
The FDA on August 5, 2016 granted accelerated approval to KEYTRUDA® injection for the treatment of patients with recurrent or metastatic Head and Neck Squamous Cell Carcinoma (HNSCC) with disease progression on or after platinum-containing chemotherapy. KEYTRUDA® is a product of Merck Sharp & Dohme Corp.
Tag: Head & Neck: Lip and Oral Cavity
Detection of HPV DNA in the Oral Cavity Increases the Risk of Head and Neck Cancer
SUMMARY: The American Cancer Society estimates that 61,760 people will be diagnosed with Head and Neck cancer in 2016 and 13,190 patients will die of the disease. Over 90% of these malignancies are Squamous Cell Carcinomas (SCCs). Oropharyngeal Squamous Cell Carcinomas (OPSCC) involve the tonsils and base of the tongue and recent studies have shown that over 70% of these tumors are caused by Human Papilloma Virus (HPV) and HPV-16 is the predominant type present in the tumor cells. The CDC estimates that more than 2,370 new cases of Human Papilloma Virus associated Oropharyngeal Squamous Cell Carcinomas (OPSCC) are diagnosed in women and nearly 9,356 are diagnosed in men, each year in the United States and this incidence has been on the rise. The malignant behavior of these tumors is dependent on the expression of viral E6 and E7 oncoproteins that inactivate the tumor suppressor proteins p53 and the retinoblastoma protein (pRb), respectively. HPV-positive OroPharyngeal Squamous Cell Carcinoma is more common among never smokers or light smokers and patients tend to be younger with better performance status.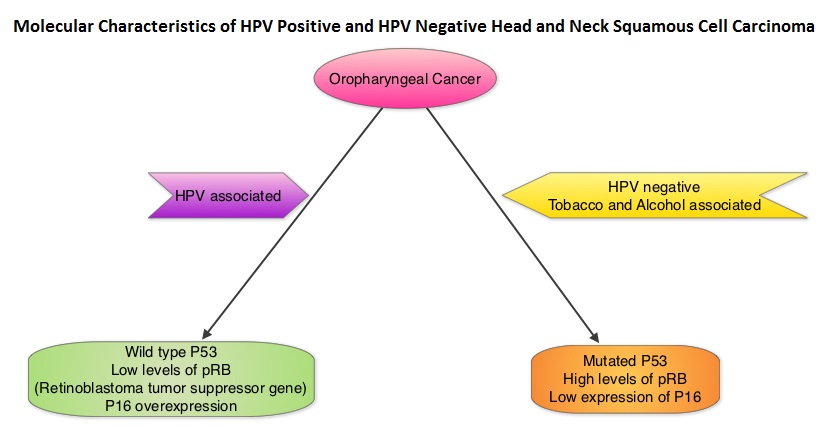
The authors conducted this prospective study to examine the temporal association between HPV DNA detection of alpha, beta and gamma Human Papilloma Virus (HPV) types in the oral samples and risk of Head and Neck Squamous Cell Carcinoma (HNSCC). A nested case-control study was carried out among 96,650 participants, cancer free at baseline, who provided mouthwash samples in 2 large prospective cohorts: the American Cancer Society Cancer Prevention Study II Nutrition Cohort and the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial (PLCO). Molecular Detection of DNA from alpha, beta and gamma HPV types in mouthwash samples was performed by next-generation sequencing method. Associations between oral HPV infection and Head and Neck Squamous Cell Carcinoma (HNSCC) were adjusted for smoking status, pack-years and number of alcoholic drinks per week, which are all known and established risk factors for HNSCC.
During an average follow up of 3.9 years in both cohorts, 132 cases of HNSCC were identified which included cancers of the Oropharynx, Oral cavity and Larynx. The authors after analyzing the 132 cases of HNSCC and 396 controls nested within 2 prospective cohorts, found that detection of oral HPV-16 DNA was associated with a 22.4 fold increased risk of incident Oropharyngeal Cancer. Detection of oral beta1-HPV-5 type and gamma11-HPV and gamma12-HPV species was associated with a 3.3 to 5.5 fold higher risk of HNSCC.
The authors concluded that HPV-16 detection in the oral cavity precedes the incidence of Oropharyngeal Squamous Cell Carcinoma and this is the first study to demonstrate a temporal association between HPV DNA detection in mouthwash specimens and risk of HNSCC. Further, other HPVs including beta and gamma species may also play a role in the etiology of HNSCC. Detection of HPV DNA in the oral cavity may have important implications for its use in Oropharygeal cancer screening program. Associations of Oral α-, β-, and γ-Human Papillomavirus Types with Risk of Incident Head and Neck Cancer. Agalliu I, Gapstur S, Chen Z, et al. JAMA Oncol. 2016;2:599-606
OPDIVO® Granted Breakthrough Designation by FDA for Head and Neck cancer
SUMMARY: The FDA granted breakthrough therapy designation to Nivolumab (OPDIVO®), as a treatment for patients with recurrent or metastatic Squamous Cell Carcinoma of the Head and Neck (SCCHN), following a platinum based therapy. This designation was based on the findings from CheckMate-141 study, which demonstrated an improvement in Overall Survival (OS) with OPDIVO®, compared to investigator’s choice of therapy. The American Cancer Society estimates that 61,760 people will be diagnosed with Head and Neck cancer in 2016 and 13,190 patients will die of the disease. Patients with recurrent/metastatic Squamous Cell Carcinoma of the Head and Neck (SCCHN) have a poor prognosis with a median Overall Survival (OS) of about 13 months with first line therapy and about 6 months or less with later lines of therapy. The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of the Immune checkpoints or gate keepers. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent related to their ability to escape immune surveillance by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response.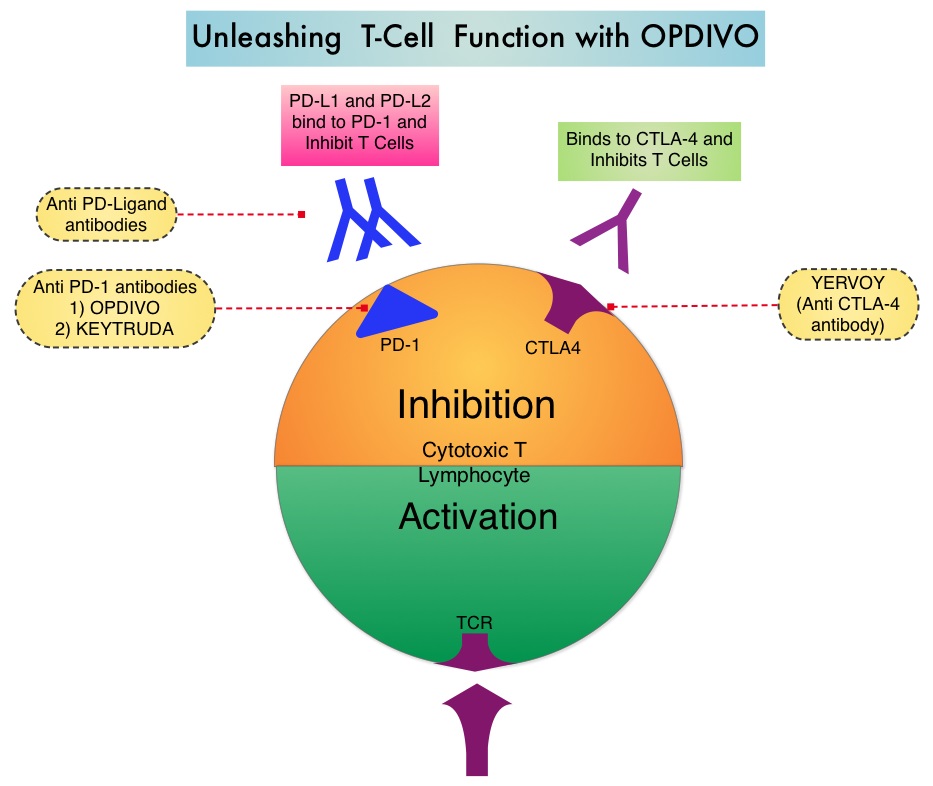
OPDIVO® is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response. CheckMate-141 is an open-label, phase III trial, in which 361 patients with recurrent or metastatic Squamous Cell Carcinoma of the oral cavity, pharynx, or larynx, were randomly assigned in a 2:1 ratio to receive either OPDIVO® (N= 240) or investigator’s choice of ERBITUX® (Cetuximab), TAXOTERE® (Docetaxel) or Methotrexate (N=121). OPDIVO® was administered intravenously at 3 mg/kg every 2 weeks. ERBITUX® dosing was 400 mg/m2 for the first dose followed by 250 mg/m2 weekly, TAXOTERE® dosing was 30 mg/m2 weekly and Methotrexate dosing was 40 mg/m2 weekly. The median age was 60 years, majority of patients were male, had received 2 or more prior systemic therapies and prior radiation therapy. Patients were stratified based on prior therapy with monoclonal antibody, ERBITUX® and HPV status was known for 50% of the participants. The primary endpoint was Overall Survival and secondary endpoints included Response Rates and Progression Free Survival (PFS).
This study was stopped earlier than scheduled after an independent monitoring panel determined that the primary endpoint for this study was met, with significant superiority of OPDIVO® over the investigator’s choice of therapy. The median Overall Survival with OPDIVO® was 7.5 months, compared to 5.1 months with investigator’s choice of therapy (HR=0.70; P=0.010). The 1-year Overall Survival with OPDIVO® was 36%, which was more than double, compared with investigator’s choice of therapy, which was 16.6%. Patients with PD-L1 expression of 1% or more benefited the most from treatment with OPDIVO®, with a median OS of 8.7 months, compared to 4.6 months in the control group (HR=0.55). For patients with PD-L1 expression less than 1%, median OS was 5.7 with OPDIVO® versus 5.8 months, for the control group (HR=0.89). HPV status also had an impact on outcomes. HPV-positive patients had a median OS of 9.1 months with OPDIVO® compared with 4.4 months with investigator’s choice of therapy (HR=0.56), whereas those who were HPV-negative and receiving OPDIVO®, had a median OS of 7.5 months compared to 5.8 months with investigator’s choice of therapy (HR=0.73). Grade 3 or 4 adverse events were significantly lower with OPDIVO®, compared with investigator’s choice of therapy(13.1% vs 35.1%).
The authors concluded that OPDIVO® is the first agent to demonstrate a significant improvement in Overall Survival, in patients with advanced head and neck cancer following progression on platinum-based chemotherapy, and fulfills an unmet need for this patient group. Gillison ML, Blumenschein G, Fayette J, et al. Nivolumab Versus Investigator’s Choice (IC) for Recurrent or Metastatic (R/M) Head and Neck Squamous Cell Carcinoma (SCCHN): CheckMate-141. Presented at: AACR 2016 Annual Meeting, New Orleans; April 16-20, 2016. Abstract CT099.
Late Breaking Abstract – ASCO 2015 Elective Neck Dissection Improves Overall Survival and Disease Free Survival in Early Oral Cavity Cancers
SUMMARY: The American Cancer Society estimates that approximately 39,500 individuals will be diagnosed with oral cavity and oropharyngeal cancer in the United States in 2015 and about 7,500 will die of the disease. These cancers are more than twice as common in men as in women and tobacco and alcohol use are among the strongest risk factors. Routinely screening for oral mucosal lesions can improve survival in this patient group. The primary treatment of oral cavity squamous cell carcinoma is complete surgical resection with tumor free margins. Surgical management of the neck in patients with early stage oral cancers has remained unclear, with regards to the benefit of ipsilateral Elective Neck Dissection (END) at the time of primary surgery following diagnosis versus Therapeutic Neck Dissection (TND) after nodal relapse in the neck. To address this question, the authors conducted a prospective, randomized, controlled trial between 2004 and 2014, in which 596 treatment naïve patients with invasive squamous cell carcinoma of the oral cavity (tongue-85%, buccal mucosa-14%, floor of the mouth-1%) were enrolled and randomized to 1:1 to Elective Neck Dissection (END) or Therapeutic Neck Dissection (TND) following primary oral surgery. Patients had T1 (2 cm or less) or T2 (more than 2 cm and less than 4 cm) tumors that was lateralized to one side of the midline and were amenable to oral excision with adequate margins. Elective Neck Dissection (END) consisted of removal of submandibular (level 1), upper jugular (level 2)and midjugular (level 3) lymph nodes, with lower jugular (level 4) and posterior triangle (level 5) lymph nodes removed only if any of the lymph nodes in the first three levels showed intraoperative metastatic disease. Therapeutic Neck Dissection (TND) consisted of modified neck dissection (level 1-5) at the time of nodal relapse. All patients with high risk disease received adjuvant radiotherapy. The Primary end point was Overall Survival and Secondary end point was Disease Free Survival.
This publication summarizes the outcomes for the first 500 patients (245 in the END group and 255 in the TND group), following a median follow-up of 39 months. The 3 year Overall Survival was significantly higher in the Elective Neck Dissection group compared with the Therapeutic Neck Dissection group (80.0% vs. 67.5%, HR=0.63; P=0.01). The three year Disease Free Survival was also significantly higher in the END arm compared with TND (69.5% vs 45.9%, HR=0.45; P<0.001). The authors concluded that Elective Neck Dissection in patients with early stage oral squamous cell carcinoma resulted in 37% reduction in mortality risk as well as significantly high Disease Free Survival rates with a 55% reduction in the risk of disease recurrence. END should therefore be considered a standard treatment option. Elective versus Therapeutic Neck Dissection in Node-Negative Oral Cancer. D’Cruz AK, Vaish R, Kapre N, et al. N Engl J Med 2015; 373:521-529
p16 Protein Expression and Human Papillomavirus Status As Prognostic Biomarkers of Non-Oropharyngeal Head and Neck Squamous Cell Carcinoma
SUMMARY: Squamous Cell Carcinoma of the Head and Neck (HNSCC) accounts for about 3-5% of all cancers in the United States. It is estimated that 55,070 people were diagnosed with Head and Neck cancer in 2014 and 12,000 patients died of the disease. The head and neck region includes the oral cavity, oropharynx, hypopharynx and larynx. Squamous Cell Carcinoma involving the head and neck region (HNSCC) is therefore a heterogeneous disease and the five year survival rate of patients with head and neck cancer depends on several factors and can be variable. Common risk factors include tobacco and alcohol use and Human PapillomaVirus (HPV) infection. Recent studies have shown that over 70% of the OroPharyngeal Squamous Cell Carcinomas (OPSCC) are caused by HPV with the HPV-16 being the predominant type present in the tumor cells.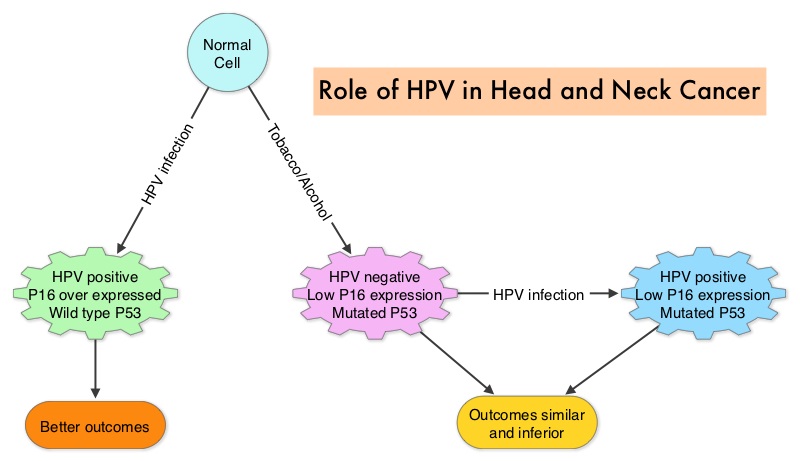 The malignant behavior of these tumors is dependent on the expression of viral E6 and E7 oncoproteins that inactivate the tumor suppressor proteins p53 and the retinoblastoma protein (pRB), respectively. HPV positive OroPharyngeal Squamous Cell Carcinoma (OPSCC) is more common among never smokers or light smokers and patients tend to be younger with better performance status. The pathobiology of HPV positive OroPharyngeal Squamous Cell Carcinoma (OPSCC) is different from the HPV negative OroPharyngeal Squamous Cell Carcinoma in that p53 is degraded/inactivated by viral E6 oncoprotein instead of by genetic mutation, pRB pathway is inactivated by viral E7 oncoprotein instead of Cyclin D1 amplification and p16 is overexpressed or upregulated instead of inactivation resulting from reduced negative feedback from pRB. Testing for HPV is based on several methodologies which include detection of HPV DNA by in situ hybridization (ISH) or Polymerase Chain Reaction (PCR), detection of HPV E6/E7 RNA expression by quantitative Reverse Transcriptase–PCR (qRT-PCR) and p16 protein overexpression, a surrogate marker of oncogenic HPV infection, by ImmunoHistoChemistry (IHC) staining. Both p16 overexpression testing by IHC and HPV by ISH can be easily performed on Formalin-Fixed Paraffin Embedded (FFPE) specimen whereas detection of HPV E6/E7 RNA expression, which is indicative of active viral oncogene transcription in tumor cells and is considered to be a gold standard, requires a larger tumor specimen compared with other methodologies.
The malignant behavior of these tumors is dependent on the expression of viral E6 and E7 oncoproteins that inactivate the tumor suppressor proteins p53 and the retinoblastoma protein (pRB), respectively. HPV positive OroPharyngeal Squamous Cell Carcinoma (OPSCC) is more common among never smokers or light smokers and patients tend to be younger with better performance status. The pathobiology of HPV positive OroPharyngeal Squamous Cell Carcinoma (OPSCC) is different from the HPV negative OroPharyngeal Squamous Cell Carcinoma in that p53 is degraded/inactivated by viral E6 oncoprotein instead of by genetic mutation, pRB pathway is inactivated by viral E7 oncoprotein instead of Cyclin D1 amplification and p16 is overexpressed or upregulated instead of inactivation resulting from reduced negative feedback from pRB. Testing for HPV is based on several methodologies which include detection of HPV DNA by in situ hybridization (ISH) or Polymerase Chain Reaction (PCR), detection of HPV E6/E7 RNA expression by quantitative Reverse Transcriptase–PCR (qRT-PCR) and p16 protein overexpression, a surrogate marker of oncogenic HPV infection, by ImmunoHistoChemistry (IHC) staining. Both p16 overexpression testing by IHC and HPV by ISH can be easily performed on Formalin-Fixed Paraffin Embedded (FFPE) specimen whereas detection of HPV E6/E7 RNA expression, which is indicative of active viral oncogene transcription in tumor cells and is considered to be a gold standard, requires a larger tumor specimen compared with other methodologies.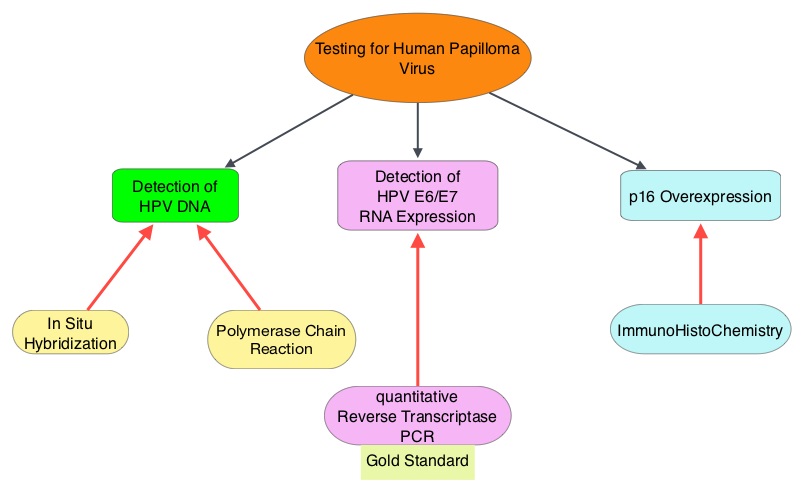 The concordance rate between HPV by ISH and p16 by IHC is approximately 90% in OPSCC, whereas the prevalence and significance p16 by IHC has remained unclear for HPV infection in non-OPSCC (oral cavity, hypopharynx and larynx). It is well established however that patients with HPV-positive/p16-positive OPSCC have better outcomes compared with those with HPV-negative/p16-negative OPSCC. However, the prognostic significance of p16 overexpression in non-OPSCC patients with or without evidence of HPV infection has not been clear. The authors in this study evaluated p16 protein overexpression by IHC and HPV status by HPV ISH as potential prognostic biomarkers in non-OPSCC tumors of patients enrolled in three prospective Radiation Therapy Oncology Group (RTOG) clinical trials. Of the 1921 patient enrolled in these three trials, 683 patients with non-OPSCC tumors were eligible and 52% (N=356) of these patients were tested for p16 overexpression and overall, 19.3% were p16 positive. When OPSCC and non-OPSCC patients were compared, OPSCC patients whose tumors were p16 positive had better Progression Free Survival and Overall Survival than non-OPSCC patients with p16 positive tumors. However, patients with p16 negative OPSCC and non-OPSCC have similar inferior outcomes. The authors concluded that patients with p16 negative non-OPSCC have worse outcomes than patients with p16 positive non-OPSCC, similar to that seen in patients with OPSCC and therefore HPV infection may influence outcomes in a subset of patients with non-OPSCC as well. Better methodologies for HPV detection and correlation with p16 expression will help identify “true” HPV infection related non-OPSCC and thereby enable tailored and less intense treatment, for this favorable group of patients. Chung CH, Zhang Q, Kong CS, et al. J Clin Oncol 2014; 32:3930-3938
The concordance rate between HPV by ISH and p16 by IHC is approximately 90% in OPSCC, whereas the prevalence and significance p16 by IHC has remained unclear for HPV infection in non-OPSCC (oral cavity, hypopharynx and larynx). It is well established however that patients with HPV-positive/p16-positive OPSCC have better outcomes compared with those with HPV-negative/p16-negative OPSCC. However, the prognostic significance of p16 overexpression in non-OPSCC patients with or without evidence of HPV infection has not been clear. The authors in this study evaluated p16 protein overexpression by IHC and HPV status by HPV ISH as potential prognostic biomarkers in non-OPSCC tumors of patients enrolled in three prospective Radiation Therapy Oncology Group (RTOG) clinical trials. Of the 1921 patient enrolled in these three trials, 683 patients with non-OPSCC tumors were eligible and 52% (N=356) of these patients were tested for p16 overexpression and overall, 19.3% were p16 positive. When OPSCC and non-OPSCC patients were compared, OPSCC patients whose tumors were p16 positive had better Progression Free Survival and Overall Survival than non-OPSCC patients with p16 positive tumors. However, patients with p16 negative OPSCC and non-OPSCC have similar inferior outcomes. The authors concluded that patients with p16 negative non-OPSCC have worse outcomes than patients with p16 positive non-OPSCC, similar to that seen in patients with OPSCC and therefore HPV infection may influence outcomes in a subset of patients with non-OPSCC as well. Better methodologies for HPV detection and correlation with p16 expression will help identify “true” HPV infection related non-OPSCC and thereby enable tailored and less intense treatment, for this favorable group of patients. Chung CH, Zhang Q, Kong CS, et al. J Clin Oncol 2014; 32:3930-3938