
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer, and 1 in 9 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, about 191,930 new cases of prostate cancer will be diagnosed in 2020 and 33,330 men will die of the disease. TransRectal UltraSound (TRUS) guided biopsy has been the standard of care for diagnosing prostate cancer in men with a clinical suspicion of prostate cancer, based on an abnormal Digital Rectal Examination and/or an elevated Prostate Specific Antigen (PSA) level. TransRectal UltraSound (TRUS) guided biopsy is a blind biopsy of the lateral and posterior peripheral zone of the prostate using a template, and 10 to 12 cores of prostate tissue is obtained (Systematic Biopsy). Even though this may result in a higher rate of prostate cancer detection, many detected cancers are low grade tumors that do not benefit from treatment, and these patients are on active surveillance for their low risk disease. The major limitation of this biopsy procedure is the risk of under-sampling a more significant tumor that is located in a region of the prostate not usually targeted with a template. Further, in patients with a rising PSA with a prior negative biopsy, patients are often subjected to a repeat blind biopsy with the same limitations as the original biopsy. Since biopsy access is through the rectum and only specific zones of the prostate are sampled, large areas of the prostate, especially the anterior and central prostate, are not routinely sampled and clinically significant higher-grade cancers are sometimes missed.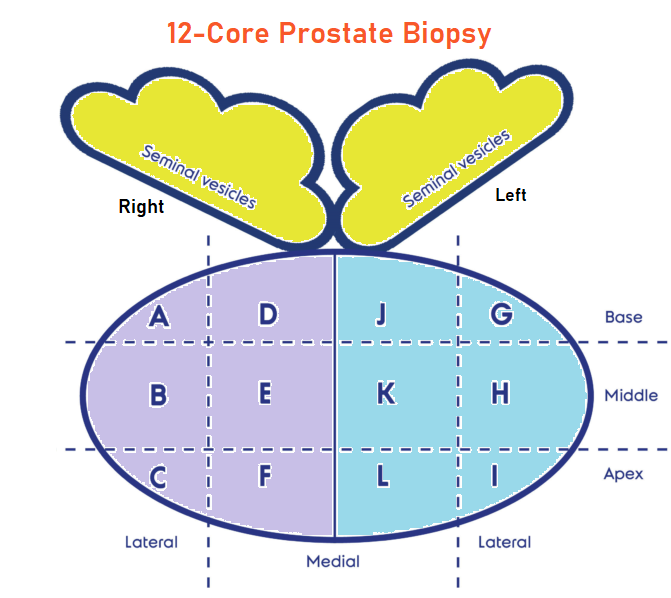
Multiparametric MRI (mp-MRI) combines anatomic imaging in the form of T2-weighted imaging, with functional imaging and is being used to detect or rule out cancer in men who have persistent concern for prostate cancer. Previously published studies have shown that MRI-targeted biopsies alone have shown similar or higher rates of detection of clinically SIGNIFICANT cancer in the prostate gland (high grade cancers) and lower rates of detection of clinically INSIGNIFICANT cancer, when compared to systematic biopsy (standard TRUS guided biopsy). This interesting advantage appears to allow the use of mp-MRI as a triage test to avoid a biopsy if the results were negative, and if positive could be used for targeting abnormal areas in the prostate during biopsy. Despite this advantage, debate persists whether MRI-targeted biopsy should be used in place of systematic biopsy or in conjunction with it.
The Trio Study is a substudy of a larger clinical trial called, Use of Tracking Devices to Locate Abnormalities During Invasive Procedures. In this substudy, the authors assessed the use of MRI-targeted, systematic, or combined MRI-targeted and systematic prostate biopsy, in an attempt to define the most effective method for prostate cancer diagnosis.
In this study a total of 2732 men with abnormal PSA or Digital Rectal Exam underwent prostate MRI. Among these patients, 2103 men had MRI-visible lesions and subsequently underwent both MRI-targeted and systematic biopsies. Grade group 1 refers to clinically INSIGNIFICANT disease (Gleason score, 3+3=6), Grade group 2 or higher refers to cancer with favorable intermediate risk or worse (Gleason score, 3+4=7), and Grade group 3 or higher refers to clinically SIGNIFICANT cancer with unfavorable intermediate risk or worse (Gleason score, 4+3=7). The Primary outcome of this study was cancer detection rates according to Grade group (Clustering of Gleason grades) for each biopsy method, and in combination.
Among all 2103 patients who underwent the two biopsy methods, prostate cancer was diagnosed in 52.5% with systematic biopsy alone and in 51.5% with MRI-targeted biopsy alone. The addition of MRI-targeted biopsy to systematic biopsy led to 208 more prostate cancer diagnoses for a total prostate cancer diagnosis of 62.4%. MRI-targeted biopsy detected more clinically SIGNIFICANT Grade group 3 or higher cancers than systematic biopsy (P=0.004) and detected fewer cancers in Grade group 1 (P<0.001). Of the 404 patients who subsequently underwent radical prostatectomy, disease upgrading on histopathology occurred in 41.6% of patients when compared to findings on systematic biopsy alone, 30.9% when compared with findings on MRI-targeted biopsy alone and 14.4% when compared with findings on combined systematic and MRI-targeted biopsy.
The authors concluded that among patients with MRI-visible lesions, a combination of systematic and MRI-targeted biopsy increases the detection of clinically significant prostate cancers, compared to either strategy alone. MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. Ahdoot M, Wilbur AR, Reese SE, et al. N Engl J Med 2020; 382:917-928
Tag: Prostate Cancer
Association Between Pseudoprogression and Outcomes in Men with Metastatic Castration-Resistant Prostate Cancer Treated with XTANDI®
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer, and 1 in 9 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, about 174,650 new cases of prostate cancer were diagnosed in 2019 and 31,620 men died of the disease. The development and progression of prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) or testosterone suppression has therefore been the cornerstone of treatment of advanced prostate cancer and is the first treatment intervention. Androgen Deprivation Therapies have included bilateral orchiectomy or Gonadotropin Releasing Hormone (GnRH) analogues, with or without first generation Androgen Receptor (AR) inhibitors such as CASODEX® (Bicalutamide), NILANDRON® (Nilutamide) and EULEXIN® (Flutamide) or with second-generation, anti-androgen agents, which include, ZYTIGA® (Abiraterone), XTANDI® (Enzalutamide), ERLEADA® (Apalutamide) and NUBEQA® (Darolutamide). Approximately 10-20% of patients with advanced prostate cancer will progress to Castration Resistant Prostate Cancer (CRPC) within five years during ADT, and over 80% of these patients will have metastatic disease at the time of CRPC diagnosis (mCRPC). Among those patients without metastases at CRPC diagnosis, 33% are likely to develop metastases within two years. The estimated mean survival of patients with CRPC is 9-36 months.
The skeletal system is the most common site for distant metastases among patients with prostate cancer and over 80% of patients with advanced prostate cancer develop bone metastases, which are osteoblastic (or sclerotic), characterized by deposition of new bone. Bone scan is the most common and cost effective modality for the diagnosis of bone metastases and Technetium (Tc) 99m-labeled methylene diphosphonate is the most widely used bone scanning agent. Bone scans are commonly used to both diagnose and monitor disease progression in the bone, among patients with advanced prostate cancer, with a sensitivity ranging from 60-90% but with lower specificity. Bone scan however is more sensitive and specific than plain films and CT scans, whereas MRI is superior in evaluating vertebral metastases. Bone scan provides information on osteoblastic activity and skeletal vascularity, with preferential uptake at sites of active bone formation, reflecting the metabolic reaction of bone to the disease activity, regardless of whether it is neoplastic, traumatic or inflammatory. It is for these reasons it has been well known that bone scans can be misleading in determining whether a patient with bone metastases is benefiting from a treatment, particularly endocrine therapy. The Prostate Cancer Working Group (PCWG) recommended that the assessment of disease progression in bone in the absence of other signs of progression, requires that new lesions detected on the first post-treatment scan be confirmed with the documentation of additional new lesions on the next follow-up scan, in the absence of other signs of disease progression. This is because the new lesions detected on the first post-treatment scan may either reflect true progression or can be the result of bone healing known as pseudoprogression (also known as bone scan flare) that can be misinterpreted as treatment failure, and lead to the premature discontinuation of an effective therapy. Even though the occurrence of pseudoprogression is well documented, its association with clinical outcomes in large prospective studies has not been evaluated.
The authors therefore conducted a post hoc retrospective analysis of the PREVAIL (A Safety and Efficacy Study of Oral MDV3100 in Chemotherapy-Naive Patients With Progressive Metastatic Prostate Cancer) and AFFIRM (Safety and Efficacy Study of MDV3100 in Patients With Castration-Resistant Prostate Cancer Who Have Been Previously Treated With Docetaxel-based Chemotherapy) studies to determine the association between new unconfirmed lesions detected on a follow up bone scan, and clinical outcomes in XTANDI® (Enzalutamide)-treated men with mCRPC. The PREVAIL and AFFIRM trials were both designed in accordance with the PCWG guidelines. This analysis included 643 patients from the PREVAIL study who had not received Docetaxel and 404 men from the AFFIRM study who had previously received Docetaxel. Eligible patients had stable disease or response to therapy based on non-bone disease criteria, including assessment of PSA and soft-tissue disease response. Pseudoprogression was defined as detection of one or more lesions on a first post-treatment bone scan (at week 9 in PREVAIL or 13 in AFFIRM) or a second bone scan (at week 17 in PREVAIL or 25 in AFFIRM), without subsequent new lesions detected at later assessments. The authors evaluated the association of the new lesions detected on the first and second bone scans, with radiographic Progression Free Survival (rPFS), Overall Survival (OS), PSA decline, Objective Response in soft tissue, and Quality of Life.
In the PREVAIL study, new unconfirmed bone lesions were detected on bone scans in 27.5% of Docetaxel-naive patients. The rPFS, OS and time to PSA progression among these patients was similar to those without new lesions, suggesting pseudoprogression. In the AFFIRM study, new, unconfirmed lesions were detected in 18.1% of Docetaxel-treated patients and the rPFS, and time to PSA progression among these patients was similar to those without new lesions on bone scans. However, the OS was significantly worse among these patients, compared with those without new lesions on bone scan, suggesting true disease progression. Most lesions were detected on the first follow up bone scan and investigators were unable to identify any pretreatment factor associated with the development of new, unconfirmed lesions in patients responding to XTANDI®, in either clinical setting.
It was concluded that new unconfirmed lesions detected on follow up bone scans within the first 4 months of treatment initiation may represent pseudoprogression in men with mCRPC and are indicative of a favorable treatment response to XTANDI®. However, new unconfirmed bone lesions in men with mCRPC who were previously treated with Docetaxel may reflect disease heterogeneity and true progression with associated worse Overall Survival. Treatment discontinuation can be considered in this patient group, taking into consideration other disease manifestations such as changes in PSA level, finding on soft tissue imaging, symptoms, and patient preferences. These findings reinforce the importance of functional imaging for diagnosing bone metastases. Association Between New Unconfirmed Bone Lesions and Outcomes in Men With Metastatic Castration-Resistant Prostate Cancer Treated With Enzalutamide: Secondary Analysis of the PREVAIL and AFFIRM Randomized Clinical Trials. Armstrong AJ, Al-Adhami M, Lin P, et al. JAMA Oncol. 2019 Dec 12. doi: 10.1001/jamaoncol.2019.4636. [Epub ahead of print]
The skeletal system is the most common site for distant metastases among patients with prostate cancer and over 80% of patients with advanced prostate cancer develop bone metastases, which are osteoblastic (or sclerotic), characterized by deposition of new bone. Bone scan is the most common and cost effective modality for the diagnosis of bone metastases and Technetium (Tc) 99m-labeled methylene diphosphonate is the most widely used bone scanning agent. Bone scans are commonly used to both diagnose and monitor disease progression in the bone, among patients with advanced prostate cancer, with a sensitivity ranging from 60-90% but with lower specificity. Bone scan however is more sensitive and specific than plain films and CT scans, whereas MRI is superior in evaluating vertebral metastases. Bone scan provides information on osteoblastic activity and skeletal vascularity, with preferential uptake at sites of active bone formation, reflecting the metabolic reaction of bone to the disease activity, regardless of whether it is neoplastic, traumatic or inflammatory. It is for these reasons it has been well known that bone scans can be misleading in determining whether a patient with bone metastases is benefiting from a treatment, particularly endocrine therapy. The Prostate Cancer Working Group (PCWG) recommended that the assessment of disease progression in bone in the absence of other signs of progression, requires that new lesions detected on the first post-treatment scan be confirmed with the documentation of additional new lesions on the next follow-up scan, in the absence of other signs of disease progression. This is because the new lesions detected on the first post-treatment scan may either reflect true progression or can be the result of bone healing known as pseudoprogression (also known as bone scan flare) that can be misinterpreted as treatment failure, and lead to the premature discontinuation of an effective therapy. Even though the occurrence of pseudoprogression is well documented, its association with clinical outcomes in large prospective studies has not been evaluated.
The authors therefore conducted a post hoc retrospective analysis of the PREVAIL (A Safety and Efficacy Study of Oral MDV3100 in Chemotherapy-Naive Patients With Progressive Metastatic Prostate Cancer) and AFFIRM (Safety and Efficacy Study of MDV3100 in Patients With Castration-Resistant Prostate Cancer Who Have Been Previously Treated With Docetaxel-based Chemotherapy) studies to determine the association between new unconfirmed lesions detected on a follow up bone scan, and clinical outcomes in XTANDI® (Enzalutamide)-treated men with mCRPC. The PREVAIL and AFFIRM trials were both designed in accordance with the PCWG guidelines. This analysis included 643 patients from the PREVAIL study who had not received Docetaxel and 404 men from the AFFIRM study who had previously received Docetaxel. Eligible patients had stable disease or response to therapy based on non-bone disease criteria, including assessment of PSA and soft-tissue disease response. Pseudoprogression was defined as detection of one or more lesions on a first post-treatment bone scan (at week 9 in PREVAIL or 13 in AFFIRM) or a second bone scan (at week 17 in PREVAIL or 25 in AFFIRM), without subsequent new lesions detected at later assessments. The authors evaluated the association of the new lesions detected on the first and second bone scans, with radiographic Progression Free Survival (rPFS), Overall Survival (OS), PSA decline, Objective Response in soft tissue, and Quality of Life.
In the PREVAIL study, new unconfirmed bone lesions were detected on bone scans in 27.5% of Docetaxel-naive patients. The rPFS, OS and time to PSA progression among these patients was similar to those without new lesions, suggesting pseudoprogression. In the AFFIRM study, new, unconfirmed lesions were detected in 18.1% of Docetaxel-treated patients and the rPFS, and time to PSA progression among these patients was similar to those without new lesions on bone scans. However, the OS was significantly worse among these patients, compared with those without new lesions on bone scan, suggesting true disease progression. Most lesions were detected on the first follow up bone scan and investigators were unable to identify any pretreatment factor associated with the development of new, unconfirmed lesions in patients responding to XTANDI®, in either clinical setting.
It was concluded that new unconfirmed lesions detected on follow up bone scans within the first 4 months of treatment initiation may represent pseudoprogression in men with mCRPC and are indicative of a favorable treatment response to XTANDI®. However, new unconfirmed bone lesions in men with mCRPC who were previously treated with Docetaxel may reflect disease heterogeneity and true progression with associated worse Overall Survival. Treatment discontinuation can be considered in this patient group, taking into consideration other disease manifestations such as changes in PSA level, finding on soft tissue imaging, symptoms, and patient preferences. These findings reinforce the importance of functional imaging for diagnosing bone metastases. Association Between New Unconfirmed Bone Lesions and Outcomes in Men With Metastatic Castration-Resistant Prostate Cancer Treated With Enzalutamide: Secondary Analysis of the PREVAIL and AFFIRM Randomized Clinical Trials. Armstrong AJ, Al-Adhami M, Lin P, et al. JAMA Oncol. 2019 Dec 12. doi: 10.1001/jamaoncol.2019.4636. [Epub ahead of print]
XTANDI® (Enzalutamide)
The FDA on December 16, 2019 approved XTANDI® for patients with metastatic Castration-Sensitive Prostate Cancer (mCSPC). XTANDI® is a product of Astellas Pharma Inc.
Higher Levels of IGF-1 and Free Testosterone Increase the Risk of Prostate Cancer
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer, and 1 in 9 men will be diagnosed with Prostate cancer during their lifetime. It is estimated that in the United States, about 174,650 new cases of Prostate cancer will be diagnosed in 2019 and 31,620 men will die of the disease. The etiology of Prostate cancer remains unclear, and North American Blacks are at the highest risk whereas risk is lowest in Asians, with the risk among Caucasians somewhere in between.
The Insulin-like Growth Factor (IGF) system has been reported to regulate normal and malignant cell growth, proliferation and differentiation, tissue homeostasis and cellular metabolism, and its relevance in carcinogenesis has been well established. The role of IGF system in Prostate cancer was initially recognized from epidemiological studies which showed that higher serum IGF-1 concentrations correlated with an increased risk of Prostate cancer. Testosterone in the circulation is bound primarily to Sex Hormone Binding Globulin (SHBG) while the unbound, or free testosterone, is the most bioavailable and active form.
The authors in this large prospective study investigated the association of circulating levels of IGF-I, free (biologically active testosterone) and total testosterone, and Sex Hormone Binding Globulin (SHBG) with Prostate cancer incidence and mortality, in a large cohort of patients. This study included 200,452 male participants who were free of cancer when they were enrolled in the study, and were not taking any hormone therapy. Baseline blood samples were obtained from these men and tested for levels of total testosterone and IGF-1. Free testosterone level was calculated from measured total testosterone and binding protein concentrations.
After a mean follow up of 6.9 years, 5412 men were diagnosed with Prostate cancer and 296 had died from the disease. It was noted that higher levels of circulating IGF-I was associated with an elevated risk of Prostate cancer diagnosis, as well as Prostate cancer mortality. Higher free testosterone level was associated with an elevated risk of incident Prostate cancer, whereas higher SHBG was associated with a lower risk, but neither was associated with Prostate cancer mortality. Total testosterone levels were not associated with Prostate cancer incidence or mortality. For every 5 nanomoles increase in the concentration of IGF-1 per liter of blood (5 nmol/L), men were 9% more likely to develop Prostate cancer. For every 50 picomoles increase of free testosterone per liter of blood (50 pmol/L), there was a 10% increase in Prostate cancer risk. The researchers added that their findings correspond to a 25% greater risk of Prostate cancer in men who have the highest levels of IGF-1, compared to those with the lowest, and men with the highest free testosterone levels have a 18% greater risk of Prostate cancer, compared to those with the lowest levels.
It was concluded from this study that circulating levels of IGF-I and free testosterone play a role in the development of Prostate cancer and these two hormones could be one of the several mechanisms that links diet, lifestyle, and body size with the risk of Prostate cancer, taking us one step closer to Prostate cancer prevention. Serum hormones and prostate cancer incidence and mortality in UK Biobank. Travis R, Watts E, Fensom G, et al. Presented at the 2019 NCRI Cancer Conference. Abstract#2904
Late breaking Abstract – ESMO 2019 Targeted Therapy with LYNPARZA® Delays Progression of Advanced Prostate Cancer
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer, and 1 in 9 men will be diagnosed with Prostate cancer during their lifetime. It is estimated that in the United States, about 174,650 new cases of Prostate cancer will be diagnosed in 2019 and 31,620 men will die of the disease. The development and progression of Prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) or testosterone suppression has therefore been the cornerstone of treatment of advanced Prostate cancer and is the first treatment intervention. Androgen Deprivation Therapies have included bilateral orchiectomy or Gonadotropin Releasing Hormone (GnRH) analogues, with or without first generation Androgen Receptor (AR) inhibitors such as CASODEX® (Bicalutamide), NILANDRON® (Nilutamide) and EULEXIN® (Flutamide) or with second-generation, anti-androgen agents, which include, ZYTIGA® (Abiraterone), XTANDI® (Enzalutamide) and ERLEADA® (Apalutamide). ZYTIGA® inhibits CYP17A1 enzyme and depletes adrenal and intratumoral androgens, thereby impairing AR signaling. XTANDI® and ERLEADA® compete with Testosterone and Dihydrotestosterone and avidly binds to the Androgen Receptor, thereby inhibiting AR signaling, and in addition inhibits translocation of the AR into the nucleus and thus inhibits the transcriptional activities of the AR.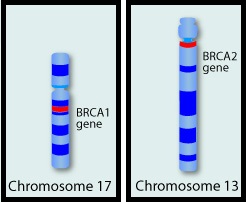
Approximately 10-20% of patients with advanced Prostate cancer will progress to Castration Resistant Prostate Cancer (CRPC) within five years during ADT, and over 80% of these patients will have metastatic disease at the time of CRPC diagnosis. Among those patients without metastases at CRPC diagnosis, 33% are likely to develop metastases within two years. The estimated mean survival of patients with CRPC is 9-36 months and there is therefore an unmet need for new effective therapies.
The malignant transformation of prostatic epithelial cell as well as the development of CRPC has been attributed to deleterious alterations in a variety of genes including loss-of-function alterations in Homologous Recombination repair genes such as BRCA1, BRCA2 and ATM. Homologous Recombination (HR) is a type of genetic recombination, and this DNA repair pathway is used by cells to accurately repair DNA double-stranded breaks (DSBs) and thereby maintain genomic integrity. Homologous Recombination Deficiency (HRD) is noted following mutation of genes involved in HR repair pathway. At least 15 genes are involved in the Homologous Recombination Repair (HRR) pathway including BRCA1 and BRCA2 genes. BRCA1 and BRCA2 are tumor suppressor genes and functional BRCA proteins repair damaged DNA, and play an important role in maintaining cellular genetic integrity. They regulate cell growth and prevent abnormal cell division and development of malignancy. Mutations in BRCA1 and BRCA2 account for about 20-25% of hereditary breast cancers and about 5-10% of all breast cancers. They also account for 15% of ovarian cancers, in addition to other cancers such as Colon and Prostate. BRCA mutations can either be inherited (Germline) and present in all individual cells or can be acquired and occur exclusively in the tumor cells (Somatic). Somatic mutations account for a significant portion of overall BRCA1 and BRCA2 aberrations. Loss of BRCA function due to frequent somatic aberrations likely deregulates Homologous Recombination (HR) pathway and increases sensitivity to platinum drugs. Majority of the individuals with Germline BRCA mutations (gBRCA) are positive for HR deficiency.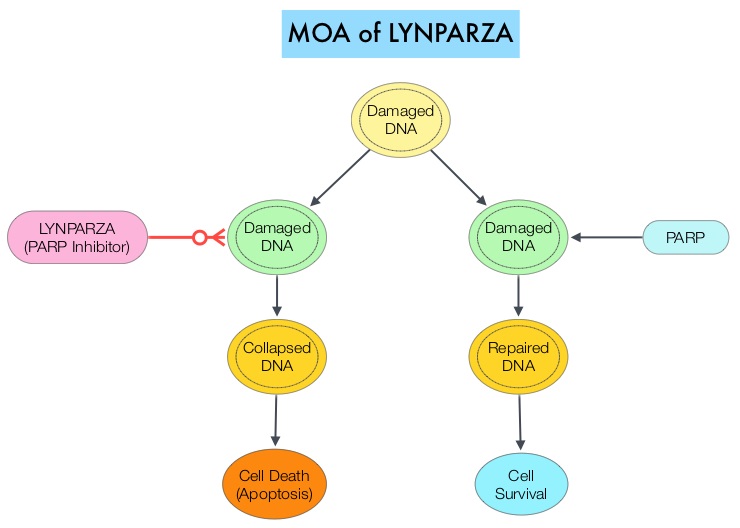
The PARP (Poly ADP Ribose Polymerase) family of enzymes which include PARP1 and PARP2 repair damaged DNA. PARP inhibitors inhibit the PARP protein in cancer cells and kill tumors defective in the BRCA1 or BRCA2 genes through the concept of synthetic lethality. LYNPARZA® (Olaparib) is a first-in-class PARP inhibitor and blocks DNA damage response in tumors harboring a deficiency in Homologous Recombination Repair, as is noted in those with mutations such as BRCA1 and/or BRCA2. LYNPARZA® showed promising results in a Phase II trial (TOPARP), when given as monotherapy, in patients with BRCA1/2 or ATM gene-mutated mCRPC, who had received a prior Taxane-based chemotherapy, and at least one newer hormonal agent (ZYTIGA® or XTANDI®).
PROfound is a prospective, multicentre, randomized, open-label, Phase III trial in which the efficacy and safety of LYNPARZA® was compared with physician’s choice of either XTANDI® or ZYTIGA® in two groups of patients with mCRPC, who had progressed on prior treatment with new hormonal anticancer treatments, and had a qualifying tumor mutation in one of 15 genes involved in the Homologous Recombination Repair (HRR) pathway. Those in Cohort A (N=245) had alterations in BRCA1, BRCA2 or ATM genes while those in Cohort B (N=142) had alterations in any one of 12 other genes known to be involved in DNA repair which included BRIP1, BARD1, CDK12, CHEK1, CHEK2, FANCL, PALB2, PPP2R2A, RAD51B, RAD51C, RAD51D or RAD54L. Patients were randomized 2:1 within each cohort to receive LYNPARZA® 300 mg orally BID or physician’s choice of XTANDI® 160 mg orally QD or ZYTIGA® 1000 mg orally QD along with Prednisone 5 mg orally BID. Patient characteristics were well-balanced between arms in each treatment group, median patient age was 68 years, approximately 25% of patients had de novo metastatic disease, about 65% of patients received prior Taxane therapy and more than 20% had received two lines of chemotherapy. Patients were allowed to cross over to LYNPARZA® upon progression. The Primary endpoint was radiographic Progression-Free Survival (rPFS) in Cohort A, assessed by Blinded Independent Central Review (BICR). Secondary endpoints included Objective Response Rate (ORR), Time to pain progression and Overall Survival (OS) in Cohort A.
It was noted that in Cohort A, the median PFS was 7.4 months with LYNPARZA®, compared to 3.5 months with hormonal treatment (HR=0.34, P<0.0001). This represented a 66% greater delay in disease progression compared to hormonal therapy. In the overall population (Cohort A+B), median PFS was 5.8 months versus 3.5 months respectively (HR=0.49, P<0.0001). The interim Overall Survival analysis in Cohort A showed that median OS was 18.5 months with LYNPARZA® compared to 15 months with hormonal treatment (HR=0.64, P=0.0173). Median OS in the overall population (Cohort A+B) was 17.5 months versus 14.2 months with LYNPARZA® versus hormonal treatment, respectively (HR 0.67, P=0.0063). In Cohort A, the Objective Response Rate (ORR) was 33.3% with LYNPARZA® compared with 2.3% with the hormonal therapies (P<0.0001). The median Time to pain progression was not yet reached with LYNPARZA® compared with 9.9 months for the hormonal agents. This suggested a 56% reduction in the risk of pain progression (HR=0.44; P=0.019). The most common Adverse Events associated with LYNPARZA® were nausea, decreased appetite, anemia and fatigue.
It was concluded that in this landmark, molecularly targeted, Phase III trial, LYNPARZA® improved Progression Free Survival and Objective Response Rates, with a trend for Overall Survival, among patients with heavily pretreated metastatic CRPC, and alterations in the Homologous Recombination Repair genes. PROFOUND: Phase III study of olaparib versus enzalutamide or abiraterone for metastatic castration-resistant prostate cancer (mCRPC) with homologous recombination repair (HRR) gene alterations. Hussain M, Mateo J, Fizazi K, et al. Presented at ESMO Congress 2019; September 27-October 1, 2019; Barcelona, Spain. Abstract LBA12_PR.
ERLEADA® (Apalutamide)
The FDA on September 17, 2019 approved ERLEADA® for patients with metastatic Castration-Sensitive Prostate Cancer (CSPC). ERLEADA® was initially approved in 2018 for patients with non-metastatic Castration-Resistant Prostate Cancer (CRPC). ERLEADA® is a product of Janssen Biotech, Inc.
NUBEQA® (Darolutamide)
The FDA on July 30, 2019 approved NUBEQA® for non-metastatic Castration-Resistant Prostate Cancer (CRPC). NUBEQA® is a product of Bayer HealthCare Pharmaceuticals Inc.
Association between Androgen Deprivation Therapy and Diagnosis of Alzheimer Disease or Dementia in Patients with Prostate Cancer
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer, and 1 in 9 men will be diagnosed with Prostate cancer during their lifetime. It is estimated that in the United States, about 174,650 new cases of Prostate cancer will be diagnosed in 2019 and 31,620 men will die of the disease. The development and progression of Prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) or testosterone suppression has therefore been the cornerstone of treatment of advanced Prostate cancer and is the first treatment intervention. Androgen Deprivation Therapies have included bilateral orchiectomy or Gonadotropin Releasing Hormone (GnRH) analogues, with or without first generation Androgen Receptor (AR) inhibitors such as CASODEX® (Bicalutamide), NILANDRON® (Nilutamide) and EULEXIN® (Flutamide). The first-generation Androgen Receptor (AR) inhibitors act by binding to the Androgen Receptor (AR) and prevent the activation of the AR and subsequent up-regulation of androgen responsive genes. They may also accelerate the degradation of the AR. These agents have a range of pharmacologic activity from being pure anti-androgens to androgen agonists. The second-generation, anti-androgen agents include, ZYTIGA® (Abiraterone), XTANDI® (Enzalutamide) and ERLEADA® (Apalutamide). ZYTIGA® inhibits CYP17A1 enzyme and depletes adrenal and intratumoral androgens, thereby impairing AR signaling. XTANDI® and ERLEADA® compete with Testosterone and Dihydrotestosterone and avidly binds to the Androgen Receptor, thereby inhibiting AR signaling, and in addition inhibits translocation of the AR into the nucleus and thus inhibits the transcriptional activities of the AR.
Androgen Deprivation Therapy (ADT) is often recommended alone or as a part of multimodality therapy, as ADT reduces the likelihood of cancer progression and/or mortality, in high-risk localized, locally advanced, recurrent, or metastatic Prostate cancer. ADT however can be associated with side effects such as fatigue, loss of muscle mass, impotence, anemia, osteoporosis, depression, etc., which in turn can have a significant negative impact on an individual’s quality of life. ADT has also been associated with cognitive dysfunction and there has been conflicting evidence establishing an association between ADT use and diagnosis of Alzheimer disease or Dementia. It has been postulated that lower testosterone levels impair neuron growth and axonal regeneration, in addition to accumulation of abnormally folded β-amyloid protein. With the earlier introduction of ADT in the course of disease progression for patients with Prostate cancer, it is important to discuss the association between ADT and Dementia with patients, which in turn can improve shared decision making around the risks and benefits of ADT in Prostate cancer.
The present study was conducted to analyze the association between ADT exposure and diagnosis of Alzheimer disease or Dementia, among elderly men with Prostate cancer. The authors in this retrospective cohort study used data from the NCI’s Surveillance, Epidemiology, and End Results (SEER)-Medicare linked database, and the participants included 154,089 elderly men with newly diagnosed Prostate cancer, between 1996 and 2003. The analyses were conducted in 2018 and patients receiving ADT within 2 years of Prostate cancer diagnosis were identified. In this study, 62,330 men received ADT within 2 years of Prostate cancer diagnosis, and 91,759 men did not receive ADT. Mean follow up was 8.3 years, and survival analysis was used to determine association between ADT exposure and diagnosis of Alzheimer disease or Dementia.
The researchers noted that exposure to ADT, compared with no ADT exposure, was associated with a diagnosis of Alzheimer disease (13.1% vs 9.4%; HR=1.14; P<0.001) and Dementia (21.6% vs 15.8%; HR=1.20; P<0.001). There was a dose-response relationship and patients who received more than 8 doses of ADT were at a significantly higher hazard of diagnosis of both Alzheimer disease and Dementia, than those receiving fewer doses ADT.
The authors concluded that over a follow-up period of at least 10 years, ADT exposure among elderly patients with Prostate cancer was associated with subsequent diagnosis of Alzheimer disease or Dementia. They added that clinicians should carefully weigh the long-term risks and benefits of ADT, in patients with a prolonged life expectancy, and stratify patients based on Dementia risk, prior to ADT initiation. Association Between Androgen Deprivation Therapy Use and Diagnosis of Dementia in Men With Prostate Cancer. Jayadevappa R, Chhatre S, Malkowicz SB, et al. JAMA Netw Open. 2019;2(7):e196562. doi:10.1001/jamanetworkopen.2019.6562
Darolutamide in Nonmetastatic Castration-Resistant Prostate Cancer
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer, and 1 in 9 men will be diagnosed with Prostate cancer during their lifetime. It is estimated that in the United States, about 174,650 new cases of Prostate cancer will be diagnosed in 2019 and 31,620 men will die of the disease. The development and progression of Prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) or testosterone suppression has therefore been the cornerstone of treatment of advanced Prostate cancer and is the first treatment intervention. Androgen Deprivation Therapies have included bilateral orchiectomy or Gonadotropin Releasing Hormone (GnRH) analogues, with or without first generation Androgen Receptor (AR) inhibitors such as CASODEX® (Bicalutamide), NILANDRON® (Nilutamide) and EULEXIN® (Flutamide). The median duration of response is approximately 1 year and majority of these patients progress to Castration Resistant Prostate Cancer (CRPC). The mechanism of resistance to Androgen Deprivation Therapy (ADT) include reactivation of Androgen Receptor signaling through persistent adrenal androgen production, modification of the biologic characteristics of Androgen Receptors, intratumoral testosterone production and parallel steroidogenic pathways. Progression to Castration Resistant Prostate Cancer (CRPC) often manifests itself with a rising PSA (Prostate Specific Antigen), and watchful waiting is recommended in men with non-metastatic CRPC. However, those with a rapidly rising PSA on ADT (doubling time of less than 8-10 months), are at significantly greater risk of developing metastases and death.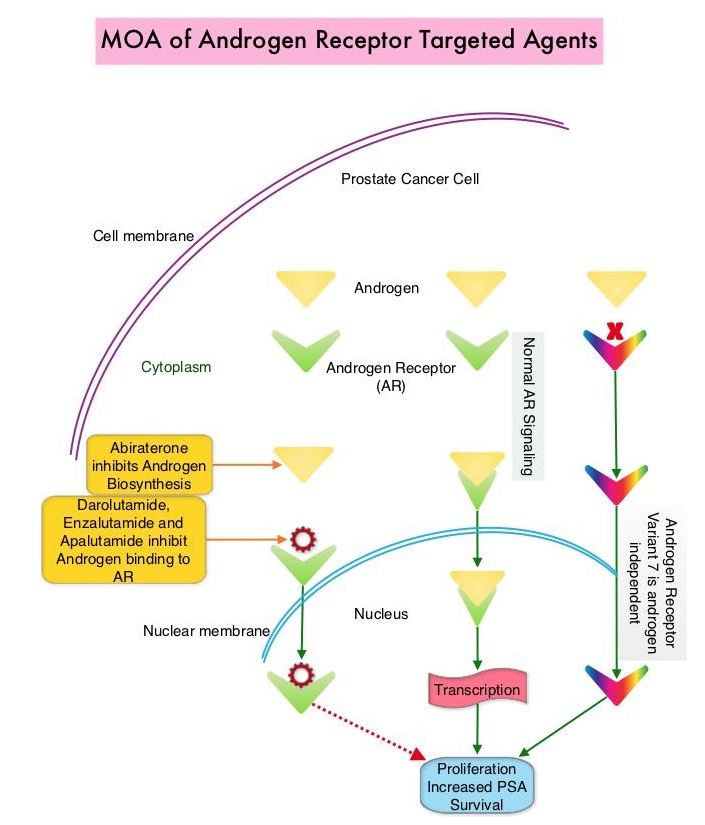
The Androgen-Receptor inhibitors ERLEADA® (Apalutamide) and XTANDI® (Enzalutamide) have recently been approved for the treatment of nonmetastatic CRPC. However, patients who may already be experiencing adverse effects from their ongoing ADT may experience additional toxicities from these agents. There is therefore an unmet need for therapies with improved safety and toxicity profiles.
Darolutamide is a nonsteroidal AR antagonist with a unique molecular structure that is distinct from other AR antagonists and exhibits tighter binding affinity to the AR than ERLEADA® and XTANDI®, resulting in strong androgen inhibitory activity. Darolutamide and its major metabolite are full antagonists and retain their activity against known AR mutations shown to enable resistance to first- and second-generation ADTs. Additionally, Darolutamide has low penetration of the blood-brain barrier and low binding affinity for Gamma AminoButyric Acid type A receptors, which in turn reduces the risk of CNS-related Adverse Events such as seizures, and results in less severe toxic effects than ERLEADA® and XTANDI®, in patients with CRPC. Darolutamide and its active metabolite have been shown to inhibit testosterone-induced translocation of AR to the nucleus, thus decreasing activation of genes required for the growth and survival of prostate tumor cells.
Based on the significant antitumor activity of Darolutamide in Phase I and II studies, as well as favorable side effect profile, the authors conducted a multinational, randomized, double-blind, placebo-controlled, Phase III trial (ARAMIS- Androgen Receptor Antagonizing Agent for Metastasis-free Survival), involving 1509 patients with nonmetastatic, Castration-Resistant Prostate Cancer (CRPC) and a Prostate Specific Antigen doubling time of 10 months or less and a baseline PSA level of at least 2 ng/ml. Patients were randomly assigned in a 2:1 ratio to receive Darolutamide 600 mg orally twice daily or placebo. Patients continued to receive ADT (Luteinizing Hormone Releasing Hormone agonist or antagonist) throughout the trial. The median patient age was 74 years, median time from initial diagnosis was 85 months and approximately 30% of patients were on a bone-sparing agent. The Primary end point was Metastasis-Free Survival, with the presence of metastasis determined by Independent Central Review of radiographic imaging, every 16 weeks. Secondary end points included Overall Survival, Time to pain progression, Time to first symptomatic skeletal event and Time to first cytotoxic chemotherapy. The median follow up was 17.9 months.
The median Metastasis-Free Survival was 40.4 months with Darolutamide, as compared with 18.4 months with placebo (Hazard Ratio for metastasis or death in the Darolutamide group=0.41; P<0.001). This treatment benefit with Darolutamide was consistently favorable across all prespecified subgroups, including in patients with PSA doubling times of 6 months or less or more than 6 months. Darolutamide was also associated with improved Overall Survival, with a lower risk of death (HR=0.71; P=0.045) and longer time to pain progression (40.3 months versus 25.4 months, HR=0.65; P<0.001), compared to the placebo group. The median time to PSA progression was 33.2 months with Darolutamide and 7.3 months with placebo (Hazard ratio for PSA progression or death=0.13; P<0.001). The time to first cytotoxic chemotherapy and time to first symptomatic skeletal event also favored Darolutamide. Adverse Events overall were reported by 83.2% of the patients who received Darolutamide and 76.9% of the patients who received placebo, and patient-reported quality of life was similar in the Darolutamide and placebo group.
It was concluded that among patients with nonmetastatic CRPC, Metastasis-Free Survival was significantly longer with Darolutamide compared with placebo, with similar incidence of Adverse Events and Quality of Life outcomes. Darolutamide in Nonmetastatic Castration-Resistant Prostate Cancer. Fizazi K, Shore N, Tammela TL, et al., for the ARAMIS Investigators. N Engl J Med 2019;380:1235-1246
Late Breaking Abstract – ASCO 2019 XTANDI® Improves Overall Survival in Metastatic Hormone-Sensitive Prostate Cancer
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer, and 1 in 9 men will be diagnosed with Prostate cancer during their lifetime. It is estimated that in the United States, about 174,650 new cases of Prostate cancer will be diagnosed in 2019 and 31,620 men will die of the disease. The development and progression of Prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) or testosterone suppression has therefore been the cornerstone of treatment of advanced Prostate cancer and is the first treatment intervention.
The first-generation NonSteroidal Anti-Androgen (NSAA) agents such as EULEXIN® (Flutamide), CASODEX® (Bicalutamide) and NILANDRON® (Nilutamide) act by binding to the Androgen Receptor (AR) and prevent the activation of the AR and subsequent up-regulation of androgen responsive genes. They may also accelerate the degradation of the AR. These agents have a range of pharmacologic activity from being pure anti-androgens to androgen agonists. CASODEX® is a nonsteroidal oral anti-androgen, that is often prescribed along with GnRH (Gonadotropin-Releasing Hormone) agonists for metastatic disease, or as a single agent second line hormonal therapy for those who had progressed on LHRH agonists. XTANDI® (Enzalutamide) is an orally administered, second-generation, anti-androgen, with no reported agonistic effects. It competitively inhibits androgens and AR binding to androgens as well as AR nuclear translocation and interaction with DNA. It thus inhibits several steps in the AR signaling pathway and was designed to overcome acquired resistance to first-generation nonsteroidal anti-androgens. Previously published studies have shown that XTANDI® improved Overall Survival in Castration-Resistant Prostate Cancer, regardless of whether it was used before or after Docetaxel chemotherapy. The benefits of adding Docetaxel or ZYTIGA® (Abiraterone) to testosterone suppression in men with metastatic, hormone-sensitive Prostate cancer have been established in randomized clinical trials.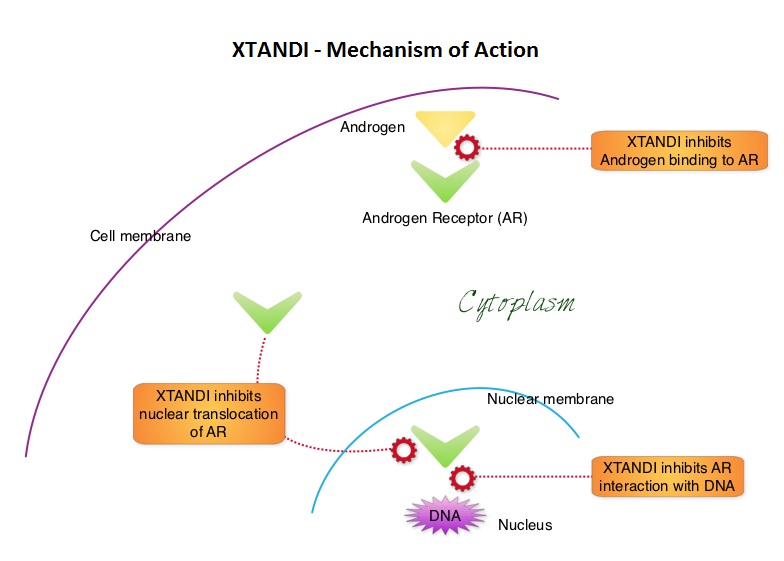
ENZAMET (Enzalutamide in First Line Androgen Deprivation Therapy for Metastatic Prostate Cancer) is an open-label, international, randomized, Phase III trial, conducted to evaluate the benefits of adding XTANDI® to initial standard treatment of Androgen Deprivation Therapy (ADT) with or without early Docetaxel, among patients with metastatic hormone-sensitive Prostate cancer.
A total of 1125 men with metastatic hormone-sensitive Prostate cancer were randomly assigned 1:1 to receive either ADT plus XTANDI® or NonSteroidal Anti-Androgens (NSAA). ADT consisted of parenteral injection of a testosterone-suppressing agent (such as Goserelin, Leuprolide, or Degarelix) with either a 160 mg dose of XTANDI® daily or one of the standard NSAA’s such as CASODEX®, EULEXIN® or NILANDRON®. Of the 1,125 men enrolled in the trial, 503 men received early doses of Docetaxel, and 602 did not. The decision to initiate early treatment with Docetaxel was at the treating physician’s discretion and was administered at 75 mg/m2 IV without prednisone every 3 weeks for a maximum of six cycles. Randomized patients were stratified according to the volume of disease (High Risk- defined as the presence of visceral metastases or at least four bone lesions with at least one lesion located beyond the vertebral bodies and pelvis or low), planned use of early Docetaxel, planned use of bone antiresorptive therapy, and score on ACE-27 (Adult Comorbidity Evaluation 27), with no coexisting conditions rated as 0, mild rated as 1, moderate rated as 2, and severe or multiple conditions rated as 3. The mean age was 68 years, 45% of patients received early Docetaxel as planned treatment and over 50% of the patients had high volume disease. The Primary end point was Overall Survival (OS) and Secondary end points included Progression Free Survival (PFS) as determined by the PSA level, clinical PFS, and adverse events. The median follow up was 34 months.
At the time of the first interim analysis, there was a 33% reduction in the risk of death in the XTANDI® group compared to the standard treatment group ((HR=0.67; P<0.002) and the estimated Overall Survival at 3 years were 80% in the XTANDI® group and 72% in the standard-of-care group. The addition of XTANDI® also improved PSA Progression Free Survival with a 61% reduction in the risk of PSA progression (HR=0.39; P<0.001) and 60% improvement in clinical PFS (HR=0.40; P<0.001). The effects of XTANDI® on clinical PFS were noted in all predefined subgroups, including those with early Docetaxel treatment. Among the patient group who also received early Docetaxel treatment, there was however no significant improvement in Overall Survival. Adding XTANDI® to standard ADT was associated with a higher frequency of toxic effects, especially peripheral neuropathy, associated with the concomitant use of Docetaxel, fatigue and slightly higher risk of seizures compared to standard therapy, and more patients discontinued treatment due to adverse events in the XTANDI® group.
It was concluded that XTANDI® was associated with significantly longer Progression Free Survival and Overall Survival than standard intervention, in men with metastatic, hormone-sensitive Prostate cancer receiving Androgen Deprivation Therapy. Patients who received early Docetaxel treatment, however did not have significant survival benefit. The authors added that ENZAMET is the first metastatic hormone-sensitive Prostate cancer trial to report Overall Survival data of an androgen receptor inhibitor (XTANDI®), and outcomes among a set of patients who also concurrently received Docetaxel. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. Davis ID, Martin AJ, Stockler MR, et al. for the ENZAMET Trial Investigators and the Australian and New Zealand Urogenital and Prostate Cancer Trials Group. June 2, 2019. DOI: 10.1056/NEJMoa1903835