
The FDA on June 12, 2025, approved KEYTRUDA® for adults with resectable locally advanced Head and Neck Squamous Cell Carcinoma (HNSCC) whose tumors express PD-L1 [Combined Positive Score (CPS) ≥1] as determined by an FDA-approved test, as a single agent as neoadjuvant treatment, continued as adjuvant treatment in combination with Radiotherapy (RT) with or without Cisplatin after surgery, and then as a single agent. KEYTRUDA® is a product of Merck.
Tag: Head & Neck: Lip and Oral Cavity
FDA Approves Perioperative KEYTRUDA® for Resectable Locally Advanced Head and Neck Squamous Cell Carcinoma
SUMMARY: The FDA on June 12, 2025, approved Pembrolizumab (KEYTRUDA®) for adults with resectable locally advanced Head and Neck Squamous Cell Carcinoma (HNSCC) whose tumors express PD-L1 Combined Positive Score (CPS) of 1 or more, as determined by an FDA-approved test, as a single agent as neoadjuvant treatment, continued as adjuvant treatment in combination with Radiotherapy (RT) with or without Cisplatin after surgery, and then as a single agent.This is the first approval for HNSCC in 6 years and the first overall perioperative approval for locally advanced HNSCC.
The American Cancer Society estimates that 59,660 new cases of cancer involving the oral cavity and pharynx will be diagnosed in the US in 2025 and 12,770 will die of the disease. The Head and Neck region includes the oral cavity, oropharynx, hypopharynx and larynx. Squamous Cell Carcinoma (SCC) of the Head and Neck accounts for about 3-5% of all cancers in the United States. Common risk factors include tobacco and alcohol use and Human PapillomaVirus (HPV) infection. Even though tobacco has long been associated with head and neck cancer development, cannabis has similar carcinogens.
The Standard of Care for patients with Stage III–IVA Head and Neck Squamous Cell Carcinoma (HNSCC) has remained largely static for nearly 2 decades: surgery followed by risk-adapted adjuvant radiotherapy, with or without concurrent chemotherapy. Despite refinements in technique and supportive care, relapse rates remain high, particularly among patients with adverse pathological features such as extranodal extension and positive margins.
The treatment paradigm for Head and Neck cancer has been rapidly evolving with the recognition and better understanding of immune evasion and the role of immune checkpoints or gate keepers in suppressing antitumor immunity. Blocking the immune checkpoints unleashes the T cells, resulting in T cell proliferation, activation, and a therapeutic response. Checkpoint inhibitors administered in a neoadjuvant setting activates both the priming phase of immunity within tumor tissue, and the effector phase within the tumor microenvironment. It has been shown that neoadjuvant immunotherapy expands more T-cell clones than adjuvant treatment. Preclinical models have also demonstrated that both radiation therapy and Cisplatin chemotherapy increase the PD-L1 expression on the tumor, suggesting that combining radiotherapy with anti-PD-1 therapy could improve the outcomes.
Pembrolizumab (KEYTRUDA®) is a fully humanized, Immunoglobulin G4, monoclonal antibody and checkpoint inhibitor, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. Pembrolizumab has been shown to improve Overall Survival in patients with Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma
KEYNOTE-689, a landmark Phase 3 trial, has provided the most compelling evidence to date that perioperative immunotherapy, specifically Pembrolizumab, can significantly improve clinical outcomes for patients with resectable, locally advanced Head and Neck Squamous Cell Carcinoma (HNSCC). This international, randomized, placebo-controlled study enrolled 714 patients (N=714) with newly diagnosed, resectable, Stage III–IVA HNSCC of the oral cavity, oropharynx, larynx, or hypopharynx.
Patients were randomized 1:1 to receive:
- Investigational arm (N=356):
- 2 cycles of neoadjuvant Pembrolizumab (200 mg IV Q3W) starting about 3 weeks before surgery.
- Standard-of-care surgery.
- Up to 3 doses of Pembrolizumab administered concurrently with adjuvant chemoradiotherapy, with Cisplatin (depending on pathologic risk- positive margins <1 mm or extranodal extension present at surgery was considered high risk).
- 12 additional adjuvant doses of Pembrolizumab Q3W (total treatment duration: about 1 year).
- Control arm (N=358):
- Identical treatment structure, substituting placebo for Pembrolizumab.
PD-L1 expression was assessed via Combined Positive Score (CPS), and stratification included CPS ≥1 and CPS ≥10 subgroups, recognizing the prognostic and potentially predictive value of PD-L1 expression. The Primary endpoint was Event-Free Survival (EFS) by Blinded Independent Central Review, defined as time from randomization to disease progression, local/regional recurrence, distant metastasis, or death from any cause. Secondary endpoints included Overall Survival (OS) and Major Pathological Response.
The trial met its Primary endpoint of EFS. At median follow-up of 38.3 months, patients in the investigational arm had significantly improved EFS compared with the Standard of Care arm (median 51.8 months vs. 30.4 months; HR=0.73; P=0.0041). Patients who received Pembrolizumab who had a CPS score ≥10 derived the greatest benefit (median 59.7 months vs. 26.9 months; HR = 0.66; P=0.002) whereas the median EFS in the CPS ≥1 subgroup was 59.7 vs. 29.6 months (HR, 0.70; P = .0014).
Major pathological response defined as 90% or more tumor regression was also notably improved. Among all patients, the major pathological response rate was 9.4% with Pembrolizumab vs. 0% with Standard of Care (P < 0.00001). In the CPS ≥10 subgroup, the major pathological response rate reached 13.7%.
While the interim analysis did not demonstrate a statistically significant OS benefit, trends were favorable, particularly in the CPS ≥10 group (HR, 0.72; P =0.02). Further OS follow-up is ongoing.
Adverse events were consistent with known profiles of checkpoint inhibitors. Grade 3 or more Treatment-Related Adverse Events (TRAEs) occurred in 44.6% of the Pembrolizumab group and 42.9% in the Standard of Care group. Immune-mediated adverse events were observed in 43.2% of the Pembrolizumab arm, with hypothyroidism being the most common (24.7%). Mortality attributable to treatment was slightly higher with Pembrolizumab (1.1% vs. 0.3%).
The researchers concluded that perioperative Pembrolizumab is now emerging as a new standard of care in the treatment of resectable locally advanced HNSCC. The findings from this study underscore the importance of harnessing the immune system both before and after surgery. Neoadjuvant administration may prime the immune response when tumor antigen burden is highest, while adjuvant therapy may help eliminate residual microscopic disease.
Neoadjuvant and adjuvant pembrolizumab plus standard of care in resectable locally advanced head and neck squamous cell carcinoma: phase 3 KEYNOTE-689 study. Uppaluri R, et al. Abstract CT001. Presented at: American Association for Cancer Research Annual Meeting; April 25-30, 2025; Chicago.
Late Breaking Abstract – ASCO 2025: A New Era for High-Risk Resected Head and Neck Cancer: Nivolumab Adds Disease-Free Survival Benefit in NIVOPOSTOP Trial
SUMMARY: The American Cancer Society estimates that 59,660 new cases of cancer involving the oral cavity and pharynx will be diagnosed in the US in 2025 and 12,770 will die of the disease. The head and neck region includes the oral cavity, oropharynx, hypopharynx and larynx. Squamous Cell Carcinoma (SCC) of the Head and Neck accounts for about 3-5% of all cancers in the United States. Common risk factors include tobacco and alcohol use and Human PapillomaVirus (HPV) infection. Even though tobacco has long been associated with head and neck cancer development, cannabis has similar carcinogens.
The Standard of Care for patients with Stage III–IVA Head and Neck Squamous Cell Carcinoma (HNSCC) has remained largely static for nearly 2 decades: surgery followed by risk-adapted adjuvant radiotherapy, with or without concurrent Cisplatin based chemotherapy. Despite refinements in technique and supportive care, relapse rates remain high, particularly among patients with adverse pathological features such as extranodal extension and positive margins.
The treatment paradigm for Head and Neck cancer has been rapidly evolving with the recognition and better understanding of immune evasion and the role of immune checkpoints or gate keepers in suppressing antitumor immunity. Blocking the immune checkpoints unleashes the T cells, resulting in T cell proliferation, activation, and a therapeutic response. Checkpoint inhibitors administered in a neoadjuvant setting activates both the priming phase of immunity within tumor tissue, and the effector phase within the tumor microenvironment. It has been shown that neoadjuvant immunotherapy expands more T-cell clones than adjuvant treatment. Preclinical models have also demonstrated that both radiation therapy and Cisplatin chemotherapy increase the PD-L1 expression on the tumor, suggesting that combining radiotherapy with anti-PD-1 therapy could improve the outcomes.
Phase 3 NIVOPOSTOP trial (GORTEC 2018-01) provides compelling evidence that integrating immunotherapy into the adjuvant setting may finally shift this long-standing treatment landscape. Nivolumab (OPDIVO®) is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2. Blocking the Immune checkpoint proteins unleashes the T cells, resulting in T cell proliferation, activation and a therapeutic response.
Study Design and Patient Population
NIVOPOSTOP (NCT03576417) was an international, randomized, open-label Phase 3 study that enrolled 680 patients with completely resected LA-SCCHN (Locally Advanced Squamous Cell Carcinoma of the Head and Neck), which included the oral cavity, oropharynx, hypopharynx, and larynx. Eligible patients were less than 75 years old, with ECOG performance status 0-1, and exhibited high-risk features for recurrence, including extracapsular nodal extension, positive surgical margins, involvement of 4 or more lymph nodes, or extensive perineural invasion. PD-L1 expression was not required for study eligibility. Majority of patients had disease of the oral cavity (58%), about 50% were current smokers, most patients had Stage IVA or IVB disease (83%), and slightly more than one-half of patients (56%) had a PD-L1 Combined Positive Score less than 20. Patients were first stratified by HPV status and enrolling center before being randomly assigned to receive standard CRT or standard CRT plus nivolumab.
Patients were randomized 1:1 to receive:
- Control Arm (SOC CRT): 66 Gy radiotherapy with three cycles of Cisplatin 100 mg/m² Q3W (N=334).
- Experimental Arm (NIVO + CRT): One lead-in dose of Nivolumab 240 mg, followed by CRT plus Nivolumab 360 mg Q3W for three cycles, followed by six cycles of Nivolumab 480 mg Q4W for maintenance (N=332).
Both treatment groups were well balanced. The Primary endpoint was Disease Free Survival (DFS). Key Secondary endpoints include Overall Survival (OS) and Safety.
Primary Endpoint Met: Significant Improvement in Disease-Free Survival
At a median follow-up of 30.3 months, the trial met its Primary endpoint. Among the 666 patients included in the Disease-Free Survival (DFS) analysis (ITT population), the addition of adjuvant Nivolumab significantly reduced the risk of disease recurrence or death compared with CRT alone (HR 0.76; 95% CI, 0.60–0.98; P = 0.034).
Three-year DFS rates were 63.1% with NIVO + CRT (95% CI, 57.0–68.7) and 52.5% with CRT alone (95% CI, 46.2–58.4). This represents a 24% relative reduction in recurrence risk with Nivolumab. Importantly, this benefit was observed across all PD-L1 expression levels, supporting the use of this strategy in an unselected population.
Safety Profile: Manageable Toxicity with Increased Grade 3–4 Events
While the addition of Nivolumab was associated with an increase in grade 3-4 adverse events, particularly within the first 100 days post-CRT (13.1% vs. 5.6%), no increase in treatment-related mortality was seen (0.6% vs. 0.7%). Late grade ≥3 toxicities occurring beyond 9 months were rare in both groups and did not exceed grade 3. The overall safety profile was considered acceptable and consistent with known immune-related toxicities.
Locoregional Control Improved with Nivolumab
One of the most noteworthy findings was a significant reduction in locoregional recurrences. At 3 years, locoregional failure occurred in 13% of patients in the NIVO + CRT arm versus 20% in the CRT-only arm (HR 0.63; 95% CI, 0.42–0.94). Interestingly, unlike perioperative immunotherapy regimens such as KEYNOTE-689 that predominantly reduced distant failures, NIVOPOSTOP’s benefit was concentrated in locoregional disease control, suggesting a synergistic effect between radiotherapy and immune checkpoint inhibition.
Survival Data Pending but Trending Favorably
Although Overall Survival (OS) data remain immature, early trends favor the Nivolumab arm. At the time of reporting, 74% of patients receiving NIVO + CRT remained alive at 3 years, compared to 68% in the CRT-alone group. The final OS analysis is planned upon reaching 283 events (currently at 158).
Clinical Context and Expert Perspectives
The NIVOPOSTOP findings stand in sharp contrast to prior trials like KEYNOTE-412 and JAVELIN Head and Neck 100, which failed to show benefit from concurrent immune checkpoint inhibitor with CRT in unselected populations. Notably, the timing and sequencing of immunotherapy in NIVOPOSTOP, administered in the postoperative setting and continued as maintenance may have circumvented the immunosuppressive milieu of CRT and allowed more robust immune priming. The researchers emphasized the clinical need among the ~40–45% of LA-SCCHN patients who relapse after surgery and CRT.
Conclusion
NIVOPOSTOP represents the first successful Phase 3 trial to demonstrate a Disease-Free Survival advantage with the addition of immunotherapy to adjuvant CRT in high-risk, resected LA-SCCHN. With a favorable balance of efficacy and manageable toxicity, this regimen is poised to reshape clinical practice, marking a long-overdue advancement in the postoperative management of head and neck cancer.
NIVOPOSTOP (GORTEC 2018-01): A phase III randomized trial of adjuvant nivolumab added to radio-chemotherapy in patients with resected head and neck squamous cell carcinoma at high risk of relapse. Bourhis J, Auperin A, Borel C, et al. J Clin Oncol 43, 2025 (suppl 17; abstr LBA2).
Perioperative KEYTRUDA® Reshapes the Treatment Landscape for Resectable Locally Advanced HNSCC
SUMMARY: The American Cancer Society estimates that 59,660 new cases of cancer involving the oral cavity and pharynx will be diagnosed in the US in 2025 and 12,770 will die of the disease. The head and neck region includes the oral cavity, oropharynx, hypopharynx and larynx. Squamous Cell Carcinoma (SCC) of the Head and Neck accounts for about 3-5% of all cancers in the United States. Common risk factors include tobacco and alcohol use and Human PapillomaVirus (HPV) infection. Even though tobacco has long been associated with head and neck cancer development, cannabis has similar carcinogens.
The Standard of Care for patients with Stage III–IVA Head and Neck Squamous Cell Carcinoma (HNSCC) has remained largely static for nearly 2 decades: surgery followed by risk-adapted adjuvant radiotherapy, with or without concurrent chemotherapy. Despite refinements in technique and supportive care, relapse rates remain high, particularly among patients with adverse pathological features such as extranodal extension and positive margins.
The treatment paradigm for Head and Neck cancer has been rapidly evolving with the recognition and better understanding of immune evasion and the role of immune checkpoints or gate keepers in suppressing antitumor immunity. Blocking the immune checkpoints unleashes the T cells, resulting in T cell proliferation, activation, and a therapeutic response. Checkpoint inhibitors administered in a neoadjuvant setting activates both the priming phase of immunity within tumor tissue, and the effector phase within the tumor microenvironment. It has been shown that neoadjuvant immunotherapy expands more T-cell clones than adjuvant treatment. Preclinical models have also demonstrated that both radiation therapy and Cisplatin chemotherapy increase the PD-L1 expression on the tumor, suggesting that combining radiotherapy with anti-PD-1 therapy could improve the outcomes.
Pembrolizumab (KEYTRUDA®) is a fully humanized, Immunoglobulin G4, monoclonal antibody and checkpoint inhibitor, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. Pembrolizumab has been shown to improve Overall Survival in patients with Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma
KEYNOTE-689, a landmark Phase 3 trial, has provided the most compelling evidence to date that perioperative immunotherapy, specifically Pembrolizumab, can significantly improve clinical outcomes for patients with resectable, locally advanced Head and Neck Squamous Cell Carcinoma (HNSCC). This international, randomized, placebo-controlled study enrolled 714 patients (N=714) with newly diagnosed, resectable, Stage III–IVA HNSCC of the oral cavity, oropharynx, larynx, or hypopharynx.
Patients were randomized 1:1 to receive:
- Investigational arm (N=356):
- 2 cycles of neoadjuvant Pembrolizumab (200 mg IV Q3W) starting about 3 weeks before surgery.
- Standard-of-care surgery.
- Up to 3 doses of Pembrolizumab administered concurrently with adjuvant chemoradiotherapy (depending on pathologic risk).
- 12 additional adjuvant doses of Pembrolizumab Q3W (total treatment duration: about 1 year).
- Control arm (N=358):
- Identical treatment structure, substituting placebo for Pembrolizumab.
PD-L1 expression was assessed via Combined Positive Score (CPS), and stratification included CPS ≥1 and CPS ≥10 subgroups, recognizing the prognostic and potentially predictive value of PD-L1 expression. The Primary endpoint was Event-Free Survival (EFS), defined as time from randomization to disease progression, local/regional recurrence, distant metastasis, or death from any cause. Secondary endpoints included Overall Survival (OS) and Major Pathological Response.
The trial met its Primary endpoint of EFS. At median follow-up of 38.3 months, patients in the investigational arm had significantly improved EFS compared with the Standard of Care arm (median 51.8 months vs. 30.4 months; HR=0.73; P=0.0041). Patients who received Pembrolizumab who had a CPS score ≥10 derived the greatest benefit (median 59.7 months vs. 26.9 months; HR = 0.66; P=0.002) whereas the median EFS in the CPS ≥1 subgroup was 59.7 vs. 29.6 months (HR, 0.70; P = .0014).
Major pathological response defined as 90% or more tumor regression was also notably improved. Among all patients, the major pathological response rate was 9.4% with Pembrolizumab vs. 0% with Standard of Care (P < 0.00001). In the CPS ≥10 subgroup, the major pathological response rate reached 13.7%.
While the interim analysis did not demonstrate a statistically significant OS benefit, trends were favorable, particularly in the CPS ≥10 group (HR, 0.72; P =0.02). Further OS follow-up is ongoing.
Adverse events were consistent with known profiles of checkpoint inhibitors. Grade 3 or more Treatment-Related Adverse Events (TRAEs) occurred in 44.6% of the Pembrolizumab group and 42.9% in the Standard of Care group. Immune-mediated adverse events were observed in 43.2% of the Pembrolizumab arm, with hypothyroidism being the most common (24.7%). Mortality attributable to treatment was slightly higher with Pembrolizumab (1.1% vs. 0.3%).
The researchers concluded that perioperative Pembrolizumab is now emerging as a new standard of care in the treatment of resectable locally advanced HNSCC. The findings from this study underscore the importance of harnessing the immune system both before and after surgery. Neoadjuvant administration may prime the immune response when tumor antigen burden is highest, while adjuvant therapy may help eliminate residual microscopic disease.
Neoadjuvant and adjuvant pembrolizumab plus standard of care in resectable locally advanced head and neck squamous cell carcinoma: phase 3 KEYNOTE-689 study. Uppaluri R, et al. Abstract CT001. Presented at: American Association for Cancer Research Annual Meeting; April 25-30, 2025; Chicago.
Late Breaking Abstract – ESMO 2022: Neoadjuvant KEYTRUDA® with Chemoradiation in Locally Advanced Head and Neck Squamous Cell Carcinoma
SUMMARY: The American Cancer Society estimates that in the US for 2022, about 54,000 new cases of oral cavity or oropharyngeal cancer will be diagnosed and about 11,230 patients will die of the disease. Patients with Squamous Cell Carcinoma of the head and neck, frequently present with locoregionally advanced disease.
The treatment paradigm for Head and Neck cancer has been rapidly evolving with the recognition and better understanding of immune evasion and the role of immune checkpoints or gate keepers in suppressing antitumor immunity. Blocking the immune checkpoints unleashes the T cells, resulting in T cell proliferation, activation, and a therapeutic response. Checkpoint inhibitors administered in a neoadjuvant setting activates both the priming phase of immunity within tumor tissue, and the effector phase within the tumor microenvironment. It has been shown that neoadjuvant immunotherapy expands more T-cell clones than adjuvant treatment. Preclinical models have also demonstrated that both radiation therapy and Cisplatin chemotherapy increase the PD-L1 expression on the tumor, suggesting that combining radiotherapy with anti-PD-1 therapy could improve the outcomes.
Pembrolizumab (KEYTRUDA®) is a fully humanized, Immunoglobulin G4, monoclonal antibody and checkpoint inhibitor, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. Pembrolizumab has been shown to improve Overall Survival in patients with Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma
KEYNOTE-412 is a randomized, double-blind, Phase III trial, conducted to evaluate the efficacy and safety of Pembrolizumab in combination with chemoradiation versus placebo in combination with chemoradiation, in treatment naïve patients with locally advanced Head and Neck Squamous Cell carcinoma. In this study, 804 patients were randomly assigned 1:1 to receive Pembrolizumab 200 mg IV every 3 weeks plus chemoradiation (70Gy in 35 fractions along with Cisplatin 100 mg/m2 IV every 3 weeks) followed by Pembrolizumab (N=402), or placebo every 3 weeks plus chemoradiation, followed by placebo (N=402). Patients received Pembrolizumab /placebo priming dose 1 week before chemoradiation, followed by 2 doses during chemoradiation and 14 doses of maintenance therapy after chemoradiation, for a total of 17 doses. Enrolled patients had newly diagnosed, pathologically proven, treatment naive locally advanced Head and Neck Squamous Cell carcinoma (T3-T4, N0-N3 or any N2a-3, T1-T4 larynx/hypopharynx/oral cavity/p16-negative oropharynx cancers, or T4 or N3 p16-positive oropharynx cancer). Both treatment groups were well balanced. The Primary endpoint was Event Free Survival (EFS). Secondary endpoints included Overall Survival (OS), and Safety.
At the time of data cutoff, with a median follow up of 47.7 months, there was a favorable trend toward improved Event Free Survival (EFS) with the addition of Pembrolizumab vs placebo to chemoradiation (HR 0.83, P=0.04), but the difference did not achieve statistical significance. The 2-year EFS was 63.2% in the Pembrolizumab group and 56.2% in the placebo group. In an exploratory analysis however, the 2-year EFS among patients with high expression of PD-L1 (CPS 20 or higher) was 71% in the Pembrolizumab group and 62% in the placebo group. A favorable of Overall Survival benefit was also observed among these patients, with a 3-year OS of 79% in Pembrolizumab group and 73% in the placebo group.
It was concluded that Pembrolizumab in combination with chemoradiation was associated with a favorable trend toward improved Event Free Survival, compared with placebo plus chemoradiation, in patients with locally advanced Head and Neck Squamous Cell carcinoma, but the difference did not reach statistical significance. The researchers added that perhaps patients with high CPS score on the tumor could benefit with this treatment approach.
Primary results of the phase III KEYNOTE-412 study: Pembrolizumab (pembro) with chemoradiation therapy (CRT) vs placebo plus CRT for locally advanced (LA) head and neck squamous cell carcinoma (HNSCC). Machiels J, Tao Y, Burtness B, et al. Annals of Oncology (2022) 33 (suppl_7): S808-S869. 10.1016/annonc/annonc1089. LBA5
Late Breaking Abstract – ASCO 2022: Docetaxel as Radiosensitizer Improves Overall Survival in Cisplatin-Ineligible Head and Neck cancer
SUMMARY: The American Cancer Society estimates that in the US for 2022, about 54,000 new cases of oral cavity or oropharyngeal cancer will be diagnosed and about 11,230 patients will die of the disease. Patients with squamous cell carcinoma of the head and neck, frequently present with locoregionally advanced disease. For patients in this setting, chemoradiotherapy is an effective non-surgical approach as primary treatment. Alternatively, chemoradiotherapy can be delivered as adjuvant therapy after a curative resection.
Cisplatin-based concurrent chemoradiation is generally accepted as the standard, definitive non-surgical and post-operative approach in selected patients with locoregionally advanced squamous cell carcinoma of the head and neck. This treatment can however be associated with substantial morbidity and lifelong toxicities. Cetuximab is an immunoglobulin G1 chimeric monoclonal antibody against Epidermal Growth Factor Receptor (EGFR), and the only approved targeted agent in locoregionally advanced squamous cell carcinoma of the head and neck. Cetuximab plus Radiotherapy significantly improved Overall Survival at 5 years, when compared with radiotherapy alone, in patients with locoregionally advanced squamous cell carcinoma of the head and neck (Lancet Oncol. 2010). Cetuximab plus Radiotherapy is therefore an important treatment option in this patient group. However, financial barriers make Cetuximab as a Cisplatin substitute, inaccessible to patients, in low and middle-income countries.
Docetaxel is a semisynthetic taxane that affects polymerized tubulin to promote microtubule formation and inhibit its disassembly. Docetaxel has been shown to have significant antitumor activity as a single agent in head and neck cancer, when given in the neoadjuvant setting. Docetaxel is also a potent radiosensitizer. The researchers evaluated Docetaxel as a radiosensitizer in this clinical trial.
The authors in this open-label, randomized, Phase III study enrolled 356 Cisplatin-ineligible patients with locally advanced head and neck squamous cell carcinoma, planned for treatment with radical or adjuvant chemoradiation. The patients were randomly assigned 1:1 to receive Radiation alone (N=176) or Radiation with concurrent Docetaxel 15 mg/m2 IV weekly for a maximum of 7 cycles (N=180). Both treatment groups were well balanced. The median age was 62 yrs, approximately 45% of patients had a ECOG Performance Status of 2, and reasons for Cisplatin ineligibility included low creatinine clearance (26%), and hearing loss (43%). Approximately 33% of patients had oral cavity cancer and about two-thirds of patients had Stage IVA disease. The FACT-G, and Head and Neck questionnaires were completed by patients at baseline, 6 months, 12 months and at 24 months. FACT-G (Functional Assessment of Cancer Therapy-G) is a 27-item questionnaire designed to measure four domains of Health-Related Quality of Life (HRQOL) in cancer patients, which includes physical, social, emotional, and functional well-being. The Primary endpoint was Disease Free Survival (DFS), and key Secondary endpoints included Overall Survival (OS), adverse events and Quality of Life.
It was noted that the 2-year DFS was 30.3% with Radiation alone versus 42% with Docetaxel plus Radiation Therapy (HR=0.67; P=0.002). Docetaxel plus Radiation Therapy also significantly improved Overall Survival. The median Overall Survival was 15.3 months with Radiation Therapy alone, versus 25.5 months in the Docetaxel plus Radiation Therapy group (P=0.035). The 2 -year Overall Survival was also significantly higher in the Docetaxel plus Radiation Therapy group and was 41.7% with Radiation Therapy alone, versus 50.8% in the Docetaxel plus Radiation Therapy group (HR=0.74; P=0.035). These survival outcomes were observed across all preplanned subgroups.
Grade 3 or above adverse events were seen in 58% of patients receiving Radiation Therapy alone and in 81.6% of patients receiving Docetaxel plus Radiation Therapy. The addition of Docetaxel to Radiation Therapy resulted in a higher incidence of Grade 3 and above mucositis (49.7% versus 22.2%; P<0.001), odynophagia (52.5% versus 33.5%; P<0.001) and dysphagia (49.7% versus 33%; P<0.002). The addition of Docetaxel however did not lead to a worsening of Quality of Life, including Trial Outcome Index and FACT-G scores at 6 months.
The authors concluded that the addition of Docetaxel to Radiation Therapy improved Disease Free Survival and Overall Survival, in Cisplatin-ineligible locally advanced head and neck squamous cell carcinoma, and provides an evidence based, financially more viable treatment option, for this patient group.
Results of phase 3 randomized trial for use of docetaxel as a radiosensitizer in patients with head and neck cancer unsuitable for cisplatin-based chemoradiation. Patil VM, Noronha V, Menon NS, et al. DOI: 10.1200/JCO.2022.40.17_suppl.LBA6003 Journal of Clinical Oncology 40, no. 17_suppl (June 10, 2022) LBA6003.
KEYTRUDA® (Pembrolizumab)
The FDA on June 10, 2019 approved KEYTRUDA® for the first-line treatment of patients with metastatic or unresectable recurrent Head and Neck Squamous Cell Carcinoma (HNSCC). KEYTRUDA® is a product of Merck.
OPDIVO® (Nivolumab)
The FDA on November 10, 2016 approved OPDIVO® for the treatment of patients with recurrent or metastatic Squamous Cell Carcinoma of the Head and Neck (SCCHN), with disease progression on or after a platinum-based therapy. OPDIVO® is marketed by Bristol-Myers Squibb company.
FDA Approves OPDIVO® for Head and Neck Cancer
SUMMARY: The FDA on November 10, 2016, approved OPDIVO® (Nivolumab) for the treatment of patients with recurrent or metastatic Squamous Cell Carcinoma of the Head and Neck (SCCHN), with disease progression on or after a Platinum-based therapy. The American Cancer Society estimates that 61,760 people will be diagnosed with Head and Neck cancer in 2016 and 13,190 patients will die of the disease. Patients with recurrent/metastatic Squamous Cell Carcinoma of the Head and Neck have a poor prognosis with a median Overall Survival (OS) of about 13 months with first line therapy and about 6 months or less with later lines of therapy. The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of immune evasion and the role of Immune checkpoints or gate keepers. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent related to their ability to escape immune surveillance by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies have been developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By blocking the Immune checkpoints, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response.
OPDIVO® is an immune checkpoint PD-1 (Programmed cell Death 1) targeted, fully human, immunoglobulin G4 monoclonal antibody that has demonstrated antitumor efficacy in multiple tumor types. The FDA approval of OPDIVO® for the treatment of recurrent or metastatic Squamous Cell Carcinoma of the Head and Neck (SCCHN), was based on the results of CheckMate-141 study which is a randomized, open label, phase III trial. In this study, 361 patients with recurrent Squamous Cell Carcinoma of the Head and Neck (cancer of the oral cavity, pharynx, or larynx), whose disease had progressed within 6 months after Platinum-based chemotherapy, were randomly assigned, in a 2:1 ratio to receive OPDIVO® (N=240) or investigator’s choice of a standard, single agent therapy (N=121). OPDIVO® was administered at a dose of 3 mg/kg every 2 weeks, whereas standard therapy consisted of either weekly Methotrexate at a dose of 40-60 mg/m2 IV, weekly Docetaxel at a dose of 30-40 mg/m2 IV or Cetuximab administered at a loading dose of 400 mg/m2 followed by 250 mg/m2 IV weekly. The median age was 60 years, over 90% had received prior radiation therapy and 54.5% of the patients had received 2 or more lines of prior systemic therapies. The primary end point was Overall Survival and secondary end points included Progression Free Survival, Objective Response Rate, safety, and patient-reported quality of life measures. Prespecified analysis of Overall Survival according to tumor PD-L1 expression and p16 status was also performed.
The median Overall Survival was 7.5 months in the OPDIVO® group versus 5.1 months for the group that received standard therapy and this improvement was statistically significant (HR=0.70; P=0.01). The estimated 1-year survival rate was 36% in the OPDIVO® group and 16.6% with standard therapy. The median Progression Free Survival was 2.0 months with OPDIVO® versus 2.3 months with standard therapy and the rate of Progression Free Survival at 6 months was 19.7% with OPDIVO® versus 9.9% with standard therapy. The Objective Response Rate was 13.3% in the OPDIVO® group versus 5.8% in the standard therapy group. Even though preliminary biomarker analysis suggested that patients with a tumor PD-L1 expression level of 1% or more, or p16-positive tumors, or both, benefited more from OPDIVO® therapy than those whose PD-L1 level was less than 1% or who had p16-negative tumors, these interactions were not statistically significant. Treatment-related grade 3 or 4 adverse events were more common in the standard therapy group (35%) versus OPDIVO® group (13%) and quality of life measures were stable in the OPDIVO® group and were worse for those who received standard therapy.
The authors concluded that OPDIVO® prolonged survival, as compared with standard therapy, among patients with Platinum-refractory Squamous Cell Carcinoma of the Head and Neck and this benefit was accomplished with fewer toxicities, compared with standard therapy. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. Ferris RL, Blumenschein G, Fayette J, et al. N Engl J Med 2016; 375:1856-1867
FDA Approves KEYTRUDA® for Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma
SUMMARY: The FDA on August 5, 2016, granted accelerated approval to KEYTRUDA® (Pembrolizumab) for the treatment of patients with recurrent or metastatic Head and Neck Squamous Cell Carcinoma (HNSCC), with disease progression on or after Platinum containing chemotherapy. The American Cancer Society estimates that 61,760 people will be diagnosed with Head and Neck cancer in 2016 and 13,190 patients will die of the disease. Patients with recurrent/metastatic Squamous Cell Carcinoma of the Head and Neck have a poor prognosis with a median Overall Survival (OS) of about 13 months with first line therapy and about 6 months or less with later lines of therapy. 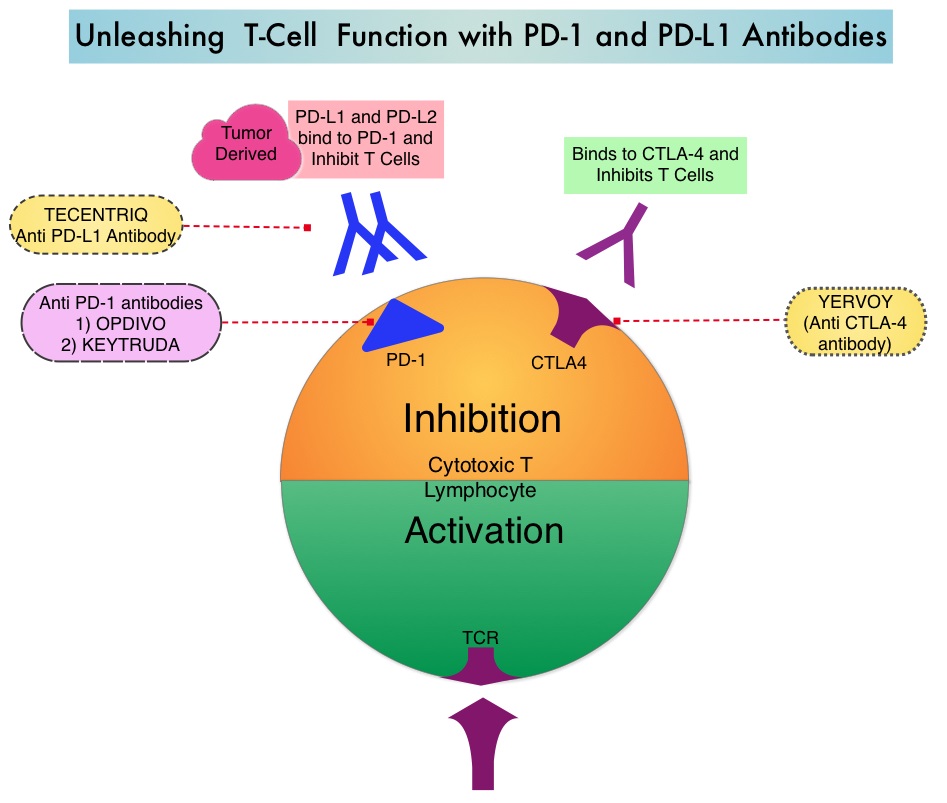 The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of the Immune checkpoints or gate keepers. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent related to their ability to escape immune surveillance by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response.
The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of the Immune checkpoints or gate keepers. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent related to their ability to escape immune surveillance by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response.
KEYTRUDA® is a fully humanized, Immunoglobulin G4, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. The accelerated approval of KEYTRUDA® was based on a multicenter, nonrandomized, open-label, multi-cohort phase Ib study (KEYNOTE-012), which included 192 patients with recurrent or metastatic HNSCC. Approximately 33% of the patients were HPV positive and patients have a median of two prior lines of therapy. Almost all enrolled patients (95%) had prior radiation therapy. Median patient age was 60 years. Treatment consisted of KEYTRUDA® 10 mg/kg IV every 2 weeks or 200 mg IV every 3 weeks and continued until disease progression or unacceptable toxicities. Patients without disease progression were treated for up to 24 months. The primary end point was Objective Response Rate (ORR) and Duration of Response. Secondary endpoints included response by HPV status, Progression Free Survival (PFS), and safety. Efficacy was evaluated in 174 of the enrolled patients. The ORR was 16% with a Complete Response Rate of 5%. The median response duration had not been reached at the time of analysis. Among the responding patients, 82% had responses of 6 months or longer. The ORR and Duration of Response were similar irrespective of dosage regimen or HPV status. In a pooled analyses after long term follow up, responses were ongoing in 76% of the patients with a median follow up duration in responders of 12.5 months. Median Overall Survival was 8.5 months and 6 month PFS rate was 24.9%. The most common adverse reactions ((20% or greater) were fatigue, decreased appetite, and dyspnea and these were similar to those occurring in patients with Melanoma or Non Small Cell Lung Cancer, with the exception of an increased incidence of facial edema and new or worsening hypothyroidism.
It was concluded that KEYTRUDA® has significant antitumor activity in recurrent/metastatic Head and Neck Squamous Cell Carcinoma and PD-L1 testing is not needed prior to use of KEYTRUDA® for this indication. As a condition of the accelerated approval, a multicenter, randomized trial is to be conducted for continued approval, establishing the superiority of KEYTRUDA® over standard therapy. Efficacy and safety of pembrolizumab in recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC): Pooled analyses after long-term follow-up in KEYNOTE-012. Mehra R, Seiwert TY, Mahipal A, et al. J Clin Oncol 34, 2016 (suppl; abstr 6012)