Written by: Carlos Becerra, MD
Content Sponsored by: Bristol Myers Squibb
Dr. Becerra is a paid consultant for BMS and was compensated for his contribution in drafting this article.
Pancreas adenocarcinoma is a highly aggressive and fatal disease that is projected to become the second leading cause of cancer related death in the US by the year 2030.1 Upon diagnosis, over 50% of the patients present with metastatic disease and we do not have an effective screening tool to detect pancreas cancer at an earlier and potentially curable stage.2-3 Some improvement has been made in median survival for patients with metastatic disease due to better supportive measures and more effective chemotherapy options.3-4 However, the COVID 19 pandemic threatens to disrupt the gains obtained in recent years due to delay in diagnosis and management of this disease.5 In the next paragraphs I will review some key features for the management of patients with metastatic pancreas cancer so that patients can continue to benefit from the current available treatment options in spite of the COVID-19 pandemic.
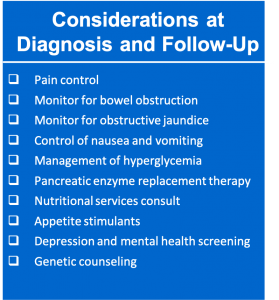
Key elements to consider at diagnosis and during management of patients with metastatic pancreas cancer include pain control with adequate narcotic analgesics titrated to the patient’s pain and consideration for local treatment modalities, such as palliative radiation therapy and celiac block to help control the pain. Patients should also be closely monitored with early intervention in case of bowel obstruction (consider even surgical intervention with a bypass procedure if the patient has an adequate performance status) and obstructive jaundice (with metal stent preferred over plastic stent; Figure 1). Additional elements include adequate control of nausea and vomiting either due to chemotherapy or to bowel dysfunction, optimal management of the hyperglycemia, and replacement therapy with pancreatic enzymes. Consultation of nutritional services and starting medications to stimulate the appetite should also be considered.3,4,6 Genetic counseling for new patients and testing for germline mutations along with testing the tumor for presence of actionable mutations should also be strongly considered, based on recent advances.7 Patients should also be screened for depression.3,4
Figure 1: Key Elements to Consider at Diagnosis and Follow-Up
The overall goal of systemic chemotherapy should be to improve overall survival of patients while maintaining the best possible quality of life.4 To that end we have several treatment options based on evidence from randomized phase III clinical trials. Keep in mind that at present we do not have a marker that will help select one regimen up front for clinical efficacy and or toxicity but the general consensus is to use a multi-drug regimen for patients with a good to marginal performance status or even a single agent in very frail patients.8,9
In 2011, the results of a phase III clinical trial demonstrated efficacy of 5-FU based combination therapy compared to single agent chemotherapy, at the expense of some increased toxicity.10 Since then, a multi-drug regimen approach has been shown to be effective.11 Today, the gemcitabine-based or 5-FU based treatments are recommended for patients with metastatic disease.12 Choice of treatment is based on overall assessment of the patient with regards to performance status, comorbidities, symptom burden, prior treatments, patient preference, goals of therapy and the patient’s home support system along with consideration of the potential side effects of the therapy.4,12
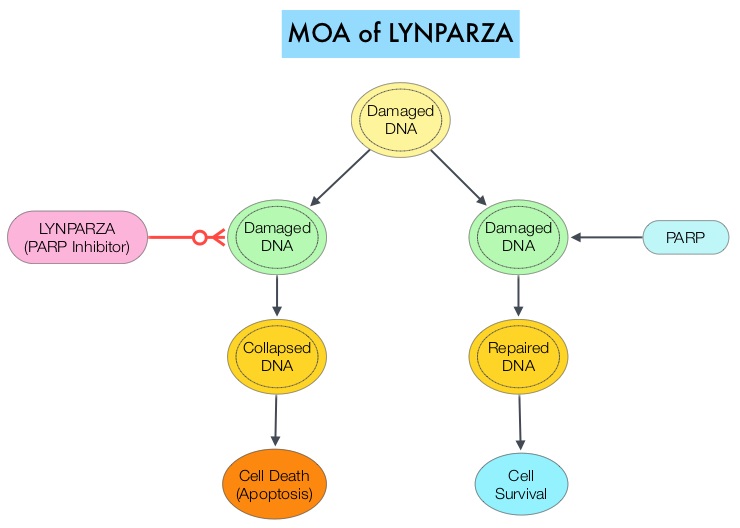
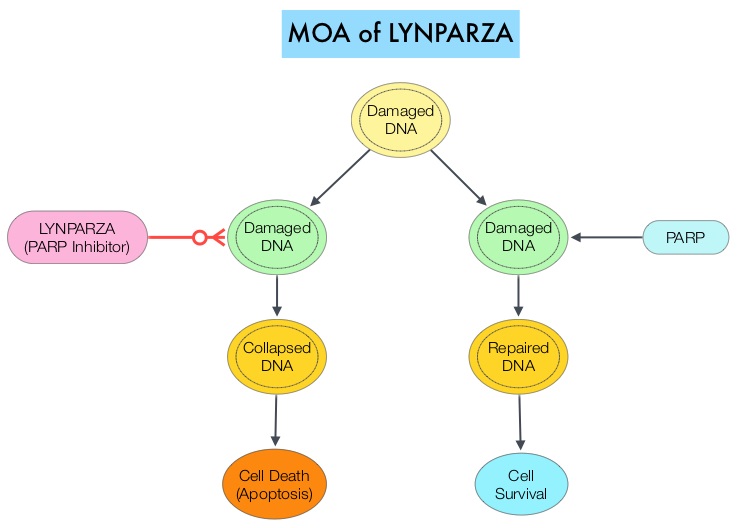
Once a patient begins treatment, close monitoring of the patient for evidence of disease progression is very important in order to offer patients second line chemotherapy. Thus, evaluation of the patient’s clinical status, restaging scans, and CA19-9 in a timely fashion will help guide the clinician on starting second line therapy.7,3 For patients with tumors that have a mutation in BRCA 1 or 2 gene (~7% of patients) maintenance with a PARP inhibitor, after receiving chemotherapy is recommended. Additional targeted agents are a possible treatment option if the tumors have presence of specific mutations.3,7
Despite advances, metastatic pancreatic cancer can be difficult to treat. The aggressive nature of the disease along with a high symptom burden make diligent patient management of the utmost importance, particularly during today’s challenging times. Recognizing and addressing symptoms proactively along with choosing the optimal treatment to allow for anti-tumor efficacy combined with a side effect profile that best fits the patient’s tolerance remains important.3,8,13
References
1. Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Cancer Res. 2014;74:2913-2921.
2. National Cancer Institute: Surveillance, Epidemiology, and End Results Program. https://seer.cancer.gov/statfacts/html/pancreas.html. Accessed November 2, 2020.
3. Mizrahi JD, Surana R, Valle JW, Shroff RT. Lancet. 2020;395:2008-2020.
4. Moffat GT, Epstein AS, O’Reilly EM. Cancer. 2019;125:3927-3935.
5. Benyon B. Oncology Nursing News. Published online March 31, 2020. https://www.oncnursingnews.com/web-exclusives/to-treat-or-not-to-treat-cancer-during-the-covid-19-pandemic. Accessed November 3, 2020.
6. Gilliland TMVillafane-Ferriol N, Shah KP, Shah RM, Tran Cao HS, Massarweh NN et al. Nutrients. 2017;9:243.
7. Sohal DPS, Kennedy EB, Cinar P, Conroy T, Copur MS, Crane CH et al. J Clin Oncol. 2020;38:3217-3230.
8. Sohal DPS, Mangu PB, Khorana AA, Shah MA, Philip PA, O’Reilly EM, et al. J Clin Oncol. 2016;34:2784-2796.
9. Zhang L, Sanagapalli S, Stoita A. World J Gastroenterol. 2018;24:2047-2060.
10. Conroy T, Desseigne FD, Ychou M, Bouche O, Guimbaud R, Becouarn Y et al. N Engl J Med. 2011;364:1817-1825.
11. Von Hoff DD, Ervin T, Areana FP, Chiorean EG, Infante J, Moore M et al. N Engl J Med. 2013;369:1691-1703.
12. Sohal DPS, Kennedy EB, Khorana A, Copur MS, Crane CH, Garrido-LagunaI et al. J Clin Oncol. 2018;36:2545-2556.
13. Catanese S, Pentheroudakis G, Douillard J-Y, Lordick F. ESMO Open. 2020;5:e000804.