
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (13%) will develop invasive breast cancer during their lifetime. Approximately 276,480 new cases of invasive female breast cancer will be diagnosed in 2020 and about 42,170 women will die of the disease.
Triple Negative Breast Cancer (TNBC) is a heterogeneous, molecularly diverse group of breast cancers and are ER (Estrogen Receptor), PR (Progesterone Receptor) and HER2 (Human Epidermal Growth Factor Receptor-2) negative. TNBC accounts for 15-20% of invasive breast cancers, with a higher incidence noted in young patients. It is usually aggressive, and tumors tend to be high grade and patients with TNBC are at a higher risk of both local and distant recurrence. Those with metastatic disease have one of the worst prognoses of all cancers with a median Overall Survival of 13 months. The majority of patients with TNBC who develop metastatic disease do so within the first 3 years after diagnosis, whereas those without recurrence during this period of time have survival rates similar to those with ER-positive breast cancers. The lack of known recurrent oncogenic drivers in patients with metastatic TNBC, presents a major therapeutic challenge. Nonetheless, patients with TNBC often receive chemotherapy in the neoadjuvant, adjuvant or metastatic settings and approximately 30-40% of patients achieve a pathological Complete Response (pCR) in the neoadjuvant setting. In addition to increasing the likelihood of tumor resectability and breast preservation, patients achieving a pCR following neoadjuvant chemotherapy have a longer Event Free Survival (EFS) and Overall Survival (OS). Those who do not achieve a pathological Complete Response tend to have a poor prognosis. For all these reasons, pCR is considered a valid endpoint for clinical testing of neoadjuvant therapy in patients with early stage TNBC. It appears that there are subsets of patients with TNBC who may be inherently insensitive to cytotoxic chemotherapy. Three treatment approaches appear to be promising and they include immune therapies, PARP inhibition and inhibition of PI3K pathway. Previously published studies have shown that presence of tumor-infiltrating lymphocytes was associated with clinical benefit, when treated with chemotherapy and immunotherapy, in patients with TNBC, and improved clinical benefit was observed in patients with immune-enriched molecular subtypes of metastatic TNBC.
KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2. It thereby reverses the PD-1 pathway-mediated inhibition of the immune response and unleashes the tumor-specific effector T cells. Cytotoxic chemotherapy releases tumor-specific antigens and immune checkpoint inhibitors such as KEYTRUDA® when given along with chemotherapy can enhance endogenous anticancer immunity. Preliminary results from Phase I and II trials have shown that in patients with TNBC, KEYTRUDA® given along with chemotherapy in a neoadjuvant setting resulted in a high rate of pCR.
KEYNOTE-522 is an international, placebo controlled Phase III trial, conducted to evaluate the safety and efficacy of neoadjuvant KEYTRUDA® plus chemotherapy followed by adjuvant KEYTRUDA® or placebo, in patients with early stage TNBC. In this study, 1,174 patients were randomly assigned in a 2:1 ratio to receive neoadjuvant KEYTRUDA® 200 mg IV every 3 weeks (N=784) or placebo (N=390). All patients received 4 cycles of Carboplatin plus Paclitaxel, followed by 4 cycles of Doxorubicin or Epirubicin plus Cyclophosphamide, in the neoadjuvant setting. Following definitive surgery, adjuvant KEYTRUDA® or placebo was continued every 3 weeks for 9 cycles or until disease recurrence or unacceptable toxicity. Enrolled TNBC patients were newly diagnosed, treatment naïve, and included both node-negative and node-positive patients with nonmetastatic disease (Tumor Stage T1c, Nodal Stage N1-N2 or Tumor Stage T2-T4, Nodal Stage N0-N2, per AJCC criteria). Treatment groups were well balanced and patients were stratified according to nodal status, tumor size, and Carboplatin schedule (weekly versus every 3 weeks). The two Primary endpoints were pathological Complete Response (pCR) at the time of definitive surgery and Event Free Survival (EFS). The median follow up was 15.5 months.
At the first interim analysis, the pCR among the first 602 patients who underwent randomization was 64.8% in the KEYTRUDA® plus chemotherapy group, compared with 51.2% in the placebo plus chemotherapy group (P<0.001). This pCR benefit was consistent across subgroups including PD-L1 expresssion subgroups. In the PD-L1-positive population, the pCR was 68.9% in the KEYTRUDA® plus chemotherapy group compared with 54.9% in the placebo plus chemotherapy group. In the PD-L1 negative group, the pCR in the KEYTRUDA® plus chemotherapy group was 45.3% and 30.3% in the placebo plus chemotherapy group. Neoadjuvant KEYTRUDA® plus chemotherapy followed by adjuvant KEYTRUDA® showed a favorable trend for Event Free Survival compared with chemotherapy alone, although these data are still premature. Across all treatment phases, Grade 3 or higher treatment-related toxicities were 78.0% in the KEYTRUDA® plus chemotherapy group and 73.0% in the placebo plus chemotherapy group.
It was concluded that among patients with early stage Triple Negative Breast Cancer, the addition of KEYTRUDA® to neoadjuvant chemotherapy significantly increased the pathological Complete Response rate, compared to those who received placebo plus neoadjuvant chemotherapy, with a favorable trend in Event Free Survival. Pembrolizumab for Early Triple-Negative Breast Cancer. Schmid P, Cortés J, Pusztai L, et al. for the KEYNOTE-522 Investigators. N Engl J Med 2020;382:810-821
Tag: Breast Cancer
KISQALI® plus FASLODEX® Improve Overall Survival in Advanced Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease. Approximately 70% of breast tumors express Estrogen Receptors and/or Progesterone Receptors. The most common subtype of metastatic breast cancer is Hormone Receptor-positive (HR-positive), HER2-negative breast cancer (65% of all metastatic breast tumors), and these patients are often treated with anti-estrogen therapy as first line treatment. However, resistance to hormonal therapy occurs in a majority of the patients, with a median Overall Survival (OS) of 36 months. Cyclin Dependent Kinases (CDK) play a very important role to facilitate orderly and controlled progression of the cell cycle. Genetic alterations in these kinases and their regulatory proteins have been implicated in various malignancies.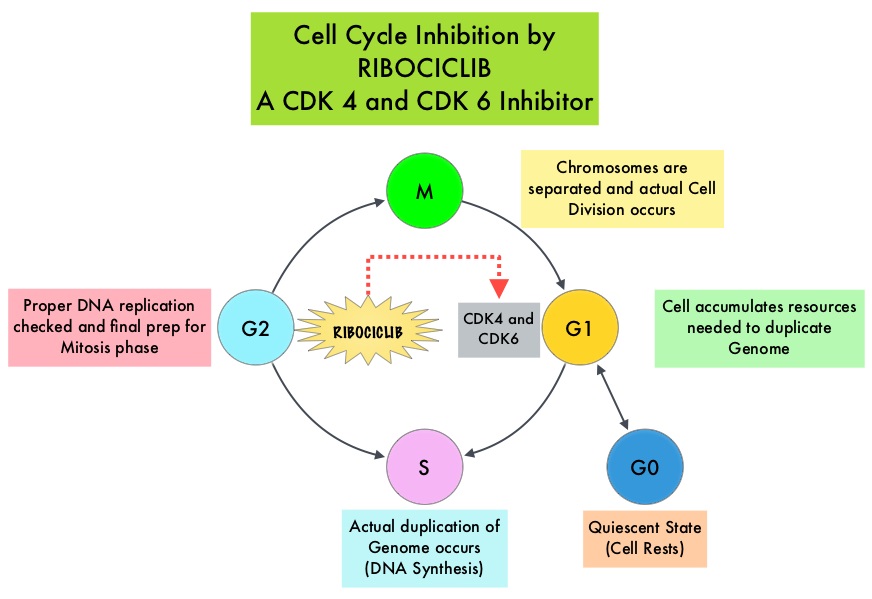
Cyclin Dependent Kinases 4 and 6 (CDK4 and CDK6) phosphorylate RetinoBlastoma protein (RB), and initiate transition from the G1 phase to the S phase of the cell cycle. RetinoBlastoma protein has antiproliferative and tumor-suppressor activity and phosphorylation of RB protein nullifies its beneficial activities. CDK4 and CDK6 are activated in hormone receptor positive breast cancer, promoting breast cancer cell proliferation. Further, there is evidence to suggest that endocrine resistant breast cancer cell lines depend on CDK4 for cell proliferation. The understanding of the role of Cyclin Dependent Kinases in the cell cycle, has paved the way for the development of CDK inhibitors.
KISQALI® (Ribociclib) is an orally bioavailable, selective, small-molecule inhibitor of CDK4/6, that blocks the phosphorylation of RetinoBlastoma protein, thereby preventing cell-cycle progression and inducing G1 phase arrest. KISQALI® in combination with an Aromatase Inhibitor has been approved by the FDA for pre and perimenopausal women with HR (Hormone Receptor)-positive, HER2-negative advanced or metastatic breast cancer, as initial endocrine-based therapy. The efficacy of KISQALI® was evaluated in two prior randomized Phase III studies. In the MONALEESA-2 trial which evaluated KISQALI® in combination with FEMARA® (Letrozole) compared to FEMARA® alone, in postmenopausal women with HR-positive, HER2-negative advanced breast cancer, who received no prior therapy for their advanced breast cancer, the addition of KISQALI® to FEMARA® significantly prolonged Progression Free Survival (PFS) compared to FEMARA® alone. In the MONALEESA-7 study, KISQALI® in combination with Tamoxifen or a Non-Steroidal Aromatase Inhibitor plus ZOLADEX® (Goserelin) was compared with Tamoxifen or an Aromatase Inhibitor plus ZOLADEX®, in premenopausal or perimenopausal women with HR-positive, HER2- negative advanced breast cancer, who had not previously received endocrine therapy for advanced disease. In this study of premenopausal women, KISQALI® plus endocrine therapy significantly improved PFS and OS, compared with placebo plus endocrine therapy.
MONALEESA-3 is a randomized, double-blind, placebo-controlled Phase III study which compared the efficacy of KISQALI® in combination with FASLODEX® with FASLODEX® alone, among postmenopausal women with HR-positive, HER2-negative advanced breast cancer, who received no prior or only one line of prior endocrine therapy for advanced disease. In this trial, 726 women were randomized, of whom 367 were treatment-naïve and 345 patients had received up to one line of prior endocrine therapy for advanced disease. . Patients were randomized 2:1 to receive KISQALI® plus FASLODEX® (N=484) or placebo plus FASLODEX® (N=242). Treatment consisted of KISQALI® 600 mg orally daily 3 weeks on and 1 week off and FASLODEX® 500 mg IM on day 1 of each 28-day cycle, with an additional dose given on day 15 of cycle 1. Patients were stratified by the presence or absence of lung or liver metastases and prior endocrine therapy (first-line versus second-line). The median age in both groups was 63 years. The Primary endpoint was Progression Free Survival (PFS). Secondary end points included Overall Survival (OS), Overall Response Rate (ORR), and Safety.
In the primary analysis of the trial, the median PFS in the KISQALI® plus FASLODEX® group was 20.5 months compared to 12.8 months in the FASLODEX® plus placebo group (HR= 0.59; P<0.001). This represented a 41% reduction in the risk of disease progression. The authors now report the results of the second interim analysis of Overall Survival and an updated analysis of Progression Free Survival. The median duration of follow up for all patients was 39.4 months, and the median duration of treatment was 15.8 months in the KISQALI® group and 12.0 months in the placebo group.
There was a significant Overall Survival benefit with KISQALI® plus FASLODEX® compared to placebo plus FASLODEX®. The estimated Overall Survival at 42 months was 57.8% in the KISQALI® group compared to 45.9% in the placebo group, and this represented a 28% reduction in the relative risk of death with the KISQALI® combination (HR=0.72; P=0.00455). The survival benefit was consistent across most subgroups. The median PFS among patients receiving first line treatment was 33.6 months (95% CI, 27.1 to 41.3) in the KISQALI® group and 19.2 months in the placebo group. No new safety signals were observed during this longer follow up period.
It was concluded that KISQALI® plus FASLODEX® significantly improved Overall Survival compared to placebo plus FASLODEX® in patients with HR-positive, HER2-negative advanced breast cancer, regardless of whether they received their treatment in the frontline setting or subsequently. Overall Survival with Ribociclib plus Fulvestrant in Advanced Breast Cancer. Slamon DJ, Neven P, Chia S, et al. N Engl J Med 2020;382:514-524
Assessment of Molecular Relapse Detection in Early Stage Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease. Majority of the breast cancer patients present with early stage disease without macroscopic metastatic disease. Several small proof of principle studies have shown that detection of circulating tumor DNA (ctDNA) in the peripheral blood may identify patients at risk of relapse following definitive therapy. ctDNA refers to DNA fragments that are shed into the bloodstream by cancer cells after apoptosis or necrosis. ctDNA can detect almost all molecular alterations present in cancer cells and the proportion of ctDNA that originates from a tumor depends on the anatomic location, tumor burden and cell turnover. ctDNA allows real-time monitoring for treatment response and resistance.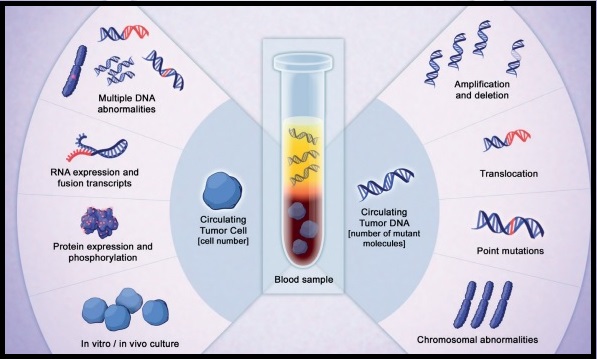
To assess the clinical validity of molecular relapse detection with circulating tumor DNA (ctDNA) analysis in early-stage breast cancer, the authors conducted a multicenter, prospective study in the UK over a 5 year period, and included patients, irrespective of their hormone receptor or HER2 status, who were receiving neoadjuvant chemotherapy followed by surgery or surgery before adjuvant chemotherapy. All patients had primary breast cancer without evidence of distant metastatic disease and patients scheduled to receive standard neoadjuvant chemotherapy followed by surgery consented for plasma sample collection before chemotherapy, and patients scheduled to receive adjuvant chemotherapy consented for plasma sample collection after surgery and before chemotherapy. This study enrolled 170 women, and somatic mutations were identified in 101 patients, and this formed the primary analysis cohort and secondary analyses were conducted on a combined cohort of 144 patients, including 43 patients previously analyzed in a proof of principle study (N=101+43). Tumor DNA extracted from the primary tumor was sequenced to identify somatic mutations to track in plasma, and personalized tumor-specific digital Polymerase Chain Reaction (dPCR) assays were designed to monitor these somatic mutations in serial plasma samples collected from patients every 3 months during the first year of follow up, and subsequently every 6 months for 5 years. ctDNA testing can identify genetic alterations unrelated to the lesion of interest (Clonal Hematopoiesis of Indeterminate Potential- CHIP). The authors analyzed buffy coat DNA to control for CHIP, which is common with increasing age and can potentially cause false-positive results in ctDNA analysis. The mean patient age was 54 years and the median follow up was 35.5 months. The Primary objective of the study was to assess whether patients with ctDNA detected in follow-up blood samples had worse Relapse Free Survival than patients without detectable ctDNA. Secondary end points included lead time between ctDNA detection and relapse, and association between detection of ctDNA in the diagnosis sample before neoadjuvant chemotherapy and relapse.
Results from the combined cohort of 144 patients showed that detection of ctDNA during follow up was associated with relapse (88.4% of patients who experienced relapse had antecedent ctDNA detection- P<0.001). Detection of ctDNA at diagnosis, before any treatment, was associated with larger tumor size and higher tumor grade, and patients with Triple Negative Breast Cancer (TNBC) had the highest level of ctDNA, likely due to high proliferative rates and cell turnover. This patient group was at a higher risk to relapse. Further, ctDNA detection had a median lead time of 10.7 months before clinical relapse and was associated with relapse in all breast cancer subtypes. Distant extracranial metastatic relapse was detected by ctDNA in 96% of patients. Brain-only metastasis however was less commonly detected by ctDNA, suggesting that cranial metastases are less readily detectable by ctDNA analysis.
It was concluded that detection of ctDNA during follow up of early-stage breast cancer is associated with a high risk of future relapse. A clinical trial is underway evaluating the benefit of treatment initiation at molecular relapse, before clinical development of metastatic disease. Assessment of Molecular Relapse Detection in Early-Stage Breast Cancer. Garcia-Murillas I, Chopra N, Comino-Méndez I, et al. JAMA Oncol.2019;5:1473-1478.
Multigene Testing for All Patients with Breast Cancer Could Identify Many More Mutation Carriers
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease. DNA can be damaged due to errors during its replication or as a result of environmental exposure to ultraviolet radiation from the sun or other toxins. The tumor suppressor genes such as BRCA1 (Breast Cancer 1) and BRCA2 help repair damaged DNA and thus play an important role in maintaining cellular genetic integrity, failing which these genetic aberrations can result in malignancies. The BRCA1 gene is located on the long (q) arm of chromosome 17 whereas BRCA2 is located on the long arm of chromosome 13. These mutations can be inherited from either of the parents in an Autosomal Dominant pattern and a child has a 50% chance of inheriting this mutation, and the deleterious effects of the mutations are seen even when an individual’s second copy of the gene is normal.
It is estimated that BRCA1/2 gene mutations occur in approximately 1 in 400 women in the general population and account for 20-25% of hereditary breast cancers, about 5-10% of all breast cancers and 15% of ovarian cancers. Mutations in the BRCA1/2 genes increase breast cancer risk 45-65% by age 70 years. The risk of ovarian, fallopian tube, or peritoneal cancer, increases to 39% for BRCA1 mutations, and 10-17% for BRCA2 mutations. PALB2 (Partner And Localizer of BRCA2) gene provides instructions to make a protein that works along with the BRCA2 protein, to repair damaged DNA. PALB2 mutation is rare in sporadic breast cancer, and is considered a high-penetrance breast cancer predisposing gene associated with 14% risk of developing breast cancer by age 50 and a 35% risk of developing breast cancer by age 70. Women with a PALB2 mutation face an increased risk of triple negative breast cancer and higher risk of death from breast cancer. PALB2 gene mutations have also been implicated in ovarian, pancreatic and other malignancies.
Current guidelines recommend genetic testing in women with breast cancer who fulfill recognized or established family history or clinical criteria. However, patients with breast cancer and genetic pathogenic variants do not always have a positive family history, and these criteria miss approximately 50% of pathogenic variant carriers. Further, genetic testing based on family history or clinical criteria depends on the awareness and understanding both by the health care providers and patients, and appropriate referrals to genetic counselors. Because of limited awareness and restricted access to genetic testing and counseling services, only 20-30% of eligible patients undergo genetic testing, and 97% of estimated carriers in the general population remain unidentified, thereby missing substantial opportunities for primary prevention.
Knowledge of a patient’s genetic pathogenic variant status has important therapeutic and prognostic implications. Identifying unaffected relatives carrying pathogenic variants enables early diagnosis and cancer prevention by offering risk management options such as enhanced MRI imaging and mammography screening, risk-reducing surgeries such as prophylactic mastectomy, salpingo-oopherectomy and chemoprevention with Selective Estrogen Receptor Modulators.
The authors in this study estimated the downstream health effects, costs and cost-effectiveness of multigene testing for all patients with breast cancer, compared with current practice of BRCA testing based on clinical criteria or family history alone. In this modeling study, data was incorporated from four large breast cancer clinical trials and/or research cohorts in the United States, United Kingdom, and Australia. This analysis included 11,836 women with invasive breast cancer, regardless of the family history, and compared lifetime costs and effects of high-risk BRCA1/BRCA2/PALB2 (multigene) testing of all unselected patients with breast cancer (Strategy A) with BRCA1/BRCA2 testing based on family history or clinical criteria (Strategy B), in UK and US populations, from January 1, 2018, through June 8, 2019.
Affected patients with BRCA/PALB2 mutations could undertake contralateral preventive mastectomy and BRCA carriers could choose Risk-Reducing Salpingo-Oophorectomy (RRSO). If patients had a BRCA1/BRCA2/PALB2 pathogenic variant, their first-degree relatives undergo testing for the familial pathogenic variant. If the first-degree relative had a BRCA1/BRCA2/PALB2 pathogenic variant, second-degree relatives undergo testing. Unaffected relative carriers could undergo MRI or mammography screening, chemoprevention, or risk-reducing mastectomy for breast cancer risk and RRSO for ovarian cancer risk. This analysis incorporated lifetime risks and long-term consequences to provide a lifetime horizon. Incidence of ovarian cancer, breast cancer, excess deaths due to heart disease, and the overall population effects were estimated.
Multigene testing was restricted to BRCA1/BRCA2/PALB2, to comply with the ACCE framework for genetic testing, which was advocated for clinical applicability of genetic testing. The ACCE framework includes Analytic validity which is technical test performance, Clinical validity which is the ability of a genetic test to identify or predict accurately and reliably the clinically defined disorder or phenotype of interest, Clinical utility which is evidence that a genetic test improves clinical outcomes measurably and that it adds value for patient management decision making compared with current management without genetic testing, and ELSI which are the complex Ethical, Legal, and Social Implications associated with genetic tests.
This study showed that unselected BRCA1/BRCA2/PALB2 testing for all patients at breast cancer diagnosis was extremely cost-effective compared with BRCA1/BRCA2 testing based on clinical criteria or family history for both UK and US health systems, with incremental cost-effectiveness ratios of £10,464 or £7,216 and $65,661 or $61,618 per Quality-Adjusted Life-Year, respectively. Quality-Adjusted Life-Year (QALY) is a measurement of health outcomes in economic evaluations recommended by NICE (National Institute of Health and Clinical Excellence). This is well below UK and US cost-effectiveness thresholds. The authors estimated that one year’s unselected panel genetic testing could prevent 1142 cases of breast cancer, 959 cases of ovarian cancer, and 633 deaths related to breast or ovarian cancer in the UK. In the US, one year’s unselected panel genetic testing could prevent 5478 cases of breast cancer, 4255 cases of ovarian cancer, and 2406 deaths related to breast or ovarian cancer.
It was concluded from this analysis that unselected, high-risk multigene testing for all women with breast cancer is extremely cost-effective, compared with testing based on family history or clinical criteria, and could identify many more mutation carriers who can benefit from precision prevention. The authors added that these findings support changing current policy to expand genetic testing to all women with breast cancer. A Cost-effectiveness Analysis of Multigene Testing for All Patients with Breast Cancer. Sun L, Brentnall A, Patel S, et al. JAMA Oncol. 2019;5:1718-1730
Neoadjuvant KEYTRUDA® Plus Chemotherapy Improves Pathological Complete Response in Triple Negative Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (13%) will develop invasive breast cancer during their lifetime. Approximately 276,480 new cases of invasive female breast cancer will be diagnosed in 2020 and about 42,170 women will die of the disease.
Triple Negative Breast Cancer (TNBC) is a heterogeneous, molecularly diverse group of breast cancers and are ER (Estrogen Receptor), PR (Progesterone Receptor) and HER2 (Human Epidermal Growth Factor Receptor-2) negative. TNBC accounts for 15-20% of invasive breast cancers, with a higher incidence noted in young patients. It is usually aggressive, and tumors tend to be high grade and patients with TNBC are at a higher risk of both local and distant recurrence. Those with metastatic disease have one of the worst prognoses of all cancers with a median Overall Survival of 13 months. The majority of patients with TNBC who develop metastatic disease do so within the first 3 years after diagnosis, whereas those without recurrence during this period of time have survival rates similar to those with ER-positive breast cancers. The lack of known recurrent oncogenic drivers in patients with metastatic TNBC, presents a major therapeutic challenge. Nonetheless, patients with TNBC often receive chemotherapy in the neoadjuvant, adjuvant or metastatic settings and approximately 30-40% of patients achieve a pathological Complete Response (pCR) in the neoadjuvant setting. In addition to increasing the likelihood of tumor resectability and breast preservation, patients achieving a pCR following neoadjuvant chemotherapy have a longer Event Free Survival (EFS) and Overall Survival (OS). Those who do not achieve a pathological Complete Response tend to have a poor prognosis. For all these reasons, pCR is considered a valid endpoint for clinical testing of neoadjuvant therapy in patients with early stage TNBC. It appears that there are subsets of patients with TNBC who may be inherently insensitive to cytotoxic chemotherapy. Three treatment approaches appear to be promising and they include immune therapies, PARP inhibition and inhibition of PI3K pathway. Previously published studies have shown that presence of tumor-infiltrating lymphocytes was associated with clinical benefit, when treated with chemotherapy and immunotherapy, in patients with TNBC, and improved clinical benefit was observed in patients with immune-enriched molecular subtypes of metastatic TNBC.
KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2. It thereby reverses the PD-1 pathway-mediated inhibition of the immune response and unleashes the tumor-specific effector T cells. Cytotoxic chemotherapy releases tumor-specific antigens and immune checkpoint inhibitors such as KEYTRUDA® when given along with chemotherapy can enhance endogenous anticancer immunity. Preliminary results from Phase I and II trials have shown that in patients with TNBC, KEYTRUDA® given along with chemotherapy in a neoadjuvant setting resulted in a high rate of pCR.
KEYNOTE-522 is an international, placebo controlled Phase III trial, conducted to evaluate the safety and efficacy of neoadjuvant KEYTRUDA® plus chemotherapy followed by adjuvant KEYTRUDA® or placebo, in patients with early stage TNBC. In this study, 1,174 patients were randomly assigned in a 2:1 ratio to receive neoadjuvant KEYTRUDA® 200 mg IV every 3 weeks (N=784) or placebo (N=390). All patients received 4 cycles of Carboplatin plus Paclitaxel, followed by 4 cycles of Doxorubicin or Epirubicin plus Cyclophosphamide, in the neoadjuvant setting. Following definitive surgery, adjuvant KEYTRUDA® or placebo was continued every 3 weeks for 9 cycles or until disease recurrence or unacceptable toxicity. Enrolled TNBC patients were newly diagnosed, treatment naïve, and included both node-negative and node-positive patients with nonmetastatic disease (Tumor Stage T1c, Nodal Stage N1-N2 or Tumor Stage T2-T4, Nodal Stage N0-N2, per AJCC criteria). Treatment groups were well balanced and patients were stratified according to nodal status, tumor size, and Carboplatin schedule (weekly versus every 3 weeks). The two Primary endpoints were pathological Complete Response (pCR) at the time of definitive surgery and Event Free Survival (EFS). The median follow up was 15.5 months.
At the first interim analysis, the pCR among the first 602 patients who underwent randomization was 64.8% in the KEYTRUDA® plus chemotherapy group, compared with 51.2% in the placebo plus chemotherapy group (P<0.001). This pCR benefit was consistent across subgroups including PD-L1 expresssion subgroups. In the PD-L1-positive population, the pCR was 68.9% in the KEYTRUDA® plus chemotherapy group compared with 54.9% in the placebo plus chemotherapy group. In the PD-L1 negative group, the pCR in the KEYTRUDA® plus chemotherapy group was 45.3% and 30.3% in the placebo plus chemotherapy group. Neoadjuvant KEYTRUDA® plus chemotherapy followed by adjuvant KEYTRUDA® showed a favorable trend for Event Free Survival compared with chemotherapy alone, although these data are still premature. Across all treatment phases, Grade 3 or higher treatment-related toxicities were 78.0% in the KEYTRUDA® plus chemotherapy group and 73.0% in the placebo plus chemotherapy group.
It was concluded that among patients with early stage Triple Negative Breast Cancer, the addition of KEYTRUDA® to neoadjuvant chemotherapy significantly increased the pathological Complete Response rate, compared to those who received placebo plus neoadjuvant chemotherapy, with a favorable trend in Event Free Survival. Pembrolizumab for Early Triple-Negative Breast Cancer. Schmid P, Cortés J, Pusztai L, et al. for the KEYNOTE-522 Investigators. N Engl J Med 2020;382:810-821
CDK4/6 Inhibitors May Replace Chemotherapy in HR-Positive, HER2-Negative Metastatic Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease. Approximately 70% of breast tumors express Estrogen Receptors and/or Progesterone Receptors and the most common subtype of metastatic breast cancer is Hormone Receptor-positive (HR-positive), HER2-negative breast cancer (65% of all metastatic breast tumors), and these patients are often treated with anti-estrogen therapy as first line treatment. However, resistance to hormonal therapy occurs in a majority of the patients with a median Overall Survival (OS) of 36 months. Cyclin Dependent Kinases (CDK) play a very important role to facilitate orderly and controlled progression of the cell cycle. Genetic alterations in these kinases and their regulatory proteins have been implicated in various malignancies.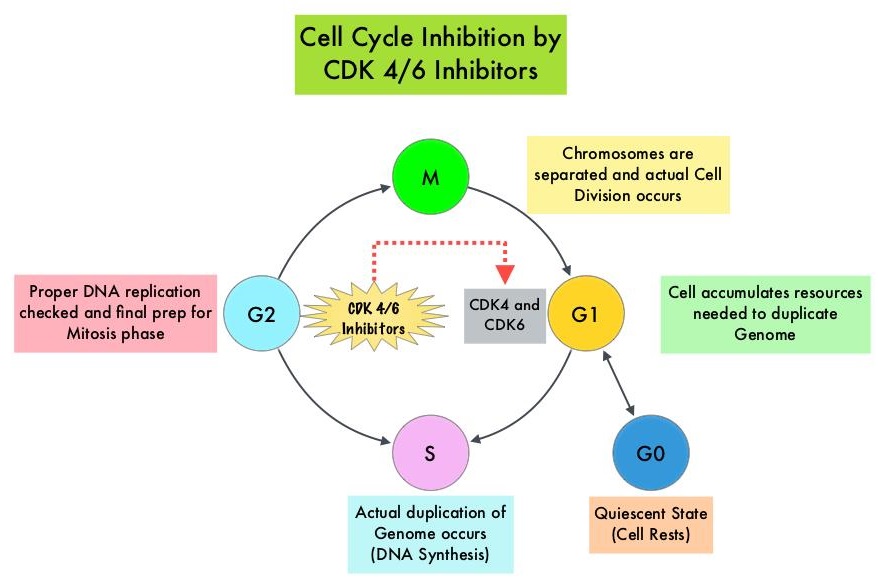
Cyclin Dependent Kinases 4 and 6 (CDK4 and CDK6) phosphorylate RetinoBlastoma protein (RB), and initiate transition from the G1 phase to the S phase of the cell cycle. RetinoBlastoma protein has antiproliferative and tumor-suppressor activity and phosphorylation of RB protein nullifies its beneficial activities. CDK4 and CDK6 are activated in hormone receptor positive breast cancer, promoting breast cancer cell proliferation. Further, there is evidence to suggest that endocrine resistant breast cancer cell lines depend on CDK4 for cell proliferation. The understanding of the role of Cyclin Dependent Kinases in the cell cycle, has paved the way for the development of CDK inhibitors.
Even though major international oncology treatment guidelines recommend a sequence of endocrine based therapies with or without targeted therapies in postmenopausal women with HR-positive, HER2-negative metastatic breast cancer, Real-World Data suggests that upfront use of chemotherapy remains common even in the absence of visceral crisis. This treatment approach may partly be due to paucity of data directly comparing hormonal therapies with chemotherapy regimens, in this patient group. To provide guidance with additional evidence, the authors conducted a comprehensive systematic review and network meta-analysis to evaluate the efficacy and activity of several first or second line hormonal therapy and chemotherapy regimens that have been investigated in randomized controlled trials, and the researchers aimed to compare these two different approaches.
This analysis included all Phase II and III randomized controlled trials investigating chemotherapy with or without targeted therapies and hormone therapies with or without targeted therapies as first-line or second-line treatments, or both, in postmenopausal women with HR-positive, HER2-negative metastatic breast cancer. Relevant examples of new targeted therapies are mTOR inhibitor Everolimus (AFINITOR®), CDK4/6 inhibitors Palbociclib (IBRANCE®), Ribociclib (KISQALI®) and Abemaciclib (VERZENIO®), and PI3K inhibitor Alpelisib (PIQRAY®), which are used in combination with endocrine therapy. Following a literature search on PubMed, Embase, Cochrane Central Register of Clinical Trials, Web of Science, and online archives of the most relevant international oncology conferences published between Jan 1, 2000 and Dec 31, 2017, 140 studies were selected, comprising of 50,029 patients. Studies exclusively enrolling premenopausal patients and those with HER2-positive or triple-negative breast cancer were excluded from this analysis. The median age was 58 yrs and median follow up was 20 months. All treatments were compared to Anastrozole (ARIMIDEX®) and to CDK4/6 inhibitor Palbociclib (IBRANCE®) plus Letrozole (FEMARA®). The Primary outcome was Progression Free Survival (PFS) and the Secondary outcome was Overall Response Rate.
In this analysis, it was noted that CDK4/6 inhibitors and PIK3K inhibitor (in patients with PIK3CA mutation) along with endocrine therapy was superior to standard endocrine therapy such as Anastrozole alone or Fulvestrant (FASLODEX®) alone, with significantly better PFS. Chemotherapy regimens with or without targeted agents were not significantly better than CDK4/6 inhibitors plus endocrine therapy. Further, the combination of CDK4/6 inhibitors plus endocrine therapy was associated with a favorable toxicity profile compared to chemotherapy. There were no significant differences noted in PFS among the three CDK4/6 inhibitors in combination with an Aromatase Inhibitor or Fulvestrant.
The authors concluded that in the first and second line setting, CDK4/6 inhibitors plus endocrine therapies are superior to standard single agent endocrine therapies in terms of Progression Free Survival. Moreover, no chemotherapy regimen with or without targeted therapy is significantly better than CDK4/6 inhibitors plus endocrine therapies in terms of Progression Free Survival. The researchers added that this is the first study to directly compare all three CDK4/6 inhibitors combined with an Aromatase Inhibitor or Fulvestrant. Endocrine treatment versus chemotherapy in postmenopausal women with hormone receptor-positive, HER2-negative, metastatic breast cancer: a systematic review and network meta-analysis. Giuliano M, Schettini F, Rognoni C, et al. Lancet Oncol. 2019;20:1360-1369.
Cyclin Dependent Kinases 4 and 6 (CDK4 and CDK6) phosphorylate RetinoBlastoma protein (RB), and initiate transition from the G1 phase to the S phase of the cell cycle. RetinoBlastoma protein has antiproliferative and tumor-suppressor activity and phosphorylation of RB protein nullifies its beneficial activities. CDK4 and CDK6 are activated in hormone receptor positive breast cancer, promoting breast cancer cell proliferation. Further, there is evidence to suggest that endocrine resistant breast cancer cell lines depend on CDK4 for cell proliferation. The understanding of the role of Cyclin Dependent Kinases in the cell cycle, has paved the way for the development of CDK inhibitors.
Even though major international oncology treatment guidelines recommend a sequence of endocrine based therapies with or without targeted therapies in postmenopausal women with HR-positive, HER2-negative metastatic breast cancer, Real-World Data suggests that upfront use of chemotherapy remains common even in the absence of visceral crisis. This treatment approach may partly be due to paucity of data directly comparing hormonal therapies with chemotherapy regimens, in this patient group. To provide guidance with additional evidence, the authors conducted a comprehensive systematic review and network meta-analysis to evaluate the efficacy and activity of several first or second line hormonal therapy and chemotherapy regimens that have been investigated in randomized controlled trials, and the researchers aimed to compare these two different approaches.
This analysis included all Phase II and III randomized controlled trials investigating chemotherapy with or without targeted therapies and hormone therapies with or without targeted therapies as first-line or second-line treatments, or both, in postmenopausal women with HR-positive, HER2-negative metastatic breast cancer. Relevant examples of new targeted therapies are mTOR inhibitor Everolimus (AFINITOR®), CDK4/6 inhibitors Palbociclib (IBRANCE®), Ribociclib (KISQALI®) and Abemaciclib (VERZENIO®), and PI3K inhibitor Alpelisib (PIQRAY®), which are used in combination with endocrine therapy. Following a literature search on PubMed, Embase, Cochrane Central Register of Clinical Trials, Web of Science, and online archives of the most relevant international oncology conferences published between Jan 1, 2000 and Dec 31, 2017, 140 studies were selected, comprising of 50,029 patients. Studies exclusively enrolling premenopausal patients and those with HER2-positive or triple-negative breast cancer were excluded from this analysis. The median age was 58 yrs and median follow up was 20 months. All treatments were compared to Anastrozole (ARIMIDEX®) and to CDK4/6 inhibitor Palbociclib (IBRANCE®) plus Letrozole (FEMARA®). The Primary outcome was Progression Free Survival (PFS) and the Secondary outcome was Overall Response Rate.
In this analysis, it was noted that CDK4/6 inhibitors and PIK3K inhibitor (in patients with PIK3CA mutation) along with endocrine therapy was superior to standard endocrine therapy such as Anastrozole alone or Fulvestrant (FASLODEX®) alone, with significantly better PFS. Chemotherapy regimens with or without targeted agents were not significantly better than CDK4/6 inhibitors plus endocrine therapy. Further, the combination of CDK4/6 inhibitors plus endocrine therapy was associated with a favorable toxicity profile compared to chemotherapy. There were no significant differences noted in PFS among the three CDK4/6 inhibitors in combination with an Aromatase Inhibitor or Fulvestrant.
The authors concluded that in the first and second line setting, CDK4/6 inhibitors plus endocrine therapies are superior to standard single agent endocrine therapies in terms of Progression Free Survival. Moreover, no chemotherapy regimen with or without targeted therapy is significantly better than CDK4/6 inhibitors plus endocrine therapies in terms of Progression Free Survival. The researchers added that this is the first study to directly compare all three CDK4/6 inhibitors combined with an Aromatase Inhibitor or Fulvestrant. Endocrine treatment versus chemotherapy in postmenopausal women with hormone receptor-positive, HER2-negative, metastatic breast cancer: a systematic review and network meta-analysis. Giuliano M, Schettini F, Rognoni C, et al. Lancet Oncol. 2019;20:1360-1369.
ENHERTU® (fam-Trastuzumab deruxtecan-nxki)
The FDA on December 20, 2019 granted accelerated approval to ENHERTU® for patients with unresectable or metastatic HER2-positive breast cancer, who have received two or more prior anti-HER2-based regimens in the metastatic setting. ENHERTU® is a product of Daiichi Sankyo.
FDA Approves ENHERTU® for Advanced HER2-Positive Breast Cancer
SUMMARY: The FDA on December 20, 2019, granted accelerated approval to ENHERTU® (Trastuzumab deruxtecan) for patients with unresectable or metastatic HER2-positive breast cancer, who have received two or more prior anti-HER2-based regimens in the metastatic setting. Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 268,600 new cases of invasive breast cancer will be diagnosed in 2019 and about 41,760 women will die of the disease. The HER or erbB family of receptors consist of HER1, HER2, HER3 and HER4. Approximately 15-20% of invasive breast cancers overexpress HER2/neu oncogene, which is a negative predictor of outcomes without systemic therapy. Patients with HER2-positive metastatic breast cancer are often treated with anti-HER2 targeted therapy along with chemotherapy, irrespective of hormone receptor status, and this has resulted in significantly improved treatment outcomes. HER2-targeted therapies include HERCEPTIN® (Trastuzumab), TYKERB® (Lapatinib), PERJETA® (Pertuzumab) and KADCYLA® (ado-Trastuzumab emtansine). Dual HER2 blockade with HERCEPTIN® and PERJETA®, given along with chemotherapy (with or without endocrine therapy), as first line treatment, in HER2 positive metastatic breast cancer patients, was shown to significantly improve Progression Free Survival (PFS) as well as Overall Survival (OS). The superior benefit with dual HER2 blockade has been attributed to differing mechanisms of action and synergistic interaction between HER2 targeted therapies. Patients progressing on Dual HER2 blockade often receive KADCYLA® which results in an Objective Response Rate (ORR) of 44% and a median PFS of 9.6 months, when administered after HERCEPTIN® and a taxane. There is however no standard treatment option for this patient population following progression on KADCYLA®.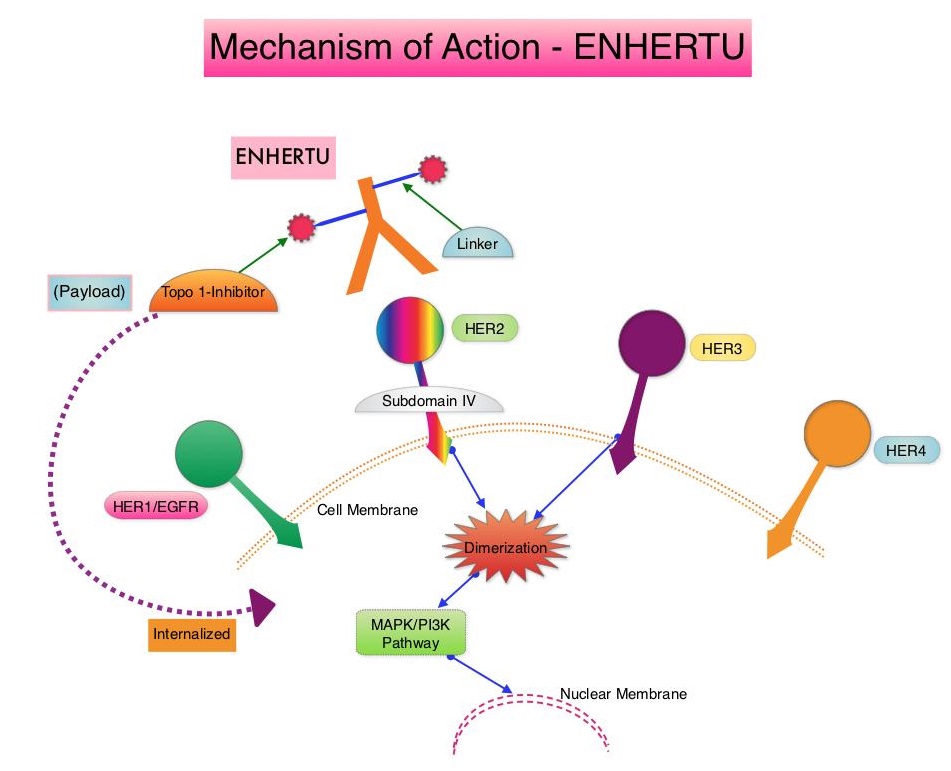
ENHERTU® is an Antibody-Drug Conjugate (ADC) composed of a humanized monoclonal antibody specifically targeting HER2, with the amino acid sequence similar to Trastuzumab, a cleavable tetrapeptide-based linker, and a potent cytotoxic Topoisomerase I inhibitor as the cytotoxic drug (payload). ENHERTU® has a favorable pharmacokinetic profile and the tetrapeptide-based linker is stable in the plasma and is selectively cleaved by cathepsins that are up-regulated in tumor cells. Unlike KADCYLA®, ENHERTU® has a higher drug-to-antibody ratio (8 versus 4), released payload easily crosses the cell membrane with resulting potent cytotoxic effect on neighboring tumor cells regardless of target expression, and the released cytotoxic agent (payload) has a short half-life, minimizing systemic exposure. In a Phase 1 dose-finding study involving patients with advanced HER2-positive breast cancer, treatment with ENHERTU® resulted in a confirmed response rate was 59.5%, and the median response duration was 20.7 months. However, the efficacy of ENHERTU® in patients with HER2-positive metastatic breast cancer, previously treated with KADCYLA® remained unclear.
The present FDA approval was based on DESTINY-Breast01 study, which is a multicenter, single-arm, Phase II trial, in which 184 patients with HER2-positive, metastatic breast cancer, who had received two or more prior HER2 targeted therapies including KADCYLA®, were enrolled. Patients received ENHERTU® 5.4 mg/kg IV every 3 weeks until disease progression or unacceptable toxicity. The median age was 55 years, 53% had Hormone Receptor-positive tumors and the median number of previous lines of therapy for metastatic disease was six and included KADCYLA® (100%), Trastuzumab (100%), Pertuzumab (66%), and other anti-HER2 therapies (54%). The Primary end point was Objective Response Rate (ORR) assessed by Independent Central Review and Secondary endpoints included Duration of Response, Progression Free Survival (PFS) and Overall Survival (OS). The median follow up was 11.1 months. The ORR was 60.9%, with 6% Complete Responses and 54.9% Partial Responses. The median time to response was 1.6 months and the median response duration was 14.8 months. The median PFS was 16.4 months the median OS was not reached at the time of this publication. The most Grade 3 or higher adverse events were cytopenias, nausea, diarrhea and Interstitial Lung Disease.
It was concluded that ENHERTU® has a high level of clinical efficacy with a durable antitumor activity in a pretreated patient population with HER2-positive metastatic breast cancer. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast Cancer. Modi S, Saura C, Yamashita T, et al. for the DESTINY-Breast01 Investigators. N Engl J Med. 2019 Dec 11. doi: 10.1056/NEJMoa1914510. [Epub ahead of print]
Long-Term Breast Cancer Preventive Benefit with ARIMIDEX®
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 268,600 new cases of invasive breast cancer will be diagnosed in 2019 and about 41,760 women will die of the disease. Some high risk factors for the development of breast cancer include first-degree relative with breast cancer at any age, first-degree relative with bilateral breast cancer who developed the first breast cancer at 50 years of age or less, Lobular Carcinoma In Situ (LCIS), Atypical ductal or lobular hyperplasia in a benign lesion, and Ductal Carcinoma In-Situ (DCIS).
Previously published studies have shown a 38% reduction in all breast cancers and 50% reduction of ER-positive tumors with the use of SERMs (Selective Estrogen Receptor Modulators) such as Tamoxifen and Raloxifene for breast cancer prevention. Further it has been shown that the effects of Tamoxifen continue with a constant 29% annual preventive effect for at least 15 years after completion of treatment. A further improvement in breast cancer incidence short-term was seen in two trials using, two Aromatase Inhibitors, ARIMIDEX® (Anastrozole) in the International Breast Cancer Intervention Study II (IBIS-II) and AROMASIN® (Exemestane) in the MAP.3 trial. However in the MAP.3 study, the study was unblinded after the initial publication and a post-treatment effect, as was seen with Tamoxifen, was not possible.
The International Breast Cancer Intervention Study II (IBIS-II) is an international, randomized, double-blind, placebo-controlled trial, which was initiated in 2003. In this trial, 3864 postmenopausal women aged 40-70 years, at increased risk of developing breast cancer were recruited and were randomly assigned (1:1) to either ARIMIDEX® 1 mg orally daily (N=1920) or matching placebo (N=1944) daily for 5 years. After treatment completion, women were followed on a yearly basis and data was collected on breast cancer incidence, death, incidence of other cancers, and major adverse events (cardiovascular events and fractures). The median age at study entry was 59 years. The exclusion criteria for this study included premenopausal status, prior breast cancer including Ductal Carcinoma In Situ (DCIS) diagnosed more than 6 months before trial entry, current or previous Tamoxifen, Raloxifene, or other SERM use for more than 6 months, or previous or planned prophylactic mastectomy. Unblinding was only permitted if the participant developed breast cancer, when a clinician considered there to be valid medical or safety reasons. The Primary outcome was the development of histologically confirmed breast cancer, either invasive or non-invasive (DCIS), particularly during the post-5-year time period. Secondary outcomes were ER-positive breast cancer, breast cancer mortality, incidence of other cancers, cardiovascular disease, fractures, and all-cause mortality. The decision to analyze the data was made without looking at the results before hand. The first analysis after a median follow-up of 60 months showed a significant reduction (53%) in incidence for all breast cancer (including DCIS). The authors now report the results on the extended duration of benefit of ARIMIDEX® in preventing breast cancer, for up to 12 years after trial entry.
After a median follow up of 10.9 years for this analysis, women assigned to the ARIMIDEX® group were 49% less likely to develop breast cancer than women assigned to the placebo arm of the study ((HR=0.51, P<0.0001). The reduction in incidence in the first 5 years of follow up was 61% (HR=0.39; P<0.0001), and a smaller but still significant 36% reduction (HR=0.64; P=0•014) was seen in subsequent years, which was still larger than that seen for Tamoxifen in previous trials, and the effects in the two time periods was not significantly different (P=0.08). Invasive ER-positive breast cancer was reduced by 54% with ARIMIDEX® treatment (HR=0.46; P<0.0001), with a continued significant effect observed in the post-treatment follow up period. A 59% reduction in DCIS overall was observed (HR=0.41; P=0.0081), with a very large reduction noted in those cases known to be ER-positive (HR = 0.22; P<0.0001). A significant decrease in non-breast cancers was observed in the ARIMIDEX® group, primarily contributed by non-melanoma skin cancer (P=0.0042), and no excess rates of fractures or cardiovascular disease was observed.
The authors concluded that this updated analysis shows a continuing long-term effect of 5 years of ARIMIDEX® treatment, in preventing breast cancer, in high-risk postmenopausal women. These new results strongly suggest that ARIMIDEX® should be preferred therapy for breast cancer prevention in postmenopausal women at increased risk for the disease, with Tamoxifen used for women who experience severe side effects from ARIMIDEX®. Use of anastrozole for breast cancer prevention (IBIS-II): long-term results of a randomised controlled trial. Cuzick J, Sestak I, Forbes JF, et al. The Lancet. Published:December 12, 2019. DOI:https://doi.org/10.1016/S0140-6736(19)32955-1
Supplemental MRI Screening for Women with Extremely Dense Breast Tissue
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 268,600 new cases of invasive breast cancer will be diagnosed in 2019 and about 41,760 women will die of the disease. Screening mammography complemented by breast self exam and clinical breast exam has resulted in early detection of breast cancer and successful outcomes. Even though mammography is a sensitive screening test, a small percentage of breast cancers may not show up on mammograms but may be palpable on examination by the patient or the clinician. Further, mammograms are less likely to find breast tumors in younger women with dense breast tissue. A breast Magnetic Resonance Imaging (MRI) is more sensitive than mammography although the specificity of a breast MRI is lower, resulting in a higher rate of false-positive findings and potentially unnecessary biopsies. Microcalcifications in the breast can be missed by a breast MRI. Taking these factors into consideration, appropriate utilization of breast MRI becomes relevant.
The American Cancer Society (ACS) recommends an annual MRI as an adjunct to screening mammogram and clinical breast exam in certain groups with increased risk of breast cancer. In a study published by Stout NK, et al., (JAMA Intern Med. 2014;174:114-121), it was noted that breast MRI was over utilized in those who did not fit the ACS criteria and was under utilized in those with documented genetic mutations. Routine breast MRI screening is not recommended for a new breast cancer diagnosis or for breast cancer surveillance and should only be considered for the group of individuals who have the most benefit. Breast MRI is performed preferably between days 7-15 of menstrual cycle for premenopausal women, using a dedicated breast coil, with the ability to perform a biopsy under MRI guidance by experienced radiologists, during the same visit.
DENSE trial is a multicenter, randomized, controlled study which evaluated the effect of supplemental Magnetic Resonance Imaging (MRI) on the incidence of interval cancers, in women with extremely dense breast tissue. In this trial, 40,373 women between the ages of 50 and 75 years with extremely dense breast tissue and normal results on screening mammography were randomly assigned in a 1:4 ratio to a group that was invited to undergo supplemental MRI (N=8061) or to a group that received mammography screening alone (N=32,312). Of the women who were invited to undergo MRI, 59% accepted the invitation (N=4783). All MRI examinations were performed with the use of a dedicated bilateral breast coil. The Primary endpoint was the difference in the incidence of interval cancers during a 2-year screening period, between the mammography screening-only group and MRI-invitation group. Secondary endpoints included the recall rate for additional examination, the cancer-detection rate on MRI, the false positive rate, the positive predictive value, and tumor characteristics.
The interval cancer rate was 2.5 per 1000 screenings in the MRI-invitation group and 5.0 per 1000 screenings in the mammography-only group (P<0.001). The MRI cancer-detection rate among the women who actually underwent MRI screening was 16.5 per 1000 screenings. The Positive Predictive Value of a positive MRI result was 17.4%, the Positive Predictive Value of an indication for biopsy was 23.9% and the Positive Predictive Value of a biopsy was 26.3%. The false positive rate was 79.8 per 1000 screenings. As a result of the MRI screening, 300 women underwent a breast biopsy and of these women, breast cancer was diagnosed in 79 women, of whom 64 had invasive breast cancer and 15 were diagnosed with DCIS.
The authors concluded that the use of supplemental MRI screening in women with extremely dense breast tissue and normal results on mammography resulted in the diagnosis of significantly fewer interval cancers than mammography alone, during a 2-year screening period. Whether a reduction in interval cancers is an appropriate surrogate for improved Overall Survival, remains unclear. Supplemental MRI Screening for Women with Extremely Dense Breast Tissue. Bakker MF, de Lange SV, Pijnappel RM, et al. for the DENSE Trial Study Group. N Engl J Med 2019; 381:2091-2102