
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their life time. Approximately, 246,660 new cases of invasive breast cancer were diagnosed in 2016 and 40,450 women will die of the disease. The HER or erbB family of receptors consist of HER1, HER2, HER3 and HER4. Approximately 20-25% of invasive breast cancers overexpress HER2/neu oncogene, which is a negative predictor of outcomes without systemic therapy. HERCEPTIN® (Trastuzumab) is a humanized monoclonal antibody targeting HER2. HERCEPTIN® binds to subdomain IV of the HER2 extracellular domain and blocks the downstream cell signaling pathways (PI3K-AKT pathway) and induces Antibody Dependent Cellular Cytotoxicity (ADCC). HERCEPTIN® in combination with chemotherapy has been proven to significantly improve Progression Free Survival and Overall Survival in patients with advanced breast cancer. Adjuvant chemotherapy in combination with HERCEPTIN® has been shown to reduce the relative risk of relapse by 52% and relative risk of death by 33%. The National Comprehensive Cancer Network (NCCN) has recommended adjuvant chemotherapy with HERCEPTIN® for patients with small, HER positive, node-negative tumors, including those with T1bN0 tumors, even though there are little or no data supporting this recommendation, because these patients are generally not included in adjuvant therapy studies. Further, the chemotherapy regimens often recommended (ACTH, TCH) along with HERCEPTIN® are relatively toxic.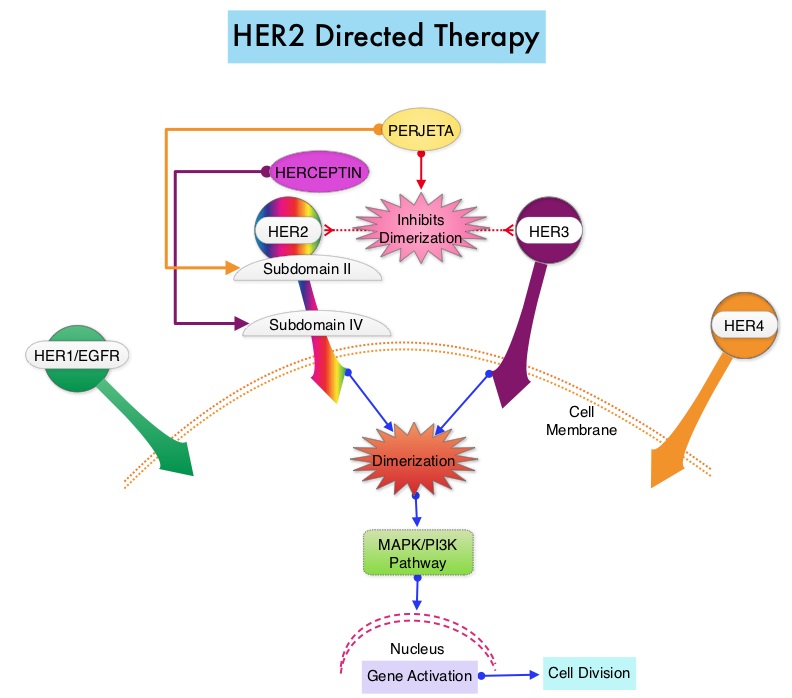
In a previously published study, it was noted that a less toxic regimen such as HERCEPTIN®, given along with weekly TAXOL® (Paclitaxel), had significant efficacy in patients with node negative patients with tumors measuring up to 3 cm in greatest dimension, decreasing the risk of recurrence in this patient group, most notable during the first three years after diagnosis. (Tolaney SM, Barry WT, Dang CT, et al. N Engl J Med 2015;372:134-141). Risk risk factors associated with HERCEPTIN® induced cardiotoxicity include, age over 50 years, borderline LVEF (Left Ventricular Ejection Fraction) before HERCEPTIN® treatment, history of cardiovascular disease, cardiovascular risk factors such as diabetes, dislipidemia or elevated body mass index (>30), sequence in which chemotherapy is administered and prior treatment with Anthracyclines (cumulative doses more than 300 mg/m2). However, unlike Anthracycline induced cardiotoxicity, HERCEPTIN® induced cardiotoxicity is reversible and there are no ultrastructural changes noted in cardiomyocytes in HERCEPTIN® induced cardiotoxicity.
This publication is a secondary analysis of the above mentioned previously published study and the authors here reported the cardiac safety data of a HERCEPIN® based nonanthracycline treatment, (TAXOL® with HERCEPTIN®), for patients with early-stage, node negative, HER2 positive breast cancer and the utility of monitoring LVEF in this patient group. This clinical trial enrolled 406 patients with node-negative, HER2 positive breast cancer 3 cm, or smaller with a baseline LVEF of 50% or greater. Treatment consisted of TAXOL® 80 mg/m2 IV weekly administered concurrently with HERCEPTIN® IV for 12 weeks, followed by HERCEPTIN® monotherapy for 39 weeks. HERCEPTIN® could be administered 2 mg/kg weekly or 6 mg/kg every 3 weeks during the monotherapy phase. Radiation and hormone therapy were administered as planned, following completion of the 12 weeks of chemotherapy. Patient LVEF was assessed at baseline, 12 weeks, 6 months, and 1 year. Median age was 55 years and 29% of the patients had hypertension, and 7% had diabetes. The median follow up was 4 years.
It was noted that a significant, asymptomatic LVEF decline was seen in 3.2% of the patients and 0.5% developed grade 3 Left Ventricular Systolic Dysfunction. The median LVEF at baseline was 65%, at 12 weeks was 64%, at 6 months was 64%; and at 1 year was 64%. The authors concluded that cardiotoxicity from a combination of TAXOL® and HERCEPTIN® is low and a baseline LVEF assessment may be adequate for the majority of patients although serial LVEF assessments could be considered for patients considered at a higher risk for cardiotoxicity. Cardiac Outcomes of Patients Receiving Adjuvant Weekly Paclitaxel and Trastuzumab for Node-Negative, ERBB2-Positive Breast Cancer. Dang C, Guo H, Najita J, et al. JAMA Oncol. 2016;2:29-36
