Philadelphia Chromosome positive chronic phase CML with the T315I mutation.
The ASC4FIRST study is a pivotal Phase III, multi-center, open-label, randomized trial aimed at evaluating the efficacy and safety of Asciminib compared to investigator-selected Tyrosine Kinase Inhibitors (TKIs) in adult patients with newly diagnosed Philadelphia chromosome positive Chronic Myeloid Leukemia in chronic phase (CML-CP). A total of 405 patients were enrolled and were randomly assigned in a 1:1 ratio to receive either Asciminib 80 mg orally once daily (N=201) or investigator-selected TKIs which included Imatinib and second generation TKIs such as Bosutinib, Dasatinib or Nilotinib given at approved doses (N=204). Before randomization, investigators, after discussing with patients, selected a TKI (either Imatinib or one of the second-generation TKIs a patient would take, if randomly assigned to the comparator group-prerandomization selected TKI), considering treatment goals, disease and patient characteristics, and coexisting conditions. Randomization was stratified by European Treatment and Outcome Study long-term survival score category (low, intermediate, or high risk), and by TKI selected by investigators before randomization. The two Primary objectives of this study were to compare the efficacy of Asciminib with that of investigator-selected TKIs (all members of this class considered together as a group), and to compare the efficacy of Asciminib with that of Imatinib. Asciminib was not compared with second-generation TKIs as a primary objective. The Primary end point for both objectives was Major Molecular Response (defined as BCR/ABL1 transcript levels 0.1% or less on the International Scale at week 48 that did not meet any treatment failure criteria). The Secondary objective of this study was assessment of Major Molecular Response (MMR) at week 48 with Asciminib, as compared with investigator-selected TKIs among patients with second-generation TKIs as their prerandomization-selected TKI. The median follow-up was 16.3 months in the Asciminib group and 15.7 months in the investigator-selected TKI group.
At the 48-week mark, Asciminib demonstrated a significantly higher MMR rate compared to investigator-selected TKIs (67.7% versus 49.0%; P<0.001). Deep molecular response rates (BCR/ABL1 transcript levels 0.01% or less, were also superior in the Asciminib group compared to investigator-selected TKIs (38.8% versus 20.6%). Patients preselected for Imatinib who were randomized to Asciminib achieved an MMR rate of 69.3% compared to 40.2% in the Imatinib group (P<0.001). Among those preselected for second-generation TKIs, the MMR rate was 66.0% for Asciminib versus 57.8% for the second-generation TKI group.
Asciminib exhibited a favorable safety profile with fewer Grade 3 or higher Adverse Events and lower rates of treatment discontinuation due to Adverse Events. Grade 3 or higher Adverse Events for Asciminib was 38%, for Imatinib was 44.4% and for second-generation TKIs was 54.9%. Discontinuation due to Adverse Events for Asciminib was 4.5%, for Imatinib was 11.1% and for Second-generation TKIs was 9.8%.
It was concluded that Asciminib is the only agent to demonstrate superiority over investigator selected standard-of-care TKIs in achieving higher MMR rates at 48 weeks in newly diagnosed chronic phase CML patients, alongside a better safety and tolerability profile. These findings indicate that Asciminib could significantly improve the treatment landscape for this group of patients, offering hope for better disease control and quality of life, thereby addressing key unmet needs in CML management.
Asciminib in Newly Diagnosed Chronic Myeloid Leukemia. Hochhaus A, Wang J, Kim DD, et al. for the ASC4FIRST Investigators. N Engl J Med 2024;391:885-898.
Late Breaking Abstract – ASCO 2024: SCEMBLIX® Superior to Other TKIs in Newly Diagnosed Chronic Myeloid Leukemia
SUMMARY: The American Cancer Society estimates that about 9,280 new CML cases will be diagnosed in the United States in 2024 and about 1,280 patients will die of the disease. Chronic Myeloid Leukemia (CML) constitutes about 15% of all new cases of leukemia and the average age at diagnosis of CML is around 64 years. The hallmark of CML, the Philadelphia Chromosome (Chromosome 22), is a result of a reciprocal translocation between chromosomes 9 and 22, wherein the ABL gene from chromosome 9 fuses with the BCR gene on chromosome 22. As a result, the auto inhibitory function of the ABL gene is lost and the BCR-ABL fusion gene is activated resulting in cell proliferation and leukemic transformation of hematopoietic stem cells.
The Tyrosine Kinase Inhibitors (TKIs) approved for newly diagnosed chronic phase CML in the United States share the same therapeutic target, which is the ATP-binding site of BCR-ABL1 kinase. They include first-generation TKI Imatinib (GLEEVEC®) or second-generation TKIs Nilotinib (TASIGNA®), Dasatinib (SPRYCEL®), or Bosutinib (BOSULIF®). Imatinib is associated with lower patient response and a higher incidence of disease progression than those with second-generation TKIs, whereas treatment with second-generation TKIs can result in faster, deeper molecular responses than Imatinib in frontline therapy, but are associated with more adverse events, necessitating dose modifications and switching treatments. Further, close to 50% of clinical resistance is associated with the acquisition of mutations in this region of the kinase, resulting in conformational changes that render TKIs inactive. Therefore resistance to one of the TKIs, will likely result in resistance to the others as well. Further, the “gatekeeper” T315I mutation, which has been reported in 20% of patients with mutations, confers resistance to all clinically available TKIs except Ponatinib (ICLUSIG®). There is therefore an unmet need for a safe and effective frontline therapy for patients with newly diagnosed chronic phase CML
Asciminib (SCEMBLIX®) is a novel, first-in-class, potent and specific, oral BCR-ABL1 inhibitor that does not bind to the ATP-binding site of the kinase. Instead, it specifically targets the ABL1 myristoyl pocket, also known as a STAMP (Specifically Targeting the ABL Myristoyl Pocket) inhibitor, with activity against native unmutated BCR-ABL1, and all clinically observed ATP-site mutants, including T315I. In a Phase I study, Asciminib was active in heavily pretreated patients with CML who had resistance to or unacceptable side effects from TKIs, including patients in whom Ponatinib had failed, and those with a T315I mutation.
Asciminib is approved in the US for the treatment of adults with Philadelphia Chromosome positive chronic phase CML who have previously been treated with two or more TKIs. It is also approved in patients with Philadelphia Chromosome positive chronic phase CML with the T315I mutation.
The ASC4FIRST study is a pivotal Phase III, multi-center, open-label, randomized trial aimed at evaluating the efficacy and safety of Asciminib compared to investigator-selected Tyrosine Kinase Inhibitors (TKIs) in adult patients with newly diagnosed Philadelphia chromosome positive Chronic Myeloid Leukemia in chronic phase (CML-CP). A total of 405 patients were enrolled and were randomly assigned in a 1:1 ratio to receive either Asciminib 80 mg orally once daily (N=201) or investigator-selected TKIs which included Imatinib and second generation TKIs such as Bosutinib, Dasatinib or Nilotinib given at approved doses (N=204). Before randomization, investigators after discussing with patients selected a TKI (either Imatinib or one of the second-generation TKIs a patient would take, if randomly assigned to the comparator group-prerandomization selected TKI), considering treatment goals, disease and patient characteristics, and coexisting conditions. Randomization was stratified by European Treatment and Outcome Study long-term survival score category (low, intermediate, or high risk), and by TKI selected by investigators before randomization. The two Primary objectives of this study were to compare the efficacy of Asciminib with that of investigator-selected TKIs (all members of this class considered together as a group), and to compare the efficacy of Asciminib with that of Imatinib. Asciminib was not compared with second-generation TKIs as a primary objective. The Primary end point for both objectives was Major Molecular Response (defined as BCR/ABL1 transcript levels 0.1% or less on the International Scale at week 48 that did not meet any treatment failure criteria. The Secondary objective of this study was assessment of Major Molecular Response (MMR) at week 48 with Asciminib, as compared with investigator-selected TKIs among patients with second-generation TKIs as their prerandomization-selected TKI. The median follow-up was 16.3 months in the Asciminib group and 15.7 months in the investigator-selected TKI group.
At the 48-week mark, Asciminib demonstrated a significantly higher MMR rate compared to investigator-selected TKIs (67.7% versus 49.0%; P<0.001). Deep molecular response rates (BCR/ABL1 transcript levels 0.01% or less, were also superior in the Asciminib group compared to investigator-selected TKIs (38.8% versus 20.6%). Patients preselected for Imatinib who were randomized to Asciminib achieved an MMR rate of 69.3% compared to 40.2% in the Imatinib group. Among those preselected for second-generation TKIs, the MMR rate was 66.0% for Asciminib versus 57.8% for the second-generation TKI group.
Asciminib exhibited a favorable safety profile with fewer Grade 3 or higher Adverse Events and lower rates of treatment discontinuation due to Adverse Events. Grade 3 or higher Adverse Events for Asciminib was 38%, for Imatinib was 44.4% and for second-generation TKIs was 54.9%. Discontinuation due to Adverse Events for Asciminib was 4.5%, for Imatinib was 11.1% and for Second-generation TKIs was 9.8%.
It was concluded that Asciminib is the only agent to demonstrate superiority over investigator selected standard-of-care TKIs in achieving higher MMR rates at 48 weeks in newly diagnosed chronic phase CML patients, alongside a better safety and tolerability profile. These findings indicate that Asciminib could significantly improve the treatment landscape for this group of patients, offering hope for better disease control and quality of life, thereby addressing key unmet needs in CML management.
ASC4FIRST, a pivotal phase 3 study of asciminib (ASC) vs investigator-selected tyrosine kinase inhibitors (IS TKIs) in newly diagnosed patients (pts) with chronic myeloid leukemia (CML): Primary results. Hughes TP, Hochhaus A, Takahashi N, et al. J Clin Oncol 42, 2024 (suppl 17; abstr LBA6500)
Novel Prognostic Factors for Treatment-Free Remission in Chronic Myeloid leukemia
SUMMARY: Chronic Myeloid Leukemia (CML) constitutes about 15% of all new cases of leukemia. The American Cancer Society estimates that about 9,280 new CML cases will be diagnosed in the United States in 2024 and about 1,280 patients will die of the disease. The hallmark of CML, the Philadelphia Chromosome (Chromosome 22), is a result of a reciprocal translocation between chromosomes 9 and 22, wherein the ABL gene from chromosome 9 fuses with the BCR gene on chromosome 22. As a result, the auto inhibitory function of the ABL gene is lost and the BCR-ABL fusion gene is activated resulting in cell proliferation and leukemic transformation of hematopoietic stem cells.
Chronic Myeloid Leukemia has long been a model for targeted cancer therapy, particularly through the development of Tyrosine Kinase Inhibitors (TKIs) targeting the BCR:ABL1 fusion gene. The presently available Tyrosine Kinase Inhibitors (TKI’s) approved in the United States including Imatinib, share the same therapeutic target, which is BCR-ABL kinase. Resistance to TKI’s can occur as a result of mutations in the BCR-ABL kinase domain or amplification of the BCR-ABL gene. With the availability of newer therapies for CML, monitoring response to treatment is important. This is best accomplished by measuring the amount of residual disease using Reverse Transcription-Polymerase Chain Reaction (RT-PCR). Molecular response in CML is expressed using the International Scale (IS) as BCR-ABL%, which is the ratio between BCR-ABL and a control gene. BCR-ABL kinase domain point mutations are detected using the mutational analysis by Sanger sequencing. Majority of the patients receiving a TKI following diagnosis of CML achieve a Complete Cytogenetic Response (CCyR) within 12 months following commencement of therapy and these patients have a life expectancy similar to that of their healthy counterparts. Previously published studies have shown that Deep Molecular Response (BCR-ABL <0.01% on the International Scale-MR4) is a new molecular predictor of long term survival in CML patients, and this was achieved in a majority of patients treated with TKIs. Further, it has been shown from previous observations, that a subgroup of CML patients experiencing deeper responses (MR3, MR4, and MR4.5), may stay in unmaintained remission even after treatment discontinuation. Despite this observation, precise criteria for stopping CML therapy have not been clearly defined.
Discontinuing TKI therapy after a Deep Molecular Response among patients with CML can potentially improve quality of life, minimize long term toxicities as well as drug-drug interactions, and reduce financial burden. Stopping TKI therapy among CML patients appears to be safe and feasible in over 50% of the patients, although about 20% of these patients experience TKI withdrawal syndrome manifesting as musculoskeletal symptoms. Discontinuation of TKI therapy should only be considered in consenting patients after a thorough discussion of the potential risks and benefits. TKIs have revolutionized the prognosis and quality of life for patients with CML, leading to a new treatment goal of achieving Treatment-Free Remission (TFR).
The European Stop Kinase Inhibitors (EURO-SKI) study is the largest clinical trial conducted to assess the safety of stopping Tyrosine Kinase Inhibitor therapy in patients with CML, whose leukemia was in stable Deep Molecular Response (DMR). The researchers presented the final analysis of the EURO-SKI trial after 3 years of follow up and highlighted the prognostic factors for short- and long-term molecular response maintenance. This comprehensive study evaluated the effects of stopping TKI treatment (Imatinib, Nilotinib or Dasatinib), in patients who had been on therapy for at least 3 years and had confirmed DMR, defined as BCR:ABL1-transcripts 0.01% or less on the International Scale for at least 12 months. The Primary outcomes of the study were the maintenance of Major Molecular Response (MMR), defined as BCR:ABL1 0.1% or less (MR3), at 6 and 36 months after stopping TKIs (Molecular Recurrence Free Survival).
In this study, 868 patients with Chronic Phase CML were screened, and 728 patients were included in the baseline analysis. The final analysis revealed that 61% of patients remained in MMR at 6 months, and 46% remained in MMR at 36 months after stopping TKI treatment. Several factors were identified as significant predictors of MMR maintenance. Longer duration of TKI treatment and DMR before stopping TKI treatment were associated with a higher likelihood of maintaining MMR at 6 months. Additionally, the type of BCR:ABL1 transcript emerged as a prognostic factor, with patients having transcript type e14a2 alone or in combination with e13a2 showing a significantly higher probability of maintaining MMR. For MMR maintenance between 6 and 36 months, the duration of TKI treatment (but not DMR duration) before stopping TKI treatment, and disease characteristics at diagnosis, including percentage of peripheral blood blast cells and platelet count at diagnosis, were significant factors influencing MMR maintenance. Among 315 patients evaluated at 36 months, the Molecular Recurrence Free Survival was 76%. Multivariate analysis over the entire 36-month trial period identified duration of TKI treatment, duration of DMR (Deep Molecular Response) while receiving TKI, percentage of peripheral blood blast cells at diagnosis, and transcript type (e14a2 plus e13a2 had a higher probability of maintaining MMR over 36 months than e13a2 alone) as independent factors for MMR maintenance.
The findings of the EURO-SKI trial have important implications and represent a significant milestone for the management of CML. They highlight the importance of considering not only the duration of TKI treatment but also disease characteristics and transcript type when predicting treatment-free remission. This study represents a significant step forward in understanding the factors influencing Treatment-Free Remission in CML patients, and may help guide clinical decision-making in the future.
European Stop Tyrosine Kinase Inhibitor Trial (EURO-SKI) in Chronic Myeloid Leukemia: Final Analysis and Novel Prognostic Factors for Treatment-Free Remission. Mahon F-X, Pfirrmann M, Dulucq S, et al. on behalf of the EURO-SKI Investigators. Journal of Clinical Oncology. March 12, 2024. https://doi.org/10.1200/JCO.23.01647.
BOSULIF® (Bosutinib)
The FDA on September 26, 2023, approved BOSULIF® for pediatric patients 1 year of age and older with Chronic Phase (CP) Ph+ Chronic Myelogenous Leukemia (CML) that is newly diagnosed or resistant or intolerant to prior therapy. The FDA also approved a new capsule dosage form available in strengths of 50 mg and 100 mg. BOSULIF® is a product of Pfizer.
Low Dose Dasatinib as Frontline Therapy in Newly Diagnosed Chronic Myeloid Leukemia
SUMMARY: Chronic Myeloid Leukemia (CML) constitutes approximately 10% of all new cases of leukemia. The American Cancer Society estimates that 6,660 new CML cases will be diagnosed in the United States in 2015 and about 1,140 people will die of the disease. Chronic Myeloid Leukemia in Chronic Phase (CML-CP) is a clonal myeloproliferative disorder and the hallmark of CML, the Philadelphia Chromosome (Chromosome 22), is a result of a reciprocal translocation between chromosomes 9 and 22, wherein the ABL gene from chromosome 9, fuses with the BCR gene on chromosome 22. As a result, the auto inhibitory function of the ABL gene is lost and the BCR-ABL fusion gene is activated resulting in cell proliferation and leukemic transformation of hematopoietic stem cells. With the development of small molecule tyrosine kinase inhibitors (TKIs) targeting BCR-ABL1, the 10-year survival rate in CML in Chronic phase is 80-90%. There are presently four TKIs (First Generation-Imatinib; Second Generation- Nilotinib, Dasatinib and Bosutinib) approved by the FDA for frontline therapy of patients with newly diagnosed CML-CP. Treatment with second generation TKIs has demonstrated significantly deeper and faster cytogenetic and Major MolecularResponses, but without any impact on long-term survival.
Dasatinib (SPRYCEL®) is an oral second generation TKI and is 325 times more potent than imatinib in inhibiting unmutated BCR-ABL1 kinase in vitro. It additionally inhibits the Src family of kinases, which are key regulators of signal transduction. Dasatinib 100mg once daily was approved by the FDA in 2010 for the treatment of patients with newly diagnosed Philadelphia chromosome-positive (Ph+) chronic myeloid leukemia (CML) in chronic phase, based on the Pivotal DASISION Study. In this trial, Dasatinib demonstrated Superior Efficacy with Higher and Faster Molecular and Confirmed Complete Cytogenetic Response Rates, compared to Imatinib by 12 months. In this trial drug-related pleural effusions occurred more frequently with Dasatinib than with Imatinib (28% versus <1%), as well as myelosuppression (20%), and, occasionally, pulmonary hypertension (5%).
Dasatinib in early clinical trials demonstrated activity at lower doses with better safety profile. Further in the DASISION trial, the efficacy of Dasatinib was maintained among patients who had their dose reduced, while improving its safety profile. Low-dose Dasatinib appears to be safe and effective in patients with Chronic Myeloid Leukemia in Chronic Phase (CML-CP). However there are no randomized trials comparing the outcome with standard-dose Dasatinib.
This present study was conducted to compare the outcome of patients with newly diagnosed CML-CP treated with Dasatinib 50 versus 100 mg/day. The researchers analyzed 233 patients with newly diagnosed CML-CP treated with low-dose Dasatinib (N = 83) or standard-dose Dasatinib (N = 150). Using Propensity score analysis with 1:1 matching, 77 patients in each cohort were identified without significant baseline differences.
Response rates were reported as the cumulative incidences of Complete Cytogenetic Response (CCyR), Major Molecular Response (MMR), Molecular Response with 4.0 (MR4.0) and 4.5 (MR4.5) log reduction. MMR was defined as BCR-ABL1/ABL1 (IS) ≤0.1%, MR4.0 defined as BCR-ABL1/ABL1 (IS) ≤0.01% and MR4.5 defined as BCR-ABL1/ABL1 (IS) ≤0.0032%. Additional comparisons between the two groups included Overall Survival (OS) calculated from the start date of the therapy to the date of death from any cause at any time or date of last follow-up, Event-Free Survival (EFS) to the date of any of the events while on study as defined in the IRIS study, Failure-Free Survival (FFS) was calculated from the start date of therapy to the dates of treatment discontinuation for any reason except of treatment-free remission, Transformation-Free Survival (TFS), to the date of transformation to accelerated or blast phases during study. Patients on low-dose Dasatinib with suboptimal response by European LeukemiaNet (ELN) 2013 criteria had the option to increase the dose to 100 mg/day. The median age was 47 years. By Sokal risk score, 66% patients had low-risk, 25% had intermediate-risk, and 9% had high-risk disease. The median follow-up time was 60 months.
The 3-year MMR rates were 92% and 84% for low-dose and standard-dose Dasatinib, respectively (P=0.23). Dasatinib 50 mg/day induced higher cumulative incidence of MR4.0 (77% versus 66%; P=0.04) and MR4.5 (77% vs. 62%; P=0.02) at 3 years. The 4-year FFS, EFS and OS rates were 89% versus 77% (P=0.04), 95% versus 92% (P=0.06), and 97% versus 96% (P=0.78) with low-dose and standard-dose Dasatinib, respectively. The incidence of any grade pleural effusion was 5% with Dasatinib 50 mg/day compared to 21% with Dasatinib 100 mg/day.
It was concluded that Dasatinib 50mg daily is a new, cost-effective therapeutic option for frontline therapy in CML-CP and is at least as effective as Dasatinib 100 mg/day, with a better safety profile.
Low-dose dasatinib 50 mg/day versus standard-dose dasatinib 100 mg/day as frontline therapy in chronic myeloid leukemia in chronic phase: A propensity score analysis. Jabbour E, Sasaki K, Haddad FG, et al. Am J Hematol. 2022;97:1413-1418.
SCEMBLIX® (Asciminib)
The FDA on October 29, 2021, granted accelerated approval to SCEMBLIX® (Asciminib) for patients with Philadelphia chromosome-positive Chronic Myeloid Leukemia (Ph+ CML) in Chronic Phase (CP), previously treated with two or more Tyrosine Kinase Inhibitors (TKIs), and approved SCEMBLIX® for adult patients with Ph+ CML in CP with the T315I mutation. SCEMBLIX® is a product of Novartis AG.
FDA Approves SCEMBLIX® for Chronic Myeloid Leukemia
SUMMARY: The FDA on October 29, 2021, granted accelerated approval to SCEMBLIX® (Asciminib), for patients with Philadelphia chromosome-positive Chronic Myeloid Leukemia (Ph-positive CML) in Chronic Phase, previously treated with two or more Tyrosine Kinase Inhibitors (TKIs), and approved SCEMBLIX® for adult patients with Ph-positive CML in Chronic Phase with the T315I mutation.
The American Cancer Society estimates that about 9,110 new CML cases will be diagnosed in the United States in 2021 and about 1,220 patients will die of the disease. Chronic Myeloid Leukemia (CML) constitutes about 15% of all new cases of leukemia and the average age at diagnosis of CML is around 64 years. The hallmark of CML, the Philadelphia Chromosome (Chromosome 22), is a result of a reciprocal translocation between chromosomes 9 and 22, wherein the ABL gene from chromosome 9 fuses with the BCR gene on chromosome 22. As a result, the auto inhibitory function of the ABL gene is lost and the BCR-ABL fusion gene is activated resulting in cell proliferation and leukemic transformation of hematopoietic stem cells.
The presently available Tyrosine Kinase Inhibitors (TKI’s) approved in the United States share the same therapeutic target, which is the ATP-binding site of BCR-ABL1 kinase. Close to 50% of clinical resistance is associated with the acquisition of mutations in this region of the kinase, resulting in conformational changes that render TKIs inactive. Therefore resistance to one of the TKIs, will likely result in resistance to the others as well. Further, the “gatekeeper” T315I mutation, which has been reported in 20% of patients with mutations, confers resistance to all clinically available TKIs except ICLUSIG® (Ponatinib).
SCEMBLIX® is a novel, first-in-class, potent and specific, oral BCR-ABL1 inhibitor that does not bind to the ATP-binding site of the kinase. Instead, it specifically targets the ABL1 myristoyl pocket, also known as a STAMP (Specifically Targeting the ABL Myristoyl Pocket) inhibitor, with activity against native unmutated BCR-ABL1, and all clinically observed ATP-site mutants, including T315I. In a Phase I study, SCEMBLIX® was active in heavily pretreated patients with CML who had resistance to or unacceptable side effects from TKIs, including patients in whom ICLUSIG® had failed, and those with a T315I mutation.
The present FDA approval was based on data from the Phase III ASCEMBL trial which evaluated this agent in patients with Ph-positive CML who previously received 2 or more TKIs, and the Phase I CABL001X2101 trial, which evaluated its use in patients with Ph-positive CML in Chronic Phase harboring a T315I mutation.
ASCEMBL is a multicenter, randomized, active-controlled, open-label, Phase III trial, which evaluated SCEMBLIX® in patients with Ph-positive CML in Chronic Phase, previously treated with two or more TKIs. In this study, a total of 233 patients were randomized (2:1) to receive either SCEMBLIX® 40 mg twice daily (N=157) or BOSULIF® (Bosutinib) 500 mg once daily (N=76). Patients were stratified by Major Cytogenetic Response (MCyR; Ph-positive metaphases 35% or less at baseline). Patients intolerant of their most recent TKI were eligible if they had BCR-ABL1 International Scale more than 0.1% at screening. Treatment was continued until unacceptable toxicity or treatment failure occurred. The median patient age was 52 years and 48% of patients had received 2 prior lines of treatment, 31% received 3 prior lines of therapy. The Primary endpoint was Major Molecular Response (MMR) rate at 24 wks.
In this study, the MMR rate was 25.5% in patients treated with SCEMBLIX® compared with 13.2% in those receiving BOSULIF®, meeting the primary objective of this study (P=0.029). At a median follow up of 20 months, the median duration of MMR has not yet been reached. Among those pts who achieved MMR, the median time to MMR was 12.7 weeks among those who achieved MMR with SCEMBLIX®, and 14.3 weeks with BOSULIF®. At 24 wks, more patients on SCEMBLIX® (19.7%)] achieved Deep Molecular Response (MR4 and MR4.5), compared with 6.6% with BOSULIF®. The Complete Cytogenetic Response rate at 24 weeks was 40.8% with SCEMBLIX® compared with 24.2% for BOSULIF®. Additionally, preplanned subgroup analysis showed that the MMR rate at 24 weeks was superior with SCEMBLIX® compared to BOSULIF® across most major demographic and prognostic subgroups, including among patients who received 3 or more prior TKIs, in those who discontinued the prior TKI due to treatment failure, and regardless of baseline Cytogenetic Response.
CABL001X2101 is a multicenter, open-label clinical trial, in which the efficacy of SCEMBLIX® was evaluated in patients with Ph-positive CML in Chronic Phase, with the T315I mutation. In this study, 45 patients with the T315I mutation received SCEMBLIX® 200 mg twice daily and treatment was continued until unacceptable toxicity or treatment failure. The main efficacy outcome measure was MMR.
MMR was achieved by 24 weeks in 42% of the patients, and 49% of the patients achieved MMR by 96 weeks. The median duration of treatment was 108 weeks.
The most common adverse reactions included upper respiratory tract infections, musculoskeletal pain, fatigue, nausea, rash, diarrhea, and cytopenias. Patients also were noted to have increased triglycerides, increased creatine kinase, alanine aminotransferase, lipase, and amylase.
It can be concluded from these two studies that SCEMBLIX®, a first-in-class STAMP inhibitor, demonstrated statistically significant and clinically meaningful superiority in efficacy, compared with BOSULIF®, among patients with Chronic Phase CML previously treated with two or more TKIs. SCEMBLIX® is also a new treatment option for patients with Ph-positive CML in Chronic Phase, harboring a T315I mutation.
A Phase 3, Open-Label, Randomized Study of Asciminib, a STAMP Inhibitor, vs Bosutinib in CML After ≥2 Prior TKIs. Rea D, Mauro MJ, Boquimpani C, et al. Blood. 2021 Aug 18;blood.2020009984. doi: 10.1182/blood.2020009984. Online ahead of print.
NCCN Establishes TKI Discontinuation Criteria in Updated CML Guideline
SUMMARY: Chronic Myeloid Leukemia (CML) constitutes about 15% of all new cases of leukemia. The American Cancer Society estimates that about 8,990 new CML cases will be diagnosed in the United States in 2019 and about 1,140 patients will die of the disease. The hallmark of CML, the Philadelphia Chromosome (Chromosome 22), is a result of a reciprocal translocation between chromosomes 9 and 22, wherein the ABL gene from chromosome 9 fuses with the BCR gene on chromosome 22. As a result, the auto inhibitory function of the ABL gene is lost and the BCR-ABL fusion gene is activated resulting in cell proliferation and leukemic transformation of hematopoietic stem cells.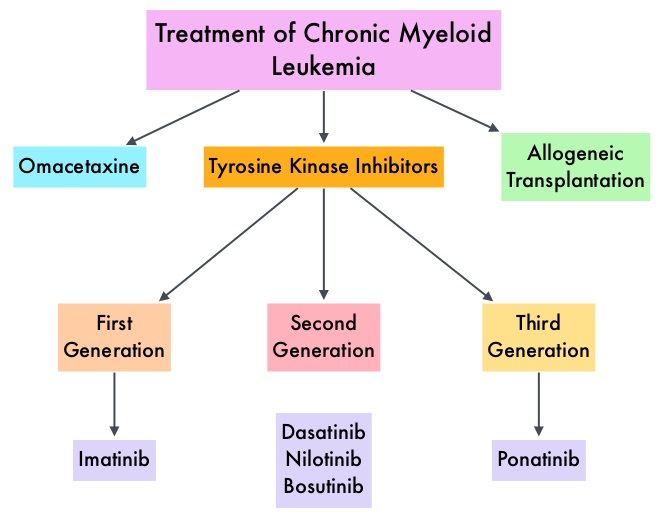
The presently available Tyrosine Kinase Inhibitors (TKI’s) approved in the United States including GLEEVEC® (Imatinib), share the same therapeutic target, which is BCR-ABL kinase. Resistance to TKI’s can occur as a result of mutations in the BCR-ABL kinase domain or amplification of the BCR-ABL gene. With the availability of newer therapies for CML, monitoring response to treatment is important. This is best accomplished by measuring the amount of residual disease using Reverse Transcription-Polymerase Chain Reaction (RT-PCR). Molecular response in CML is expressed using the International Scale (IS) as BCR-ABL%, which is the ratio between BCR-ABL and a control gene. BCR-ABL kinase domain point mutations are detected using the mutational analysis by Sanger sequencing. Majority of the patients receiving a TKI following diagnosis of CML achieve a Complete Cytogenetic Response (CCyR) within 12 months following commencement of therapy and these patients have a life expectancy similar to that of their healthy counterparts. Previously published studies have shown that Deep Molecular Response (BCR-ABL <0.01% on the International Scale – MR4) is a new molecular predictor of long term survival in CML patients, and this was achieved in a majority of patients treated with optimized dose of GLEEVEC®. Further, it has been shown on previous observations, that a subgroup of CML patients experiencing deeper responses (MR3, MR4, and MR4.5), may stay in unmaintained remission even after treatment discontinuation. Despite this observation, precise criteria for stopping CML therapy have not been clearly defined.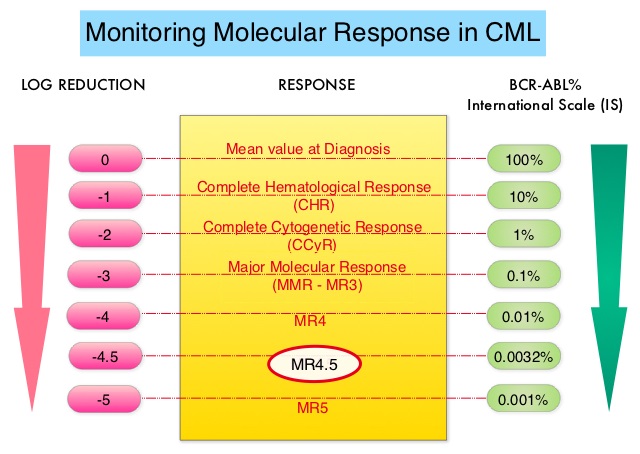
Discontinuing TKI therapy after a Deep Molecular Response among patients with CML can potentially improve quality of life, minimize long term toxicities as well as drug-drug interactions, and reduce financial burden. Two important studies, STIM (Stop Imatinib) and EURO-SKI have set the stage for TKI discontinuation of TKI therapy in CML patients, who are in deep molecular remission, taking into consideration Sokal score at diagnosis, duration on TKI therapy and molecular response based on BCR-ABL transcripts log reduction. Sokal score is calculated using a formula that includes Age, Spleen size, Platelet count and percentage of Myeloblasts and has three risk groups: Low-risk (Sokal score<0.8), Intermediate-risk (Sokal score 0.8-1.2) and High-risk (Sokal score >1.2).
Stopping TKI therapy among CML patients appears to be safe and feasible in over 50% of the patients, although about 20% of these patients experience TKI withdrawal syndrome manifesting as musculoskeletal symptoms. Discontinuation of TKI therapy should only be considered in consenting patients after a thorough discussion of the potential risks and benefits.
Criteria for TKI Discontinuation: Outside of a clinical trial, TKI discontinuation should be considered only if a patient meets ALL the criteria listed below-
1) Age 18 years or older.
2) Chronic phase CML with no prior history of Accelerated or Blast phase.
3) On approved TKI therapy for at least 3 years.
4) Prior evidence of quantifiable BCR-ABL1 transcript.
5) Stable molecular response defined as MR4, (BCR-ABL equal to 0.01% or less IS), for 2 or more years as documented on at least 4 tests, performed at least 3 months apart.
6) Access to qPCR test that can reliably detect at least MR4.5 (BCR-ABL equal to 0.0032% or less IS), with results available within 2 weeks.
7) For patients who remain in Major Molecular Remission or MMR (MR3, BCR-ABL equal to 0.1% or less IS) after discontinuation of TKI therapy, the recommendations are monthly molecular monitoring the first year, every 6 weeks the second year and every 12 weeks thereafter, indefinitely.
8) TKI therapy should be promptly resumed within 4 weeks of a loss of MMR, with molecular monitoring every 4 weeks until MMR is re-established and then every 12 weeks thereafter, indefinitely. If a patient fails to achieve MMR after 3 months of TKI resumption, BCR-ABL kinase domain mutation testing should be performed, and monthly molecular monitoring should be continued for an additional 6 months.
9) Consultation with a CML Specialty Center is recommended regarding the appropriateness for TKI discontinuation, and potential risks and benefits of discontinuing therapy, including TKI withdrawal syndrome.
10) It is strongly encouraged to report the following to an NCCN CML Panel Member-
a) Any significant adverse event thought to be related to therapy discontinuation.
b) Progression to Accelerated or Blast phase at any time.
c) Failure to regain MMR after 3 months following treatment reinitiation.
NCCN guidelines updates: discontinuing TKI therapy in the treatment of chronic myeloid leukemia. Shah NP. Presented at 2019 NCCN Annual Conference; March 21-23, 2019; Orlando, FL.
TASIGNA® (Nilotinib)
The FDA on March 22, 2018 approved TASIGNA® for pediatric patients 1 year of age or older with newly diagnosed Philadelphia chromosome positive Chronic Myeloid Leukemia in Chronic Phase (Ph+ CML-CP) or Ph+ CML-CP resistant or intolerant to prior Tyrosine Kinase Inhibitor (TKI) therapy. TASIGNA® is a product of Novartis Pharmaceuticals Corporation.