
The FDA on November 13, 2020 granted accelerated approval to KEYTRUDA® in combination with chemotherapy for the treatment of patients with locally recurrent unresectable or metastatic Triple-Negative Breast Cancer (TNBC) whose tumors express PD-L1 (CPS 10 or more), as determined by an FDA approved test. KEYTRUDA® is a product of Merck & Co.
Tag: Breast Cancer
Adjuvant Trastuzumab Monotherapy for Older Patients with HER-2 Positive Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (13%) will develop invasive breast cancer during their lifetime. Approximately 276,480 new cases of invasive female breast cancer will be diagnosed in 2020 and about 42,170 women will die of the disease. Approximately 15-20% of invasive breast cancers overexpress HER2/neu oncogene, which is a negative predictor of outcomes without systemic therapy. Trastuzumab is a humanized monoclonal antibody targeting HER2. Adjuvant and neoadjuvant chemotherapy given along with Trastuzumab reduces the risk of disease recurrence and death, among patients with HER2-positive, early stage as well as advanced metastatic breast cancer. Since the approval of Trastuzumab, several other HER2-targeted therapies have become available. The duration of adjuvant Trastuzumab therapy has been 12 months and this length of treatment was empirically adopted from the pivotal registration trials.
Elderly patients with HER-2 positive breast cancer may not be candidates for adjuvant chemotherapy. Single agent Trastuzumab used as adjuvant treatment without chemotherapy could be of potential benefit, avoiding chemotherapy-induced toxicities. However, the benefit of single agent Trastuzumab has not been investigated in patients older than 70 years. The present study was designed to investigate the efficacy of Trastuzumab monotherapy, compared with Trastuzumab in combination with chemotherapy, incidence of Adverse Events, as well as Quality of Life, in terms of the noninferiority criterion.
RESPECT Study is a multicenter, open-label, randomized controlled, prospective, adjuvant, noninferiority trial, in which Trastuzumab monotherapy was compared with Trastuzumab plus chemotherapy, among patients older than 70 years, with HER-2 positive breast cancer. A total of 275 patients, aged 70-80 years with surgically treated HER-2 positive invasive breast cancer, were randomly assigned in a 1:1 ratio to receive either Trastuzumab monotherapy (N=137) or Trastuzumab plus chemotherapy (N=138). Trastuzumab plus chemotherapy treatment consisted of a loading dose of Trastuzumab at 8 mg/kg and a maintenance dose of 6 mg/kg every 3 weeks for 1 year. Chemotherapy regimens consisted of either Paclitaxel 80 mg/m2 IV weekly for 12 weeks, Docetaxel 75 mg/m2 IV every 3 weeks for 4 cycles, Doxorubicin 60 mg/m2 IV and Cyclophosphamide 600 mg/m2 IV (AC) every 3 weeks for 4 cycles, Epirubicin 90 mg/m2 IV and Cyclophosphamide 600 mg/m2 IV (EC) every 3 weeks for 4 cycles, Cyclophosphamide 75-100 mg orally, Methotrexate 40 mg/m2, and 5-fluorouracil 500-600 mg/m2 IV (CMF) for 6 cycles, Docetaxel 75 mg/m2 IV and Cyclophosphamide 600 mg/m2 IV (TC) every 3 weeks for 4 cycles or Docetaxel 60-75 mg/m2 IV, Carboplatin AUC 5-6 mg/ml/min IV along with Trastuzumab IV (TCH) every 3 weeks for 6 cycles. Patients treated with Trastuzumab monotherapy received similar doses of loading and maintenance Trastuzumab. Patients were stratified based on Performance Status, Hormone Receptor status and pathologic nodal status. Approximately 44% of patients had Stage I disease, 42% had Stage IIA, 13% had IIB, and 1% had IIIA disease. Approximately 14% of patients received Selective Estrogen Receptor Modulators such as Tamoxifen, and about 69% of patients received Aromatase Inhibitors. The Primary endpoint was Disease Free Survival (DFS) with assessment of prespecified Hazard Ratio (HR) and Restricted Mean Survival Time (RMST) for each treatment group. (RMST has been advocated as an alternative or a supplement to the Hazard Ratio for reporting the effect of an intervention in a randomized clinical trial, and is a measure of average survival from time 0 to a specified time point, and may be estimated as the area under the KM curve up to that point. RMST measure is especially informative for older patient populations in which Quality of Life issues are more important). Secondary endpoints included Overall Survival (OS), Relapse-Free Survival (RFS), Adverse Events (AEs) and Health-Related Quality of Life (HRQoL). The median follow up time was 4.1 years.
The 3-year DFS was 89.5% with Trastuzumab monotherapy versus 93.8% with Trastuzumab plus chemotherapy (HR=1.36; P=0.51) and this study failed to meet the prespecified criterion for noninferiority. However, a preplanned analysis of DFS according to RMST was -0.39 months, suggesting that only 0.39 months of DFS were lost within 3 years, by avoiding chemotherapy. The 3-year RFS was 92.4% with Trastuzumab monotherapy versus 95.3% with Trastuzumab plus chemotherapy (HR=1.33) and the difference in RMST for RFS between treatment groups at 3 years was −0.41 months (P=0.53). There were significant differences noted in clinically meaningful HRQoL deterioration rate at 2 months (31% for Trastuzumab monotherapy versus 48% for Trastuzumab plus chemotherapy; P=.016) and at 1 year (19% versus 38%; P=0.009). Breast cancer-specific survival at 3 years was 99.2% with Trastuzumab monotherapy versus 99.2% with Trastuzumab plus chemotherapy (HR=0.20; P=0.14).
The authors concluded that even though the Primary endpoint of noninferiority for Trastuzumab monotherapy was not met, the Restricted Mean Survival Time revealed that the observed loss of survival without chemotherapy was less than 1 month at 3 years, and Health-Related Quality of Life was better, with lower toxicities. Therefore, Trastuzumab monotherapy can be considered as a reasonable adjuvant therapy option for a select group of elderly patients with favorable outcomes.
Randomized Controlled Trial of Trastuzumab With or Without Chemotherapy for HER2-Positive Early Breast Cancer in Older Patients. Sawaki M, Taira N, Uemura Y, et al. J Clin Oncol. 2020;38:3743-3752.
FDA Approves KEYTRUDA® Plus Chemotherapy for Triple Negative Breast Cancer
SUMMARY: The FDA on November 13, 2020, granted accelerated approval to KEYTRUDA® (Pembrolizumab) in combination with chemotherapy for the treatment of patients with locally recurrent, unresectable or metastatic, Triple Negative Breast Cancer (TNBC), whose tumors express PD-L1 (Combined Positive Score-CPS 10 or more) as determined by an FDA approved test. Breast cancer is the most common cancer among women in the US and about 1 in 8 women (13%) will develop invasive breast cancer during their lifetime. Approximately 276,480 new cases of invasive female breast cancer will be diagnosed in 2020 and about 42,170 women will die of the disease. Triple Negative Breast Cancer (TNBC) is a heterogeneous, molecularly diverse group of breast cancers and are ER (Estrogen Receptor), PR (Progesterone Receptor) and HER2 (Human Epidermal Growth Factor Receptor-2) negative. TNBC accounts for 15-20% of invasive breast cancers, with a higher incidence noted in young patients and African American females. It is usually aggressive, and tumors tend to be high grade, and patients with TNBC are at a higher risk of both local and distant recurrence and often develop visceral metastases. Those with metastatic disease have one of the worst prognoses of all cancers with a median Overall Survival of 13 months. The majority of patients with TNBC who develop metastatic disease do so within the first 3 years after diagnosis, whereas those without recurrence during this period of time have survival rates, similar to those with ER-positive breast cancers. The lack of known recurrent oncogenic drivers in patients with metastatic TNBC, presents a major therapeutic challenge. Overall survival among patients with pretreated metastatic TNBC has not changed over the past 2 decades and standard chemotherapy is associated with low response rates of 10-15% and a Progression Free Survival (PFS) of only 2-3 months.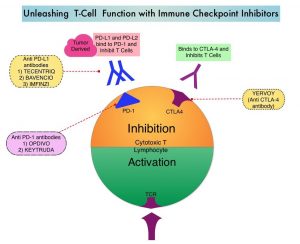
KEYTRUDA® is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2. It thereby reverses the PD-1 pathway-mediated inhibition of the immune response, and unleashes the tumor-specific effector T cells. The rationale for combining chemotherapy with immunotherapy is that cytotoxic chemotherapy releases tumor-specific antigens, and immune checkpoint inhibitors such as KEYTRUDA® when given along with chemotherapy can enhance endogenous anticancer immunity. Single agent KEYTRUDA® in metastatic TNBC demonstrated durable antitumor activity in several studies, with Objective Response Rates (ORRs) ranging from 10% to 21% and improved clinical responses in patients with higher PD-L1 expression. When given along with chemotherapy as a neoadjuvant treatment for patients with high-risk, early-stage TNBC, KEYTRUDA® combination achieved Pathological Complete Response rate of 65%, regardless of PD-L1 expression. Based on this data, KEYTRUDA® in combination with chemotherapy was studied, for first-line treatment of TNBC.
KEYNOTE-355 is a randomized, double-blind, Phase III study, which evaluated the benefit of KEYTRUDA® in combination with one of the three different chemotherapy regimens, nab-Paclitaxel, Paclitaxel, or the non-taxane containing Gemzar/Carboplatin, versus placebo plus one of the three chemotherapy regimens, in patients with previously untreated or locally recurrent inoperable metastatic TNBC. In this study, 847 patients were randomized 2:1 to receive either KEYTRUDA® 200 mg IV on day 1 of each 21-day cycle along with either nab-paclitaxel 100 mg/m2 IV on days 1, 8 and 15 of each 28-day cycle, Paclitaxel 90 mg/m2 IV on days 1, 8 and 15 of each 28-day cycle, or Gemcitabine 1000 mg/m2 IV plus Carboplatin AUC 2, IV on days 1 and 8 of each 21-day cycle (N= 566) or placebo along with one of the three chemotherapy regimens (N= 281). This study was not designed to compare the efficacy of the different chemotherapy regimens. Treatment was continued until disease progression. Patients were stratified by chemotherapy, PD-L1 tumor expression (CPS of 1 or higher versus CPS of less than 1), and prior treatment with the same class of neoadjuvant/adjuvant chemotherapy (Yes versus No). The baseline characteristics of treatment groups were well-balanced. The co-Primary end points of the trial were Progression Free Survival (PFS) and Overall Survival (OS) in patients with PD-L1-positive tumors, and in all patients. Secondary end points were Objective Response Rate (ORR), Duration of Response, Disease Control Rate, and Safety. The median follow up for patients assigned to receive KEYTRUDA® was 17.5 months and 15.5 months for the placebo group. The authors reported the results from an interim analysis conducted by an Independent Data Monitoring Committee (IDMC).
KEYTRUDA® in combination with chemotherapy, significantly improved PFS in patients with CPS (Combined Positive Score) of 10 or greater. The median PFS was 9.7 months for KEYTRUDA® plus chemotherapy, compared with 5.6 months for placebo plus chemotherapy (HR=0.65, P=0.0012). This represented a 35% reduction in the risk of disease progression. Among patients with CPS of 1 or greater, the median PFS was 7.6 months for KEYTRUDA® plus chemotherapy, compared with 5.6 months for the placebo plus chemotherapy arm (HR= 0.74; P=0.0014). This however based on prespecified statistical criteria, was not considered statistically significant. Among the entire Intention-To-Treat (ITT) population, the median PFS was 7.5 months in the KEYTRUDA® plus chemotherapy group, compared with 5.6 months for chemotherapy plus placebo group (HR=0.82). Formal statistical significance was not tested in the ITT population. Overall Survival data are pending. Adverse Events (AEs) were similar in both treatment groups, although immune-related AEs occurred at a higher incidence in the KEYTRUDA® arm.
It was concluded that KEYTRUDA® in combination with several chemotherapy regimens, showed a statistically significant and clinically meaningful improvement in PFS, compared with chemotherapy alone, in patients with previously untreated locally recurrent, inoperable or metastatic TNBC, whose tumors expressed PD-L1 with a Combined Positive Score (CPS) of 10 or more. This data may be particularly relevant for patients who may have received a taxane in the adjuvant setting within a year, and could be more appropriately treated with a non-taxane regimen, in combination with KEYTRUDA®.
KEYNOTE-355: Randomized, double-blind, phase III study of pembrolizumab + chemotherapy versus placebo + chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer. Cortes J, Cescon DW, Rugo HS. et al. J Clin Oncol 38: 2020 (suppl; abstr 1000)
NERLYNX® Combination Superior to TYKERB® Combination in Advanced HER2-Positive Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (13%) will develop invasive breast cancer during their lifetime. Approximately 276,480 new cases of invasive female breast cancer will be diagnosed in 2020 and about 42,170 women will die of the disease. The HER or erbB family of receptors consist of HER1, HER2, HER3 and HER4. Approximately 15-20% of invasive breast cancers overexpress HER2/neu oncogene, which is a negative predictor of outcomes without systemic therapy. Patients with HER2-positive metastatic breast cancer are often treated with anti-HER2 targeted therapy along with chemotherapy, irrespective of hormone receptor status, and this has resulted in significantly improved treatment outcomes.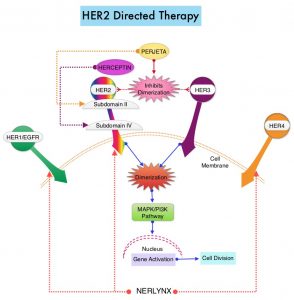
NERLYNX® (Neratinib) is a potent, irreversible, oral Tyrosine Kinase Inhibitor, of HER1, HER2 and HER4 (pan-HER inhibitor). NERLYNX® interacts with the catalytic domain of HER1, HER2, and HER4 and blocks their downstream signaling pathways, resulting in decreased cell proliferation and increased cell death. Clinical data has suggested that NERLYNX® has significant activity in suppressing HER-mediated tumor growth and is able to overcome tumor escape mechanisms experienced with current HER2-targeted and chemotherapeutic agents. It has been well known that hormone receptor positive breast cancer patients, who are also HER2-positive, have relative resistance to hormone therapy. Preclinical models had suggested that the addition of NERLYNX® could improve responses in ER positive, HER2-positive breast cancer patients. Further, NERLYNX® has clinical activity in patients with HER2-positive metastatic breast cancer. NERLYNX® is the first TKI approved by the FDA, shown to reduce the risk for disease recurrence, in patients with early stage HER2-positive breast cancer. NERLYNX® when given for 12 months after chemotherapy and HERCEPTIN®-based adjuvant therapy, to women with HER2-positive breast cancer, significantly reduced the proportion of clinically relevant breast cancer relapses that might lead to death, such as distant and locoregional recurrences outside the preserved breast.
TYKERB® (Lapatinib) is a Tyrosine Kinase Inhibitor of HER2 and EGFR, and in a previously published Phase III study, a combination of TYKERB® plus XELODA® (Capecitabine) was found to be superior to XELODA® alone in women with HER2-positive advanced breast cancer, that has progressed after treatment with regimens that included an Anthracycline, a Taxane, and HERCEPTIN®. (N Engl J Med 2006; 355:2733-2743)
The NALA trial was designed to compare NERLYNX® plus XELODA® versus TYKERB® plus XELODA® in patients with heavily pretreated Stage IV HER2-positive metastatic breast cancer, including those with asymptomatic or stable (treated or untreated) CNS metastases. In this multinational, randomized, active-controlled, Phase III study, 621 patients (N = 621) with metastatic HER2-positive breast cancer who received two or more prior anti-HER2 based regimens in the metastatic setting were randomly assigned in a 1:1 to receive NERLYNX® 240 mg given orally once daily on days 1-21 along with XELODA® 750 mg/m2 given orally twice daily on days 1-14 for each 21-day cycle (N=307) or TYKERB® 1250 mg given orally once daily on days 1-21 along with XELODA® 1000 mg/m2 given orally twice daily on days 1-14 for each 21-day cycle (N=314). Approximately 85% of patients had visceral metastases, and about 30% had received at least three anti-HER2 therapies. Patients in the NERLYNX® group also received antidiarrheal prophylaxis with Loperamide. Patients were treated until disease progression or unacceptable toxicity. The Co-Primary endpoints were Progression Free Survival (PFS) and Overall Survival (OS). Secondary endpoints included Objective Response Rate (ORR) and Duration of Response, Clinical Benefit Rate (CBR), time to intervention for symptomatic metastatic Central Nervous System (CNS) disease and Safety.
At a median follow up of 29.9 months, treatment with NERLYNX® with XELODA® significantly improved the median PFS, compared to those receiving TYKERB® with XELODA® (HR=0.76; P=0.006). This represented a 24% reduction in the risk of disease progression or death for those receiving a combination of NERLYNX® and XELODA®. The PFS rate at 12 months was 29% versus 15% respectively. The median OS was 21 months for patients receiving NERLYNX® and XELODA® compared to 18.7 months for those receiving TYKERB® and XELODA® (HR=0.88; P=0.20) and this was not statistically significant. The ORR was numerically higher with NERLYNX® and XELODA® combination in patients with measurable disease (32.8% versus 26.7%), and there was a statistically significant improvement in the Clinical Benefit Rate (45% versus 36%; P=0.03). The median Duration of Response was 8.5 versus 5.6 months respectively (HR=0.50; P=0.0004), favoring the NERLYNX® combination. The time to intervention for symptomatic CNS disease was significantly delayed with NERLYNX® combination versus TYKERB® combination, with an overall cumulative incidence of 22.8% versus 29.2% respectively (P= 0.043). The most common toxicities of any grade in the study population were diarrhea, nausea, palmar-plantar erythrodysesthesia syndrome, and vomiting. Treatment related toxicities were similar between arms, but there was a higher rate of Grade 3 diarrhea with the NERLYNX® combination (24% versus 13% respectively).
It was concluded from this study that a combination of NERLYNX® and XELODA® significantly improved Progression Free Survival, with a trend towards improved Overall Survival, and also resulted in a delayed time to intervention for symptomatic CNS disease, among patients with heavily pretreated advanced HER2-positive breast cancer. This is the first study to demonstrate superiority of one HER2-directed Tyrosine Kinase Inhibitor over another, in HER2-positive metastatic breast cancer.
Neratinib Plus Capecitabine Versus Lapatinib Plus Capecitabine in HER2-Positive Metastatic Breast Cancer Previously Treated With 2 or More HER2-Directed Regimens: Phase III NALA Trial. Saura C, Oliveira M, Y Feng Y-H, et al. for the NALA Investigators. J Clin Oncol. 2020;38:3138-3149.
DCIS and Risk of Death from Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease largely due to metastatic recurrence. Carcinoma in situ of the breast also known as Ductal Carcinoma In Situ (DCIS) is defined as a malignant proliferation of ductal epithelial cells that are confined to the milk ducts without invasion of the basement membrane, and is a precursor lesion to invasive carcinoma. DCIS accounts for approximately 25% of all newly diagnosed breast cancers. Patients with small, screening-detected lesions, are often treated with breast-conserving surgery (to prevent the development of invasive breast cancer), followed by adjuvant radiation and hormonal therapy, although neither of the latter two interventions have been shown to improve survival outcomes. As such, a significant number of patients are over treated. DCIS in itself is not life-threatening but can potentially progress to invasive breast cancer. The two important goals of DCIS treatment therefore are, to prevent invasive ipsilateral cancer recurrence and to prevent death from breast cancer. There remains a large unmet need, to distinguish relatively benign DCIS from DCIS that will develop into invasive breast cancer.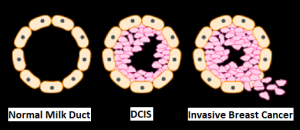
In a previously published meta-analysis (Cancer Epidemiol Biomarkers Prev. 2019;28:835-845), researchers identified six prognostic factors that were statistically significant and were associated with a 36% to 84% increase in the relative risk of recurrence of invasive disease after a DCIS diagnosis. These six factors included-
1) African American race (43% higher risk)
2) Premenopausal status (59% higher risk)bre
3) Detection by palpation (84% higher risk)
4) Positive margins (63% higher risk)
5) High histologic grade (36% higher risk)
6) High p16 expression (51% higher risk).
This present large cohort study was conducted to determine the risk of death from breast cancer, following diagnosis and treatment of DCIS, compared with the mortality risk among cancer-free women, in the general population. This study included a total of 144,524 women diagnosed with first primary DCIS between 1995 and 2014, from the Surveillance, Epidemiology and End Results (SEER) registries database. Patients with DCIS with microinvasion, Lobular Carcinoma In Situ (LCIS), nonepithelial histological presentations, Paget disease of the nipple, diffuse DCIS, unknown laterality, no surgical intervention on the primary tumor, DCIS diagnosis in women younger than 25 years or aged 80 years or older, were all excluded. Patients with DCIS underwent surgical treatment, and approximately half of these patients also received radiotherapy. These patients were followed from the date of DCIS diagnosis until death from breast cancer, or date of last follow up. These patients were compared with women in the general population without a diagnosis of breast cancer (control group). The mean age at diagnosis was 57.4 years. The Primary outcome was death from breast cancer. Standardized Mortality Ratios (SMR) were estimated by comparing deaths from breast cancer among women diagnosed with DCIS, with expected deaths from breast cancer among women in the general population who did not have cancer.
At a mean follow up period of 9.2 years, the incidence of ipsilateral invasive recurrence events was 3.1%, resulting in a 20-year actuarial risk of 13.9%. There was a 3.8% incidence of contralateral invasive breast cancer events during this follow up period, resulting in a 20-year actuarial risk of 11.3%. The 20-year actuarial risk of breast cancer death among women with DCIS was 3.3%.
The Standardized Mortality Ratio (SMR) for death from breast cancer given a diagnosis of DCIS was 3.36, but varied based on age and race. The SMR for women younger than 40 years was much higher at 11.95, whereas the SMR for women aged 40 to 49 years was 4.15. The SMR for White women was 3.03, for Black women was 7.56, and for East Asian women was 1.89. The SMR for Black women diagnosed with DCIS before age 50 years was 12.10, and the SMR for White women diagnosed with DCIS before age 50 years was 4.21, suggesting that Black women did worse than White woman.
All women with DCIS underwent surgical treatment, and 47.1% also received radiotherapy. Among those patients who were not treated with radiotherapy, the SMR was 4.12, for those treated with unilateral mastectomy and 4.14 for those treated with bilateral mastectomies. Among women who underwent lumpectomy, the SMR was 2.81 for women treated with radiotherapy and 3.42 for those who underwent surgical treatment alone. There were 1540 women who died of breast cancer in the cohort, of whom 45.7% experienced an ipsilateral invasive recurrence or contralateral invasive breast cancer in the interval between DCIS and death from breast cancer. Among the patients who died, 27.8% were known to have undergone a mastectomy.
The annual mortality rate from breast cancer over the entire period of follow up was, 0.12% per year. The mortality rate increased for the first 10 years of the follow-up period and remained constant through years 15 thru 20. The cumulative 20-year risk of breast cancer-specific mortality following DCIS was 3.3% overall, but for Black women diagnosed before age 50 years, the 20-year risk of breast cancer-specific mortality was 8.1%. It has been postulated that the highest risk for recurrence among women who underwent mastectomy may be related to them having more extensive disease with close margins or may have genetic mutations that increase the likelihood of recurrence. Further, patients with DCIS undergoing bilateral mastectomies generally are not treated with endocrine therapy.
It was concluded from this cohort study that women with DCIS had a 3-fold increased risk of death from breast cancer after surgical treatment. The Standardized Mortality Ratio was lower among women who received lumpectomy plus radiation compared with women who received lumpectomy alone. The rate of breast cancer death was nearly 12-fold higher among women diagnosed with DCIS before age 40 years and 7-fold higher in Black women diagnosed with DCIS, compared with the general population.
Association of a Diagnosis of Ductal Carcinoma In Situ With Death From Breast Cancer. Giannakeas V, Sopik V and Narod SA. JAMA Netw Open. 2020;3(9):e2017124. doi:10.1001/jamanetworkopen.2020.17124
Late Breaking Abstract – ESMO 2020. VERZENIO® Plus Endocrine Therapy Improves Disease Free Survival in Early Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women 12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease largely due to metastatic recurrence. About 70% of breast tumors express Estrogen Receptors and/or Progesterone Receptors, and Hormone Receptor (HR)-positive/HER2-negative breast cancer is the most frequently diagnosed molecular subtype. Majority of these patients are diagnosed with early stage disease and are often cured with a combination of surgery, radiotherapy, chemotherapy, and hormone therapy. However approximately 20% of patients will experience local recurrence or distant relapse during the first 10 years of treatment. This may be more relevant for those with high risk disease, among whom the risk of recurrence is even greater during the first 2 years while on adjuvant endocrine therapy, due to primary endocrine resistance. More than 75% of the early recurrences are seen at distant sites.
Cyclin Dependent Kinases (CDK) play a very important role to facilitate orderly and controlled progression of the cell cycle. Genetic alterations in these kinases and their regulatory proteins have been implicated in various malignancies. CDK 4 and 6 phosphorylate RetinoBlastoma protein (RB), and initiate transition from the G1 phase to the S phase of the cell cycle. RetinoBlastoma protein has antiproliferative and tumor-suppressor activity and phosphorylation of RB protein nullifies its beneficial activities. CDK4 and CDK6 are activated in hormone receptor positive breast cancer, promoting breast cancer cell proliferation. Further, there is evidence to suggest that endocrine resistant breast cancer cell lines depend on CDK4 for cell proliferation. The understanding of the role of Cyclin Dependent Kinases in the cell cycle, has paved the way for the development of CDK inhibitors.
VERZENIO® (Abemaciclib) is an oral, selective inhibitor of CDK4 and CDK6 kinase activity, and prevents the phosphorylation and subsequent inactivation of the Rb tumor suppressor protein, thereby inducing G1 cell cycle arrest and inhibition of cell proliferation. VERZENIO® is structurally distinct from other CDK 4 and 6 inhibitors (such as Ribociclib and Palbociclib) and is 14 times more potent against cyclin D1/CDK 4 and cyclin D3/CDK 6, in enzymatic assays, but potentially less toxic than earlier pan-CDK inhibitors. At higher doses, only VERZENIO® causes significant cancer cell death, compared with other CDK4/6 inhibitors, suggesting that this drug may be affecting proteins, other than CDK4/6. Additionally, preclinical studies have demonstrated that VERZENIO® may have additional therapeutic benefits for a subset of tumors that are unresponsive to treatment or have grown resistant to other CDK4/6 inhibitors. It has also been shown to cross the blood-brain barrier.
VERZENIO® is presently approved by the FDA as monotherapy as well as in combination with endocrine therapy for patients with HR-positive, HER2- negative advanced breast cancer. The addition of VERZENIO® to FASLODEX® resulted in a statistically significant improvement in Overall Survival among patients with HR-positive, HER2-negative advanced breast cancer, who had progressed on prior endocrine therapy. The goal of monarchE was to evaluate the additional benefit of adding a CDK4/6 inhibitor to endocrine therapy in the adjuvant setting, for patients with HR-positive, HER2-negative early breast cancer.
The international monarchE trial, is an open-label, randomized, Phase III study, which included 5637 patients, who were pre- and postmenopausal, with HR-positive, HER2-negative early breast cancer, and with clinical and/or pathologic risk factors that rendered them at high risk for relapse. The researchers defined high risk as the presence of four or more positive axillary lymph nodes, or 1-3 three positive axillary lymph nodes, with either a tumor size of 5 cm or more, histologic Grade 3, or centrally tested high proliferation rate (Ki-67 of 20% or more). Following completion of primary therapy which included both adjuvant and neoadjuvant chemotherapy and radiotherapy, patients were randomly assigned (1:1) to VERZENIO® 150 mg orally twice daily for 2 years plus 5 to 10 years of physicians choice of endocrine therapy as clinically indicated (N=2808), or endocrine therapy alone (N=2829). The median patient age was 51 years, about 43% of the patients were premenopausal, and 95% of patients had prior chemotherapy. Approximately 60% of patients had 4 or more positive lymph nodes. The Primary endpoint was Invasive Disease Free Survival (IDFS), and Secondary end points included distant Relapse Free Survival, Overall Survival, and safety. The authors in this publication reported the first results, following a preplanned interim analysis.
The addition of VERZENIO® to endocrine therapy resulted in an IDFS of 92.2% at 2 years compared with 88.7% with endocrine therapy alone, and this was statistically significant (HR=0.75; P=0.01). This suggested a 25% reduction in the risk of developing an IDFS event, relative to endocrine therapy alone, and a 3.5% absolute improvement in 2-year IDFS rates. VERZENIO® plus endocrine therapy combination also reduced the risk of metastatic recurrence especially in bone and liver (distant recurrences or Distant Relapse Free Survival) by a clinically meaningful 28% compared to endocrine therapy alone. This clinical benefit was observed in all prespecified subgroups, and among the 43% of patients who were premenopausal at diagnosis, there was a significant 37% reduction in the risk of recurrence compared to endocrine therapy alone. The safety was consistent with the known profile of VERZENIO® and included diarrhea, neutropenia, and fatigue. Diarrhea was well managed with antidiarrheal medications and dose adjustments.
It was concluded that VERZENIO® when combined with endocrine therapy demonstrated a significant improvement in Invasive Disease Free Survival, compared to endocrine therapy alone, in patients with high risk HR-positive, HER2-negative early breast cancer. The researchers also plan to look at genomic signatures in the tissue and plasma samples of enrolled patients and response to VERZENIO®.
Abemaciclib Combined With Endocrine Therapy for the Adjuvant Treatment of HR+, HER2−, Node-Positive, High-Risk, Early Breast Cancer (monarchE). Johnston SRD, Harbeck N, Hegg R, et al. DOI: 10.1200/JCO.20.02514 Journal of Clinical Oncology – published online before print September 20, 2020
Novel Ultrasensitive Liquid Biopsy Detects Minimal Residual Disease in Early Stage Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women 12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease largely due to metastatic recurrence. Recurrent disease can occur early, but majority of patients with hormone receptor-positive breast cancer may develop recurrent disease decades, following their initial diagnosis. Once a diagnosis of metastatic breast cancer is established, it is generally incurable.
Systemic recurrence likely arises from micrometastatic disease present at initial diagnosis, which is undetectable by imaging or conventional blood tests. Adjuvant systemic therapy is recommended to eradicate micrometastatic disease and reduce the risk of cancer recurrence. However, current clinical tools are not accurate in identifying which patients would benefit from adjuvant systemic therapy and further are unable to, in real-time, predict whether the recommended therapies have achieved their therapeutic objective. Therefore, more sensitive techniques to detect micrometastatic disease are needed, so that patients receive the most appropriate and optimal therapy, with improved outcomes.
Recently published studies have shown that detection of circulating tumor DNA (ctDNA) in the peripheral blood may identify patients at risk of relapse following definitive therapy using digital droplet Polymerase Chain Reaction (ddPCR) assays. ctDNA refers to DNA fragments that are shed into the bloodstream by cancer cells after apoptosis or necrosis. The clinical sensitivity of this technique however is limited at the early postoperative time points, at which treatment decisions are usually made, and the lead time prior to clinical manifestation of overt metastatic disease has been relatively short. This is because presently available techniques track one or few mutations and are unable to detect MRD when the fraction of cancerous cell free DNA (cfDNA) in the bloodstream is low.
The authors developed an ultrasensitive blood test for tracking hundreds of patient-specific mutations, to detect Minimal Residual Disease (MRD), with a 1,000-fold lower error rate than conventional sequencing, to identify patients who might benefit from additional systemic treatment or de-escalation of therapy. The authors performed Whole-Exome Sequencing (WES) to define several hundred mutations from each patient’s tumor, and to limit potential errors, selected somatic SNVs (Single Nucleotide Variants) to track, using duplex sequencing in cfDNA and employing strict criteria. The detection of 2 or more mutations in a cfDNA sample was considered MRD-positive and any mutations found in a patient’s own genomic DNA was excluded.
For this study, the authors identified 142 patients who had been treated for Stage 0-III breast cancer with curative intent surgery, had postoperative blood and plasma samples available. Overall, 92% of patients received either neoadjuvant, or adjuvant chemotherapy, 76% received adjuvant endocrine therapy and 73% received adjuvant radiation treatment. Approximately 2% of patients had Stage 0 disease, 23% had Stage I, 48% had Stage II, and 27% had Stage III breast cancer at diagnosis. The MRD levels were tracked post-op (median 3.5 months) and 1 year out (median 14.2 months). The patients were monitored for distant recurrences for up to 13 years. A median of 57 mutations were targeted in each patient, identified via Whole-Exome Sequencing of primary tumor tissue and genomic DNA from whole blood. About 78% of patients had post-op samples available, while 86% had 1-year samples. The Primary objective of this study was to determine the predictive power of MRD testing and associated lead time to recurrence, in patients treated for early-stage breast cancer.
The median lead time (the time from a positive test to diagnosis of metastatic disease) between the first MRD-positive result and disease recurrence was 18.9 months in the patients with the most mutations tracked. This is significantly longer than what has been seen in prior studies. Distant disease recurrence was shown to be more likely if MRD was detected at the 1-year mark (HR=20.8; P<0.0001) compared with the post-op setting. Among these patients, the positive and negative predictive values for distant recurrence, was 0.70 and 0.77, respectively. Overall, the clinical sensitivities were 81% in patients with newly diagnosed metastatic breast cancer, 23% in the post-op setting, and 19% at the one year in early stage disease, and highest among patients with the most tumor mutations available to track. The authors noted that their testing methodology was 100-fold more sensitive than ddPCR, when tracking 488 mutations.
It was concluded that the ultrasensitive blood test developed by investigators for Minimal Residual Disease (MRD) could identify survivors who might benefit from additional systemic treatment versus de-escalation. MRD detection was strongly associated with distant recurrence and provided significant lead time to recurrence, enabling early therapeutic intervention in patients who may otherwise develop metastatic recurrence. The authors recommended that future blood-based Whole-Genome Sequencing assays should aim for extra sensitivity, to identify enough mutations to track in all patients.
Sensitive Detection of Minimal Residual Disease in Patients Treated for Early-Stage Breast Cancer. Parsons HA, Rhoades J, Reed SC, et al. Clin Can Res. DOI: 10.1158/1078-0432.CCR-19-3005. Published June 2020.
Favorable Outcomes with KADCYLA® in HER2+ Breast Cancer Irrespective of Mutational Status
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (13%) will develop invasive breast cancer during their lifetime. Approximately 276,480 new cases of invasive female breast cancer will be diagnosed in 2020 and about 42,170 women will die of the disease. Approximately 15-20% of invasive breast cancers overexpress HER2/neu oncogene, which is a negative predictor of outcomes without systemic therapy. HERCEPTIN® (Trastuzumab) is a humanized monoclonal antibody targeting HER2, and adjuvant and neoadjuvant chemotherapy given along with HERCEPTIN® reduces the risk of disease recurrence and death, among patients with HER2-positive, early stage as well as advanced metastatic breast cancer. Since the approval of HERCEPTIN®, several other HER2-targeted therapies have become available. The duration of adjuvant HERCEPTIN® therapy has been 12 months and this length of treatment was empirically adopted from the pivotal registration trials.
KADCYLA® is an Antibody-Drug Conjugate (ADC) comprised of the antibody HERCEPTIN® and the chemotherapy agent Emtansine, linked together. Upon binding to the HER2 receptor, it not only inhibits the HER2 signaling pathways but also delivers a chemotherapy agent Emtansine, a microtubule inhibitor, directly inside the tumor cells. This agent is internalized by lysosomes and destroys the HER2-positive tumor cells upon intracellular release. It is well established that patients with HER2-positive early breast cancer following HERCEPTIN® based neoadjuvant therapies have a pathological Complete Response (pCR) rate of 40-60%. Those without a pCR tend to have significantly less favorable outcomes. These patients irrespective of pathological response status complete their standard adjuvant therapy which includes 12 months of HER2-targeted therapy. KATHERINE trial was conducted to address an unmet need, and evaluate the benefit of switching from standard HER2-directed therapy to single-agent KADCYLA®, after neoadjuvant chemotherapy, in patients with residual invasive cancer at surgery.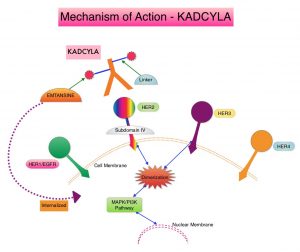
The KATHERINE trial is an open-label, Phase III global study, which compared KADCYLA® with HERCEPTIN®, as an adjuvant treatment for patients with HER2-positive early breast cancer, who had residual invasive disease following neoadjuvant chemotherapy and HERCEPTIN®. This study included 1,486 patients with HER2-positive early stage breast cancer, who were found to have residual invasive disease in the breast or axillary lymph nodes at surgery, following at least six cycles (16 weeks) of neoadjuvant chemotherapy with a Taxane (with or without Anthracycline) and HERCEPTIN®. Within 12 weeks of surgery, patients (N=1486) were randomly assigned in a 1:1 ratio to KADCYLA® 3.6 mg/kg IV every 3 weeks or HERCEPTIN® 6 mg/kg IV every 3 weeks, for 14 cycles (743 patients in each group). Both treatment groups were well balanced and Hormone Receptor positive disease was present in 72% of the patients. The Primary end point was invasive Disease Free Survival (iDFS-defined as freedom from ipsilateral invasive breast tumor recurrence, ipsilateral locoregional invasive breast cancer recurrence, contralateral invasive breast cancer, distant recurrence, or death from any cause). At the prespecified interim analysis, invasive disease occurred in 12.2% of patients who received KADCYLA® and 22.2% of patients who received HERCEPTIN®. The estimated percentage of patients who were free of invasive disease at 3 years was 88.3% in the KADCYLA® group and 77.0% in the HERCEPTIN® group, which translated to an absolute improvement of 11.3%. Invasive Disease Free Survival (iDFS), which was the Primary end point of the study, was significantly higher in the KADCYLA® group than in the HERCEPTIN® group (HR=0.50; P<0.001).This suggested that KADCYLA® reduced the risk of developing an invasive breast cancer recurrence or death by 50%.
The authors in this publication reported the exploratory analyses of the relationship between iDFS, and biomarkers potentially related to response. The authors focused on pathways that have been implicated in resistance to HER2 treatment such as pathways associated with PIK3CA mutations, as well as HER2 and PD-L1 expression in the post-neoadjuvant residual surgical samples.
In the first part of this biomarker analysis, a total of 1,363 available post-neoadjuvant surgery samples were analyzed through DNA sequencing for PIK3CA mutations. In the second part of this analysis, mRNA expression through RNA sequencing was determined on 1,059 tissue samples of which 244 were pre-neoadjuvant samples and 815 were post-neoadjuvant surgical samples. Because the post-neoadjuvant surgical samples were representative of the entire Intent-To-Treat (ITT) patient population, biomarker analysis for markers such as HER2, PD-L1, CD8, and predefined immune signatures including 3-gene, 5-gene, Teffector, chemokine signaling, and checkpoint inhibitor signatures, were performed by using post-neoadjuvant surgical samples.
The authors noted that in the ITT population (N=743), PIK3CA mutation status had no impact on outcomes when treated with KADCYLA®. Among those patients with mutated tumors who received KADCYLA® and HERCEPTIN®, the iDFS rates were 88.9% versus 77.9%, respectively (HR=0.54) and among those with non-mutated tumors the Invasive Disease Free Survival rates were 88.3% versus 77.0%, respectively (HR=0.48). There was no prognostic impact of PIK3CA mutations in this cohort of patients and the 3 year iDFS rates were almost identical between the mutated and non-mutated tumors.
The authors next looked at HER2 gene expression in the post-neoadjuvant surgical samples and noted that patients who had a tumors with high HER2 expression in the post-neoadjuvant residual surgical samples, and received subsequent treatment with HERCEPTIN®, had the worst outcomes with worse iDFS. This detrimental effect was not seen in the KADCYLA® group, suggesting that residual tumors that have a high HER2 expression in this setting are resistant to HERCEPTIN® but not to KADCYLA®.
When patients were evaluated based on their tumor PD-L1 expression, low PD-L1 expression in post-neoadjuvant residual tumors was associated with a worse outcome for those who received treatment with HERCEPTIN®, whereas treatment with KADCYLA® did not impact outcomes. These findings suggested that PD-L1 may be involved in some resistance mechanisms.
It was concluded that in the KATHERINE trial biomarker analysis, PIK3CA mutation status did not influence outcomes in either treatment groups. However, in the post-neoadjuvant HERCEPTIN® group, high HER2 expression and low PD-L1 expression was associated with less favorable outcomes. The benefit with KADCYLA® in this patient population was independent of all biomarkers assessed.
Biomarker data from KATHERINE: A phase III study of adjuvant trastuzumab emtansine (T-DM1) versus trastuzumab (H) in patients with residual invasive disease after neoadjuvant therapy for HER2-positive breast cancer. Denkert C, Lambertini C, Fasching PA, et al. J Clin Oncol. 2020;38(suppl 15):502. doi: 10.1200/JCO.2020.38.15_suppl.502
First Line KEYTRUDA® plus Chemotherapy Significantly Improves PFS in PD-L1-High Triple Negative Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (13%) will develop invasive breast cancer during their lifetime. Approximately 276,480 new cases of invasive female breast cancer will be diagnosed in 2020 and about 42,170 women will die of the disease. Triple Negative Breast Cancer (TNBC) is a heterogeneous, molecularly diverse group of breast cancers and are ER (Estrogen Receptor), PR (Progesterone Receptor) and HER2 (Human Epidermal Growth Factor Receptor-2) negative. TNBC accounts for 15-20% of invasive breast cancers, with a higher incidence noted in young patients and African American females. It is usually aggressive, and tumors tend to be high grade, and patients with TNBC are at a higher risk of both local and distant recurrence and often develop visceral metastases. Those with metastatic disease have one of the worst prognoses of all cancers with a median Overall Survival of 13 months. The majority of patients with TNBC who develop metastatic disease do so within the first 3 years after diagnosis, whereas those without recurrence during this period of time have survival rates similar to those with ER-positive breast cancers. The lack of known recurrent oncogenic drivers in patients with metastatic TNBC, presents a major therapeutic challenge. Overall survival among patients with pretreated metastatic TNBC has not changed over the past 2 decades and standard chemotherapy is associated with low response rates of 10-15% and a Progression Free Survival (PFS) of only 2-3 months.
KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2. It thereby reverses the PD-1 pathway-mediated inhibition of the immune response and unleashes the tumor-specific effector T cells. The rationale for combining chemotherapy with immunotherapy is that cytotoxic chemotherapy releases tumor-specific antigens, and immune checkpoint inhibitors such as KEYTRUDA® when given along with chemotherapy can enhance endogenous anticancer immunity.
Single agent KEYTRUDA® in metastatic TNBC demonstrated durable antitumor activity in several studies, with Objective Response Rates (ORRs) ranging from 10% to 21% and improved clinical responses in patients with higher PD-L1 expression. When given along with chemotherapy as a neoadjuvant treatment for patients with high-risk, early-stage TNBC, KEYTRUDA® combination achieved Pathological Complete Response rate of 65%, regardless of PD-L1 expression. Based on this data, KEYTRUDA® in combination with chemotherapy was studied, for first-line treatment of triple-negative metastatic breast cancer.
KEYNOTE-355 is a randomized, double-blind, phase III study, which evaluated the benefit of KEYTRUDA® in combination with one of the three different chemotherapy regimens, nab-Paclitaxel, Paclitaxel, or the non-taxane containing Gemzar/Carboplatin, versus placebo plus one of the three chemotherapy regimens, in patients with previously untreated or locally recurrent inoperable metastatic TNBC. In this study, 847 patients were randomized 2:1 to receive either KEYTRUDA® 200 mg IV on day 1 of each 21-day cycle along with either nab-paclitaxel 100 mg/m2 IV on days 1, 8 and 15 of each 28-day cycle, Paclitaxel 90 mg/m2 IV on days 1, 8 and 15 of each 28-day cycle, or Gemcitabine 1000 mg/m2 IV plus Carboplatin AUC 2 IV on days 1 and 8 of each 21-day cycle (N= 566) or placebo along with one of the three chemotherapy regimens (N= 281). This study was not designed to compare the efficacy of the different chemotherapy regimens. Treatment was continued until disease progression. Patients were stratified by chemotherapy, PD-L1 tumor expression (CPS of 1 or higher versus CPS of less than 1), and prior treatment with the same class of neoadjuvant/adjuvant chemotherapy (yes vs no). The baseline characteristics of treatment groups were well-balanced. The co-Primary end points of the trial were Progression Free Survival (PFS) and Overall Survival (OS) in patients with PD-L1-positive tumors, and in all patients. Secondary end points were Objective Response Rate (ORR), Duration of Response, Disease Control Rate, and safety. The median follow up for patients assigned to receive KEYTRUDA® was 17.5 months and 15.5 months for the placebo group. The authors reported the results from an interim analysis conducted by an Independent Data Monitoring Committee (IDMC).
KEYTRUDA® in combination with chemotherapy, significantly improved PFS in patients with CPS (Combined Positive Score) of 10 or greater. The median PFS was 9.7 months for KEYTRUDA® plus chemotherapy, compared with 5.6 months for placebo plus chemotherapy (HR=0.65, P=0.0012). This represented a 35% reduction in the risk of disease progression. Among patients with CPS of 1 or greater, the median PFS was 7.6 months for KEYTRUDA® plus chemotherapy, compared with 5.6 months for the placebo plus chemotherapy arm (HR= 0.74; P=0.0014). This however based on prespecified statistical criteria, was not considered statistically significant. Among the entire Intention-To-Treat (ITT) population, the median PFS was 7.5 months in the KEYTRUDA® plus chemotherapy group, compared with 5.6 months for chemotherapy plus placebo group (HR=0.82). Formal statistical significance was not tested in the ITT population. Overall Survival data are pending. Adverse Events (AEs) were similar in both treatment groups, although immune-related AEs occurred at a higher incidence in the KEYTRUDA® arm.
It was concluded that KEYTRUDA® in combination with several chemotherapy regimens, showed a statistically significant and clinically meaningful improvement in PFS, compared with chemotherapy alone, in patients with previously untreated locally recurrent, inoperable or metastatic TNBC, whose tumors expressed PD-L1 with a Combined Positive Score (CPS) of 10 or more. This data may be particularly relevant for patients who may have received a taxane in the adjuvant setting within a year, and could be more appropriately treated with a non-taxane regimen, in combination with KEYTRUDA®.
KEYNOTE-355: Randomized, double-blind, phase III study of pembrolizumab + chemotherapy versus placebo + chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer. Cortes J, Cescon DW, Rugo HS. et al. J Clin Oncol 38: 2020 (suppl; abstr 1000)
PIQRAY® Effective after Progression on CDK Inhibition in Advanced Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (13%) will develop invasive breast cancer during their lifetime. Approximately 276,480 new cases of invasive female breast cancer will be diagnosed in 2020 and about 42,170 women will die of the disease. Approximately 6% of newly diagnosed breast cancer patients present with Stage IV disease and about half of patients with primary breast cancer will progress later to the metastatic stage. About 70% of breast tumors express Estrogen Receptors and/or Progesterone Receptors and Hormone Receptor (HR)-positive/HER2-negative breast cancer is the most frequently diagnosed molecular subtype. Most of these patients with advanced disease in the current era are treated with a combination of CDK4/6 inhibitor and endocrine therapy (often an oral Aromatase Inhibitor), based on survival data. However, resistance to these regimens typically develops in a majority of the patients.
The PhosphoInositide 3-Kinase (PI3K) pathway is an intracellular signaling pathway important in the regulation of cancer cell proliferation and metastasis. PI3K is a lipid kinase and has four distinct isoforms – alpha, beta, gamma and delta, which play a unique role in the survival of different tumor types and establishment of supportive tumor microenvironments. The alpha and beta isoforms are expressed in a wide variety of tissues whereas the gamma and delta isoforms are primarily expressed in hematopoietic cells such as B and T cells. The PI3K alpha isoform is particularly important in breast cancer and plays an important role in tumorigenesis, supporting tumor angiogenesis and stromal interactions, making this a viable target. PIK3CA is an oncogene that codes for the alpha isoform of PI3K, (PI3Kα), more specifically for the alpha isoform of p110. The PI3k pathway is the most frequently altered pathway in human cancers including breast cancer, and has been implicated in disease progression in a significant number of patients with breast cancer. Activation of the PI3K pathway in breast cancer has been associated with resistance to endocrine therapy and disease progression. Approximately 40% of patients with Hormone Receptor positive (HR+), HER2-negative breast cancers, harbor activating mutations in the PIK3CA isoform of PI3K, which is the most common mutation in HR+ breast cancer. Patients with advanced breast cancer harboring PIK3CA mutations typically have a poor prognosis. This provides a strong rationale for targeting the PI3K pathway in breast cancer.
PIQRAY® is an oral, alpha-specific PI3K inhibitor that specifically inhibits PIK3 in the PI3K/AKT kinase signaling pathway. Further, it was shown in preclinical studies that cancer cells with PIK3CA mutations are more sensitive to PIQRAY® than those without the mutation, across a broad range of tumor types. In the SOLAR-1 Phase III trial, there was a 35% improvement in Progression Free Survival (PFS) in patients randomized to PIQRAY® plus FASLODEX®, compared to the placebo plus FASLODEX® group, among postmenopausal patients with PIK3CA-mutated, HR+/HER2- negative, advanced breast cancer, who had progressed on or following prior Aromatase Inhibitor (AI) treatment with or without a CDK 4/6 inhibitor. However in this study, only 6% had received prior CDK4/6 inhibitor therapy and there is presently limited data available, to inform treatment decisions in patients who progress on AI and CDK 4/6 inhibitor combination.
BYLieve is an ongoing, prospective, open-label, Phase II, non-comparative trial, which evaluated the benefit of PIQRAY® in combination with endocrine therapy in patients with HR+, HER-negative, PIK3CA-mutated, advanced breast cancer, who progressed on or after a prior therapy including CDK inhibitor. This study included 3 patient cohorts– Cohort A included patients who received a CDK4/6 inhibitor plus an AI as immediate prior therapy, Cohort B included patients who received a CDK4/6 inhibitor plus FASLODEX® (Fulvestrant) as immediate prior therapy, and Cohort C included patients who progressed on/after an AI and received chemotherapy or endocrine therapy as immediate prior treatment.
The authors in this publication shared findings from Cohort A group of patients, who had received CDK4/6 inhibitor plus an AI as their immediate prior therapy. Cohort A enrolled 127 patients of whom 121 patients had centrally confirmed PIK3CA mutation. Patients in Cohort A received PIQRAY® 300 mg orally once daily along with FASLODEX® 500 mg IM on Day 1 and 15 of cycle 1 followed by Day 1 treatment, of each 28 day cycle thereafter. The median patient age was 58 years. Seventy percent (70%) of patients had received one prior metastatic regimen, none of the patients had received FASLODEX® as a first-line metastatic agent, and 60% of patients had secondary endocrine resistance. The median follow up was 11.7 months. The Primary endpoint was proportion of patients alive without disease progression at 6 months. Secondary end points included Progression Free Survival (PFS), Overall Response Rate (ORR), Overall Survival (OS), and safety.
The Primary endpoint was met and the proportion of patients with confirmed PIK3CA mutation and without disease progression at 6 months was 50.4%. The median PFS was 7.3 months. Among the 121 patients in Cohort A with a confirmed PIK3CA mutation, the response rate, which was all partial responses was 17.4%, and 45.5% achieved stable disease.
Although the BYLieve trial did not have a control group to allow comparing patients in Cohort A to patients receiving other standard therapies, the authors conducted a weighted/matched analysis between the patients in Cohort A of the BYLieve trial and a Real-World similar group of 95 patients with HR+, HER2-negative, PIK3CA-mutated advanced breast cancer, who were treated with standard therapies. The Real-World patient data was obtained from the de-identified clinic-genomic database of Flatiron Health and Foundation Medicine. These 95 patients had received a wide range of regimens, with the most frequent being XELODA® (Capecitabine) monotherapy, FASLODEX® monotherapy, FASLODEX® plus IBRANCE® (Palbociclib), AFINITOR® (Everolimus) plus AROMASIN® (Exemestane), FASLODEX® plus FEMARA® (Letrozole), and IBRANCE® monotherapy.
Unadjusted results showed a median PFS of 7.3 months in BYLieve Cohort A versus 3.6 months in the Real-World cohort. Similar outcomes were noted when data were weighted by odds, propensity score matching, and exact matching.
It was concluded that the BYLieve trial is continuing to show clinically meaningful efficacy with a combination of PIQRAY® and FASLODEX® in HR+, HER2-negative, PIK3CA-mutated advanced breast cancer, post CDK inhibitor treatment, building further on the findings of SOLAR-1 trial. The matched analysis comparing BYLieve with Real-World Data in the post-CDK4/6 inhibitor setting, further supports use of PIQRAY® plus FASLODEX® for this patient group.
Alpelisib (ALP) + fulvestrant (FUL) in patients (pts) with PIK3CA-mutated (mut) hormone receptor-positive (HR+), human epidermal growth factor receptor 2-negative (HER2–) advanced breast cancer (ABC) previously treated with cyclin-dependent kinase 4/6 inhibitor (CDKi) + aromatase inhibitor (AI): BYLieve study results. Rugo HS, Lerebours F, Ciruelos E, et al. J Clin Oncol 38: 2020 (suppl; abstr 1006).