
SUMMARY: The Center for Disease Control and Prevention (CDC) estimates that approximately 1-2 per 1000 individuals develop Deep Vein Thrombosis/Pulmonary Embolism (PE) each year in the United States, resulting in 60,000 – 100,000 deaths. VTE is the third leading cause of cardiovascular mortality with a mortality rate of up to 25% in those with untreated acute pulmonary embolism. For decades, Unfractionated Heparin (UFH) also known as standard heparin along with Vitamin K antagonist (Warfarin) has been the established standard, for the treatment of Acute Venous ThromboEmbolism. 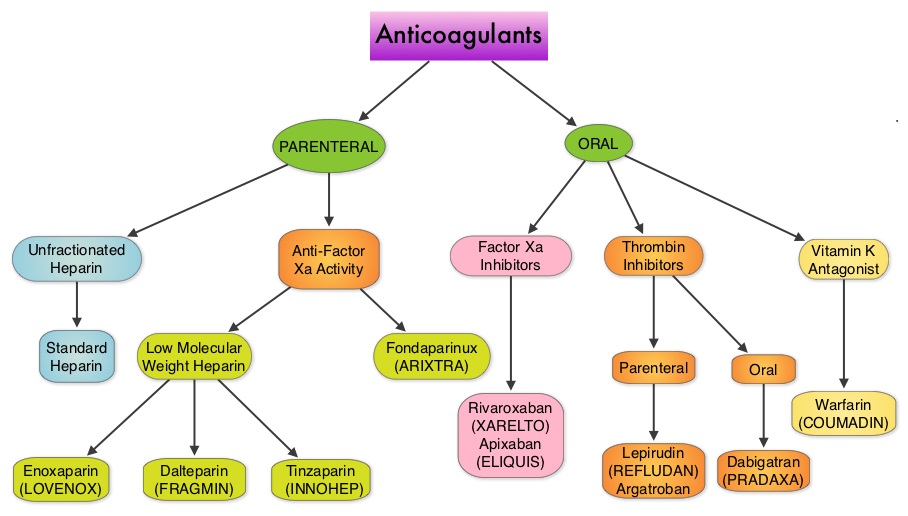 Even though Low Molecular Weight Heparin (LMWH) preparations as well as new oral anticoagulants have been available for the treatment Venous ThromboEmbolism, there has been very little guidance for Health Care Providers on the use of these newer agents. The authors in this analysis compared the efficacy and safety outcomes associated with different anticoagulation regimens for treatment of Venous ThromboEmbolism (VTE). These anticoagulant regimens included Unfractionated Heparin (UFH), Low Molecular Weight Heparin (LMWH) or Fondaparinux in combination with Vitamin K antagonists, LMWH with Dabigatran (PRADAXA®), Rivaroxaban (XARELTO®), Apixaban (ELIQUIS®) or Edoxaban and LMWH alone. This meta analysis included 44,989 patients from 45 randomized trials which reported rates of recurrent VTE and major bleeding in patients with acute VTE. In these Acute Deep Vein Thrombosis and Pulmonary Embolism trials, Rivaroxaban and Apixaban were evaluated without the use of initial LMWH whereas both Dabigatran or Edoxaban were assessed following an initial 5 day treatment with LMWH. This analysis was therefore able to assess clinical and safety outcomes associated with different anticoagulation regimens. The followings findings were noted:
Even though Low Molecular Weight Heparin (LMWH) preparations as well as new oral anticoagulants have been available for the treatment Venous ThromboEmbolism, there has been very little guidance for Health Care Providers on the use of these newer agents. The authors in this analysis compared the efficacy and safety outcomes associated with different anticoagulation regimens for treatment of Venous ThromboEmbolism (VTE). These anticoagulant regimens included Unfractionated Heparin (UFH), Low Molecular Weight Heparin (LMWH) or Fondaparinux in combination with Vitamin K antagonists, LMWH with Dabigatran (PRADAXA®), Rivaroxaban (XARELTO®), Apixaban (ELIQUIS®) or Edoxaban and LMWH alone. This meta analysis included 44,989 patients from 45 randomized trials which reported rates of recurrent VTE and major bleeding in patients with acute VTE. In these Acute Deep Vein Thrombosis and Pulmonary Embolism trials, Rivaroxaban and Apixaban were evaluated without the use of initial LMWH whereas both Dabigatran or Edoxaban were assessed following an initial 5 day treatment with LMWH. This analysis was therefore able to assess clinical and safety outcomes associated with different anticoagulation regimens. The followings findings were noted:
1) Standard Heparin–Vitamin K antagonist combination was associated with an increased risk of recurrent VTE compared with the LMWH–Vitamin K antagonist combination
2) Both new oral anticoagulants and LMWH–vitamin K antagonist combination had similar clinical outcomes. However, the newer oral anticoagulants were associated with a lower risk of major bleeding and this benefit was more pronounced with Rivaroxaban and Apixaban. Compared with LMWH-Dabigatran and LMWH-Edoxaban combinations, Apixaban was associated with a lower risk of bleeding.
This comprehensive analysis lead the authors to conclude that Unfractionated Heparin (Standard Heparin)–Vitamin K antagonist combination is the least effective strategy for the treatment of Acute Venous ThromboEmbolism and Rivaroxaban and Apixaban are associated with the lowest risk for bleeding. Castellucci LA, Cameron C, Le Gal G, et al. JAMA 2014;312:1122-1135
