
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop breast cancer during their life time. Approximately, 255,180 new cases of breast cancer will be diagnosed in 2017 and 41,070 women will die of the disease. Estrogen Receptor (ER) positive breast cancer cells are driven by estrogens. Approximately 60-65% of breast tumors express Estrogen Receptors and/or Progesterone Receptors and this is a predictor of response to endocrine therapy. These patients are often treated with anti-estrogen therapy which is the cornerstone of their treatment. In premenopausal woman, the ovary is the main source of estrogen production, whereas in postmenopausal women, the primary source of estrogen is the Aromatase enzyme mediated conversion of androstenedione and testosterone to estrone and estradiol, in extragonadal/peripheral tissues. NOLVADEX® (Tamoxifen) is a nonsteroidal Selective Estrogen Receptor Modulator (SERM) and works mainly by binding to the Estrogen Receptor and thus blocks the proliferative actions of estrogen on the mammary tissue. ARIMIDEX® (Anastrozole), FEMARA® (Letrozole) and AROMASIN® (Exemestane) are Aromatase Inhibitors (AIs) that binds to the Aromatase enzyme and inhibit the conversion of androgens to estrogens in the extra-gonadal tissues. FASLODEX® (Fulvestrant) is an estrogen antagonist and like NOLVADEX®, binds to estrogen receptors (ERs) competitively, but unlike NOLVADEX® causes rapid degradation and loss of ER protein (ER downregulator), and is devoid of ER agonist activity.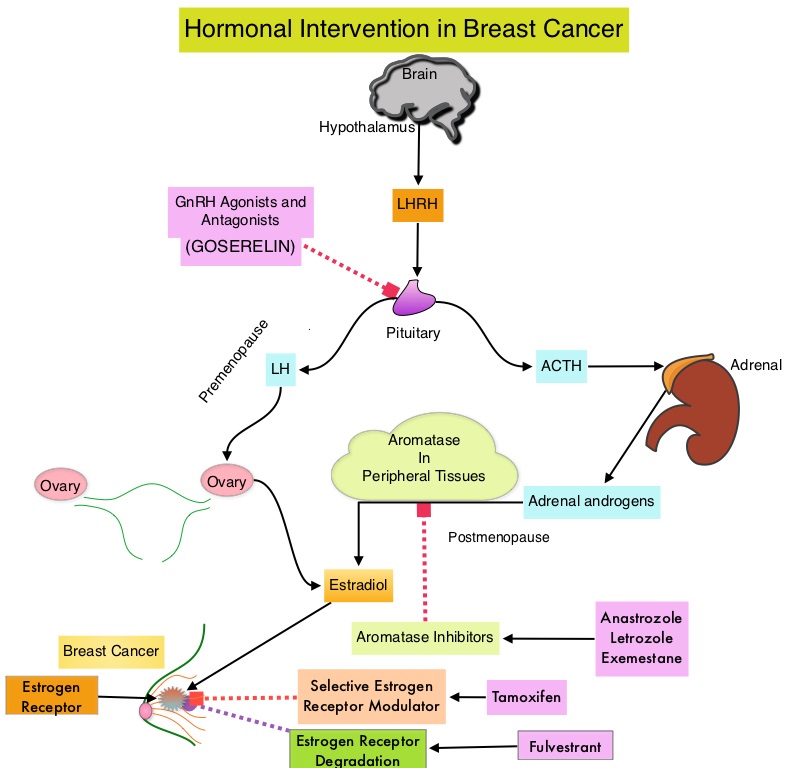
Upon development of metastatic disease, a subgroup of these patients, develop resistance to endocrine therapy. The most common acquired mutation noted in breast tumors as they progress from primary to metastatic setting are the ESR1 mutations. These mutations promote ligand independent estrogen receptor activation and have been shown to promote resistance to estrogen deprivation therapy. It appears that ESR1 mutations are harbored in metastatic ER-positive breast cancers with prior Aromatase Inhibitor (AI) therapy, but not in primary breast cancers, suggesting that ESR1 mutations may be selected by prior therapy with an AI, in advanced breast cancer. In a recently published study (JAMA Oncol.2016;2:1310-1315) ESR1 mutations Y537S and D538G mutations detected in baseline plasma samples from ER positive, HER negative advanced breast cancer patients, was associated with shorter Overall Survival. In this study it was noted that there was a three-fold increase in the prevalence of these mutations in patients who had failed first line hormonal therapy for metastatic disease, compared with those who were initiating first line therapy for advanced breast cancer (33% vs 11%).
Droplet digital Polymerase Chain Reaction (ddPCR) is a highly sensitive and specific technique and can detect ESR1 mutations in the plasma. Retrospective studies have shown that ESR1 mutations detected in plasma cfDNA (cell free DNA) by ddPCR were associated with a lack of response to subsequent AI therapy. The authors in this publication used baseline plasma samples and assessed the impact of ESR1 mutations on sensitivity to standard therapies in two phase III randomized trials, the SoFEA trial and PALOMA-3 trial, which are representative of the current standard of care for ER positive advanced breast cancer.
In the SoFEA trial (Study of Faslodex With or Without Concomitant Arimidex), AROMASIN® (Exemestane), a steroidal AI, was compared with FASLODEX® (Fulvestrant)-containing regimens, in patients with prior sensitivity to nonsteroidal AIs (Letrozole and Anastrozole). In the PALOMA3 trial (Palbociclib Combined With Fulvestrant in Hormone Receptor–Positive HER2-Negative Metastatic Breast Cancer After Endocrine Failure) trial, FASLODEX® plus placebo was compared with FASLODEX® plus IBRANCE® (Palbociclib), in patients with progression after receiving prior endocrine therapy. ESR1 mutations were analyzed by multiplex digital Polymerase Chain Reaction. (Multiplex PCR amplifies several different DNA sequences simultaneously and more information can be obtained from a single test run).
In the SoFEA trial, ESR1 mutations were found in 39.1% of patients of whom 49.1% were polyclonal. Polyclonal ESR1 mutations suggest that biopsy from a single metastatic site would fail to show capture these mutations. Patients with ESR1 mutations on FASLODEX® had improved Progression Free Survival (PFS) compared with AROMASIN® (HR=0.52; P=0.02). Patients with wild-type ESR1 had similar PFS after receiving either treatment (HR=1.07; P=0 .77). Ability to detect these mutations was not impacted by delays in processing of archival plasma. In the PALOMA3 trial, ESR1 mutations were found in the plasma of 25.3% of patients of whom 28.6% were polyclonal ESR1 mutations. The combination of FASLODEX® plus IBRANCE® improved PFS compared with FASLODEX® plus placebo in both ESR1 mutant (HR=0.43; P=0.002) and ESR1 wild-type patients (HR=0.49; P<0.001).
The authors concluded that plasma analysis for ESR1 mutations after progression on prior AI therapy may help direct choice of further endocrine-based therapy. Plasma ESR1 Mutations and the Treatment of Estrogen Receptor–Positive Advanced Breast Cancer. Fribbens C, O’Leary B, Kilburn L, et al. J Clin Oncol. 2016;34:2961-2968
