SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2019, about 228,150 new cases of lung cancer will be diagnosed and 142,670 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions by switching off the T cells of the immune system.
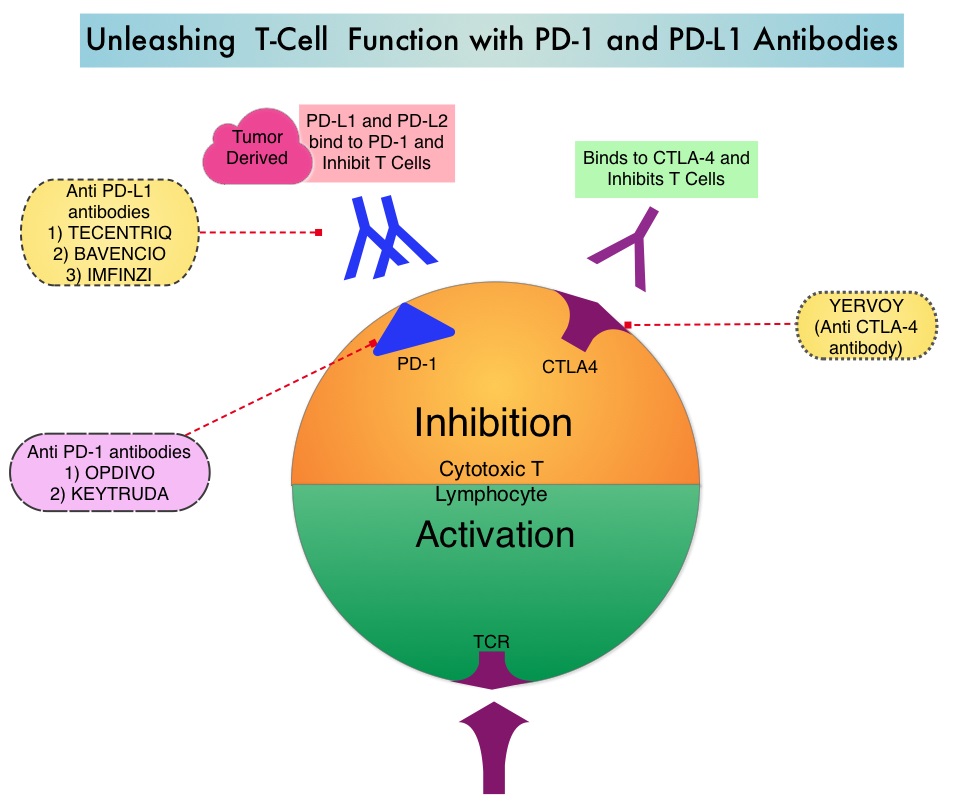
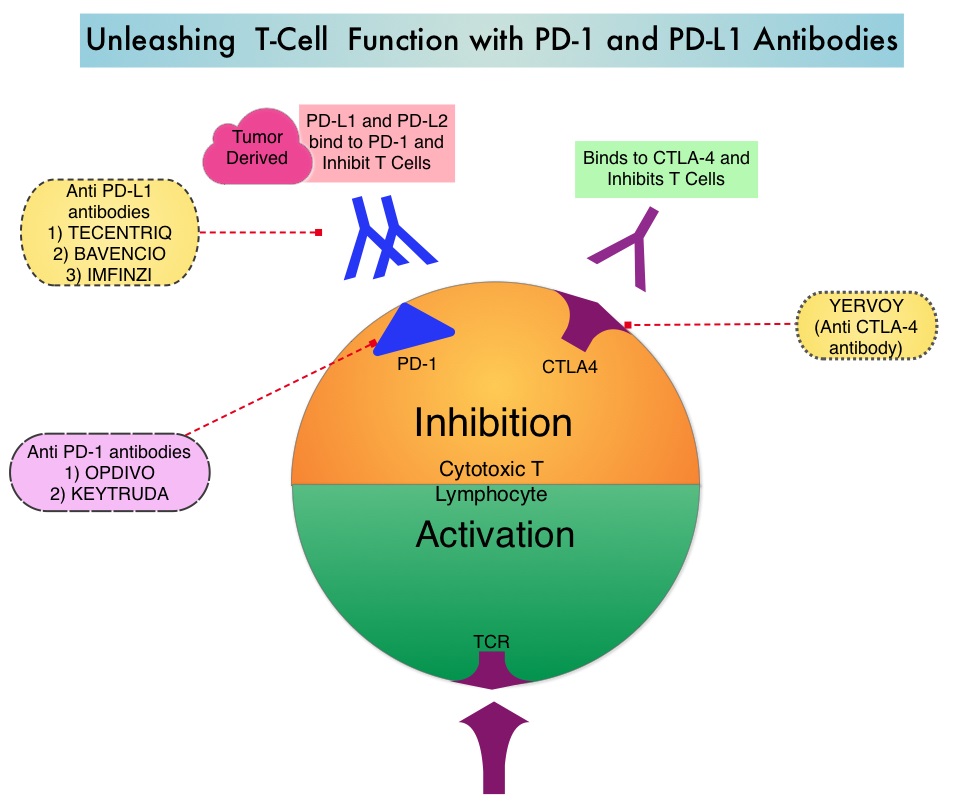
Immune checkpoint proteins/receptors include CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152) and PD-1(Programmed cell Death 1). Checkpoint inhibitors unleash the T cells resulting in T cell proliferation, activation, and a therapeutic response. OPDIVO® (Nivolumab) is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the T cells. OPDIVO® is presently approved for treatment of patients with metastatic NSCLC and progression on or after Platinum-based chemotherapy. YERVOY® is a fully human immunoglobulin G1 monoclonal antibody that blocks Immune checkpoint protein/receptor CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4).
CheckMate-227 is an open-label, multi-part, global, Phase III trial in which OPDIVO® based regimens were compared with Platinum-doublet chemotherapy in patients with first line advanced NSCLC, across non-squamous and squamous tumor histologies. In Part 1 of this trial, there were 2 cohorts- Part 1a in which OPDIVO® plus low dose YERVOY® (N=396) or OPDIVO® monotherapy (N=396) was compared with chemotherapy alone (N=397), in patients whose tumors expressed PD-L1 expression of 1% or more and Part 1b in which OPDIVO® plus low dose YERVOY® (N=187) or OPDIVO® plus chemotherapy (N=177) was compared with chemotherapy alone (N=186), in patients whose tumors did not express PD-L1 (less than 1%). (In Part 2 of this trial, OPDIVO® plus chemotherapy was compared with chemotherapy alone, regardless of PD-L1 expression. Part 2 did not meet its Primary endpoint for Overall Survival for OPDIVO® plus chemotherapy versus chemotherapy alone, in patients with non-squamous NSCLC, and is published elsewhere). It should be noted that when this trial was launched, chemotherapy along with immunotherapy or immunotherapy alone was not approved for the front-line treatment of NSCLC. Therefore, dual immunotherapy combination was not compared with current standards of care such as chemotherapy plus immunotherapy.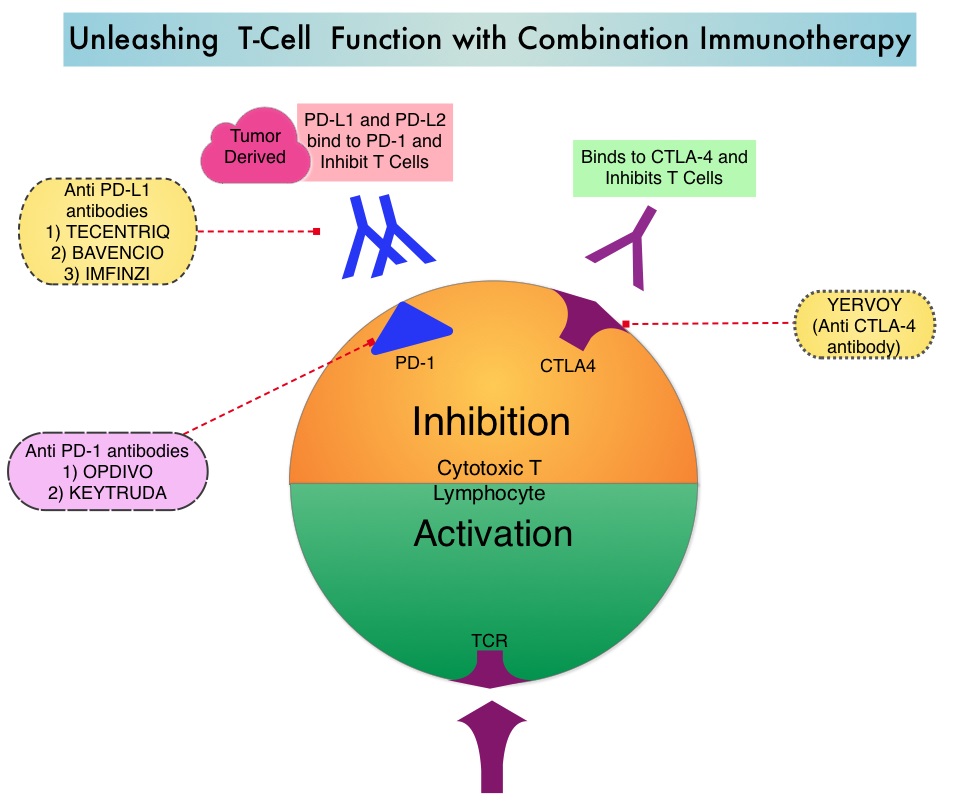
OPDIVO® was administered at 3 mg/kg every 2 weeks, and in the combination arm, YERVOY® was administered at 1 mg/kg every 6 weeks. When administered with chemotherapy, OPDIVO® was administered at 360 mg every 3 weeks. Patients were stratified by histology, and treatment was administered until disease progression, unacceptable toxicity, or for 2 years, for immunotherapy. There were two Co-primary endpoints in Part 1 for OPDIVO® plus YERVOY® versus chemotherapy: Overall survival (OS) in patients whose tumors express PD-L1 (assessed in patients enrolled in Part 1a) and Progression Free Survival (PFS) in patients with TMB of 10 mut/Mb or more, across the PD-L1 spectrum (assessed in patients enrolled across Parts 1a and 1b). The minimum follow up for the Primary endpoint was 29 months.
Both Part 1a and Part 1b groups met their Primary endpoints. In the Part 1a cohort with PD-L1 expression of 1% or more, the Overall Survival was significantly longer with OPDIVO® plus YERVOY®, compared to chemotherapy. The median Overall Survival was 17.1 months in the Immunotherapy combination group compared to 14.9 months in the chemotherapy group (HR=0.79; P=0.007). Progression Free Survival, Objective Response Rates and Duration of Response were all greater with OPDIVO® plus YERVOY® combination, compared to chemotherapy. In the Part 1b cohort with PD-L1 expression of less than 1%, Overall Survival benefit was again observed with the OPDIVO® plus YERVOY® combination, compared with chemotherapy. Grade 3 and 4 treatment-related Adverse Events across all patients was 33% in those treated with OPDIVO® plus YERVOY® combination, 19% with single agent OPDIVO® and 36% with chemotherapy.
It was concluded that first-line treatment of patients with advanced NSCLC with a combination of two immunotherapy drugs improves Overall Survival, compared to chemotherapy, and offers a chemotherapy-free first line treatment option for a subset of NSCLC patients, leaving chemotherapy for later lines of therapy. Nivolumab + low-dose ipilimumab versus platinum-doublet chemotherapy as first-line treatment for advanced non–small cell lung cancer: CheckMate-227 part 1 final analysis. Peters S, Ramalingam SS, Paz-Ares L, et al. Presented at 2019 ESMO Congress; September 27 to October 1, 2019; Barcelona, Spain. Abstract LBA4.