
SUMMARY: The FDA on May 13, 2016 approved LENVIMA® (Lenvatinib) in combination with AFINITOR® (Everolimus), for the treatment of advanced Renal Cell Carcinoma, following one prior anti-angiogenic therapy. LENVIMA® was first approved in 2015 for the treatment of locally recurrent or metastatic, progressive, radioactive iodine-refractory differentiated thyroid cancer. The American Cancer Society estimates that about 62,700 new cases of kidney cancer will be diagnosed in the United States in 2016 and over 14,000 patients will die from this disease.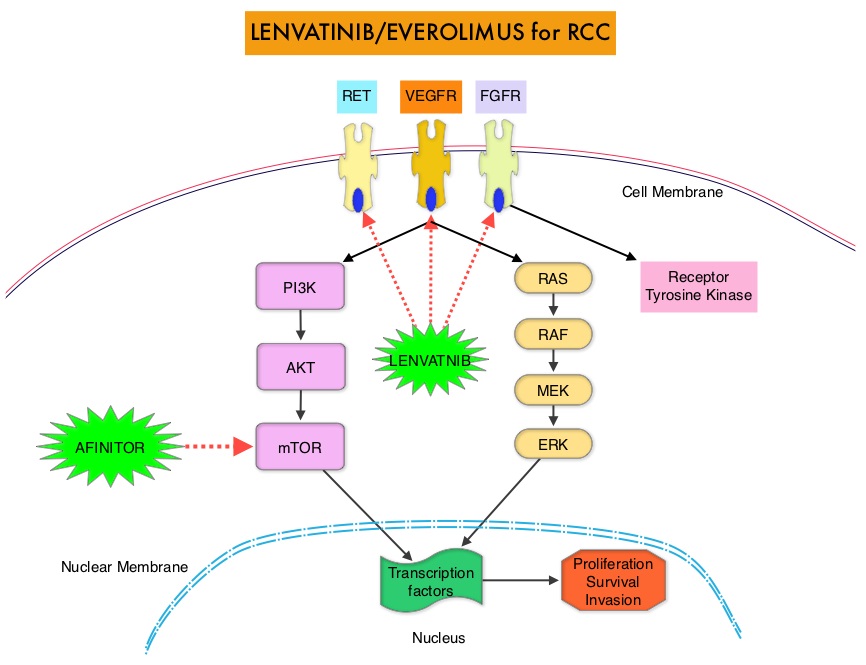
LENVIMA® is an oral multitargeted TKI (Tyrosine Kinase Inhibitor), which targets Vascular Endothelial Growth Factor Receptor (VEGFR)1-3, Fibroblast Growth Factor Receptor (FGFR)1-4, REarranged during Transfection tyrosine kinase receptor (RET), c-KIT, and Platelet Derived Growth Factor Receptor (PDGFR). LENVIMA® differs from other TKIs with anti-angiogenesis properties by its ability to inhibit FGFR-1, thereby blocking the mechanisms of resistance to VEGF/VEGFR inhibitors. In addition, it controls tumor cell growth by inhibiting RET, c-KIT, and PDGFR beta and influences tumor microenvironment by inhibiting by FGFR and PDGFR beta. AFINITOR® (Everolimus) does not inhibit tyrosine kinases, but is a specific inhibitor of mTOR (Mammalian Target of Rapamycin), which is a serine/threonine kinase, normally activated further downstream in the signaling cascade. With the inhibition of mTOR, protein synthesis is inhibited resulting in decreased angiogenesis, cell proliferation and survival as well as decreased levels of HIF-1 alpha.
Metastatic Renal Cell Carcinoma is currently treated with sequential therapy using single agent VEGF or mTOR inhibitors. The current FDA approval was based on a multicenter open-label phase II study in which 153 patients were randomized in a 1:1:1 ratio to receive LENVIMA® plus AFINITOR® (N=51), LENVIMA® monotherapy (N=52), or AFINITOR® monotherapy (N=50). Enrolled patients had advanced or metastatic Renal Cell Carcinoma and had previously received anti-angiogenic therapy. Patients in the combination group received LENVIMA® 18 mg QD along with AFINITOR® 5 mg QD, orally, whereas patients in the single agent groups received either LENVIMA® 24 mg QD or AFINITOR® 10 mg QD. Patients were not allowed to crossover in this study. Using the MSKCC (Memorial Sloan Kettering Cancer Center) risk classification, patients were well balanced between the treatment groups. The primary endpoint was Progression Free Survival. Secondary endpoints included Objective Response Rate (ORR) and Overall Survival (OS).
It was noted that the median PFS in the combination group was 14.6 months compared with 5.5 months in the AFINITOR® alone group (HR=0.37; P=0.0005). This meant a 63% reduction in the risk of disease progression. The median OS with the combination treatment was 25.5 months compared to 15.4 months with AFINTOR® alone (HR=0.67) and this meant a 33% reduction in the risk of death. The ORR with the LENVIMA® and AFINITOR® combination was 37% compared with 6% in the AFINITOR® alone group. The PFS at one year was 31% with the combination treatment versus 14% with single agent AFINITOR® and at 2 years 51% of patients remained alive in the combination treatment group compared with 26% in the single-agent AFINITOR® group. The most common grade 3-4 toxicities in the combination group included diarrhea, fatigue, arthralgia, hypertension and anemia.
The authors concluded that a combination of LENVIMA® and AFINITOR® significantly improves Progression Free Survival, in patients with metastatic Renal Cell Carcinoma, who had progressed on previous VEGF targeted therapy and this combination therapy may change the treatment paradigm for this patient population. Lenvatinib, everolimus, and the combination in patients with metastatic renal cell carcinoma: a randomised, phase 2, open-label, multicentre trial. Motzer RJ, Hutson TE, Glen H, et al. Lancet Oncol. 2015;16:1473-1482.
