
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 246,660 new cases of invasive breast cancer will be diagnosed in 2016 and 40,450 women will die of the disease. Approximately 75% of patients with breast cancer are hormone receptor positive (Estrogen Receptor/Progesterone Receptor positive) and this is a predictor of response to endocrine therapy. 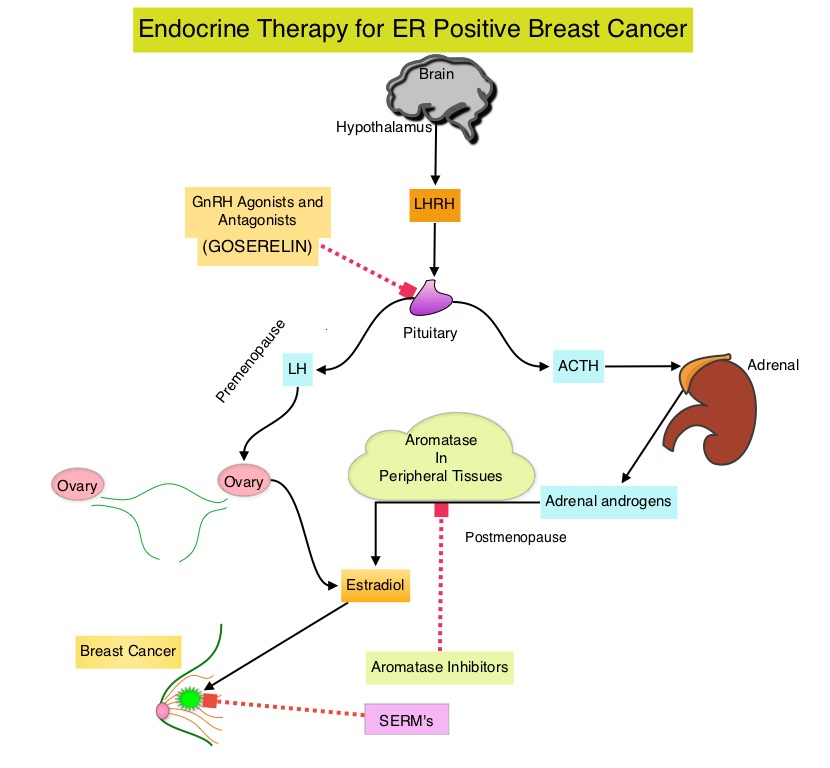 These patients are often treated with anti-estrogen therapy as first line treatment. In premenopausal woman, the ovary is the main source of estrogen production, whereas in postmenopausal women, the primary source of estrogen is the Aromatase enzyme mediated conversion of androstenedione and testosterone to estrone and estradiol, in extragonadal/peripheral tissues. NOLVADEX® (Tamoxifen) is a nonsteroidal Selective Estrogen Receptor Modulator (SERM) and works mainly by binding to the Estrogen Receptor and thus blocks the proliferative actions of estrogen on the mammary tissue. ARIMIDEX® (Anastrozole), FEMARA® (Letrozole) and AROMASIN® (Exemestane) are Aromatase Inhibitors (AIs) that binds to the Aromatase enzyme and inhibit the conversion of androgens to estrogens in the extra-gonadal tissues.
These patients are often treated with anti-estrogen therapy as first line treatment. In premenopausal woman, the ovary is the main source of estrogen production, whereas in postmenopausal women, the primary source of estrogen is the Aromatase enzyme mediated conversion of androstenedione and testosterone to estrone and estradiol, in extragonadal/peripheral tissues. NOLVADEX® (Tamoxifen) is a nonsteroidal Selective Estrogen Receptor Modulator (SERM) and works mainly by binding to the Estrogen Receptor and thus blocks the proliferative actions of estrogen on the mammary tissue. ARIMIDEX® (Anastrozole), FEMARA® (Letrozole) and AROMASIN® (Exemestane) are Aromatase Inhibitors (AIs) that binds to the Aromatase enzyme and inhibit the conversion of androgens to estrogens in the extra-gonadal tissues.
An Update Panel of the ASCO conducted a systematic review of randomized clinical trials investigating ovarian suppression and published this update. This information is an update of the ASCO adjuvant endocrine therapy guideline, regarding the risks and benefits of ovarian suppression in addition to standard adjuvant therapy, in premenopausal women with Estrogen Receptor positive breast cancer. The ASCO Update Panel addressed the following questions with regard to premenopausal women with stage I-III hormone receptor-positive Breast Cancer:
1) Should premenopausal women with ER positive tumors receive adjuvant ovarian suppression in addition to standard adjuvant therapy, and, if so, in which subsets of patients?
2) If ovarian suppression is recommended, should ovarian suppression be administered in combination with Tamoxifen or an Aromatase Inhibitor?
Recommendation 1
1.1 The panel recommends that higher risk patients should receive ovarian suppression in addition to adjuvant endocrine therapy, whereas lower-risk patients should not. (For women with higher risk cancers who receive chemotherapy but remain premenopausal, ovarian suppression added to Tamoxifen reduces the risk of breast cancer recurrence).
1.2 Women with stage II or III Breast Cancers who would ordinarily be advised to receive adjuvant chemotherapy should receive ovarian suppression in addition to endocrine therapy.
1.3 Women with stage I or II breast cancers at higher risk of recurrence, who might consider chemotherapy, may also be offered ovarian suppression in addition to endocrine therapy.
1.4 Women with stage I breast cancers not warranting chemotherapy should receive endocrine therapy but not ovarian suppression.
1.5 Women with node-negative cancers 1 cm or less (T1a, T1b) should receive endocrine therapy but not ovarian suppression.
Qualifying Statements
• The standard duration of ovarian suppression in the included trials was 5 years. The panel therefore supports ovarian suppression for 5 years as there is no comparative data available on alternative durations.
• To date, there is no adequate evidence for assessing the benefit of adjuvant ovarian suppression in women at sufficient risk to warrant chemotherapy compared with 10 years of Tamoxifen.
• There is no current role for ovarian suppression as adjuvant therapy in ER negative breast cancers.
• There are substantial adverse effects related to ovarian suppression. Clinicians and patients should take this into consideration when choosing ovarian suppression.
• The long-term effects of ovarian suppression on breast cancer risk and survival are not yet established.
Recommendation 2
Ovarian suppression may be administered with either Tamoxifen or an Aromatase Inhibitor.
Qualifying Statements
• Tamoxifen and Aromatase Inhibitor therapy differ in their side effect profiles, which may affect patient preferences.
• Clinicians should be alert to the possibility of incomplete ovarian suppression with Gonadotropin-Releasing Hormone agonist therapy and evaluate patients for whom there is concern about residual ovarian function.
Burstein HJ, Lacchetti C, Anderson H, et al: Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: American Society of Clinical Oncology clinical practice guideline update on ovarian suppression. J Clin Oncol 2016;34:1689-1701
