
The FDA on October 18, 2024, approved VYLOY®, a Claudin 18.2 (CLDN18.2)-directed cytolytic antibody, with Fluoropyrimidine- and Platinum-containing chemotherapy, for the first-line treatment of adults with locally advanced unresectable or metastatic Human Epidermal growth factor Receptor 2 (HER2)-negative Gastric or GastroEsophageal Junction (GEJ) adenocarcinoma whose tumors are CLDN18.2 positive, as determined by an FDA-approved test. VYLOY® is a product of Astellas Pharma US, Inc.
Tag: Gastric and GE Junction Cancer
FDA Approves VYLOY® with Chemotherapy for Biomarker Positive Gastric or GEJ Adenocarcinoma
SUMMARY: The FDA on October 18, 2024, approved Zolbetuximab-clzb (VYLOY®), a claudin 18.2 (CLDN18.2)-directed cytolytic antibody, with fluoropyrimidine and platinum-containing chemotherapy, for the first-line treatment of adults with locally advanced unresectable or metastatic Human Epidermal growth factor Receptor 2 (HER2)-negative Gastric or GastroEsophageal Junction (GEJ) adenocarcinoma whose tumors are CLDN18.2 positive, as determined by an FDA-approved test. The FDA also approved the VENTANA CLDN18 (43-14A) RxDx Assay (Ventana Medical Systems, Inc./Roche Diagnostics) as a companion diagnostic device to identify patients with Gastric or GEJ adenocarcinoma who may be eligible for treatment with Zolbetuximab.
The American Cancer Society estimates that in the US about 26,890 new gastric cancer cases will be diagnosed in 2024 and about 10,880 people will die of the disease. It is one of the leading causes of cancer-related deaths in the world. Several hereditary syndromes such as Hereditary Diffuse Gastric Cancer (HDGC), Lynch syndrome (Hereditary Nonpolyposis Colorectal Cancer) and Familial Adenomatous Polyposis (FAP) have been associated with a predisposition for Gastric cancer. Additionally, one of the strongest risk factor for Gastric adenocarcinoma is infection with Helicobacter pylori (H.pylori), which is a gram-negative, spiral-shaped microaerophilic bacterium.
Patients with localized disease (Stage II and Stage III) are often treated with multimodality therapy and 40% of the patients may survive for 5 years or more. However, majority of the patients with Gastric and GastroEsophageal junction (GEJ) adenocarcinoma have advanced disease at the time of initial presentation and have limited therapeutic options with little or no chance for cure. The five-year relative survival rate for patients with metastatic disease is approximately 6%. These patients frequently are treated with platinum containing chemotherapy along with a fluoropyrimidine such as modified FOLFOX6 or CAPOX. Patients with HER2-positive disease are usually treated with chemotherapy plus Trastuzumab, and for those patients with HER2-negative disease, patients receive chemotherapy along with a checkpoint inhibitor, or checkpoint inhibitor alone, if the tumors express PD-L1.
CLDN18.2 protein found in normal gastric cells, and is a major component of epithelial and endothelial tight junctions controlling the flow of molecules between cells. Pre-clinical studies have shown that CLDN18.2 expression which can also be present in gastric tumors, increases as cancer progresses, and may become more exposed on the surface of the cancer cells and accessible to targeted therapies with antibodies. CLDN18.2 is expressed in 30-40% of Gastric adenocarcinomas.
Zolbetuximab is a first-in-class chimeric IgG1 monoclonal antibody that targets and binds to CLDN18.2, a transmembrane protein. The binding interaction of Zolbetuximab to CLDN18.2 activates Antibody-Dependent Cellular Cytotoxicity (ADCC) and Complement Dependent Cytotoxicity (CDC) resulting in cancer cell death.
SPOTLIGHT trial is a Phase III, global, multi-center, double-blind, randomized study, in which the efficacy and safety of Zolbetuximab plus mFOLFOX6 was compared with placebo plus mFOLFOX6, as first-line treatment of patients with CLDN18.2-positive, HER2- negative, locally advanced unresectable or metastatic Gastric or GastroEsophageal Junction cancer. This study met the Primary endpoint and the median Progression Free Survival (PFS) was 10.6 months with the Zolbetuximab plus mFOLFOX6 combination versus 8.67 months with placebo plus mFOLFOX6 (HR=0.75; P=0.0066) and this was statistically significant. The Overall Survival (OS) was also significantly improved (18.23 versus 15.54 months, HR=0.75; P=0.0053), making this one of the longest durations of median OS seen in Phase III trials for this patient population.
GLOW trial is a global, multi-center, double-blind, randomized Phase III study, conducted to assess the efficacy and safety of Zolbetuximab plus CAPOX (N=254) versus placebo plus CAPOX (N=253) as a first-line treatment for patients with CLDN18.2-positive/HER2-negative, unresectable, locally advanced or metastatic Gastric or GEJ cancer. In this trial, 507 eligible patients were randomly assigned 1:1 to receive Zolbetuximab 800 mg/m2 IV as a loading dose on cycle 1, day 1, of the first 21-day cycle, followed by 600 mg/m2 IV on day 1 of subsequent cycles, along with CAPOX regimen consisting of Capecitabine 1000 mg/m2 orally twice daily on days 1-14 of each cycle and Oxaliplatin 130 mg/m2 IV on day 1 of each cycle, or the same CAPOX regimen plus placebo. CAPOX was given for 8 cycles in both treatment groups and patients could continue beyond 8 cycles with Zolbetuximab or placebo plus Capecitabine at investigator’s decision, and treatment continued until disease progression or unacceptable toxicities. CLDN18.2 positive was defined as at least 75% of tumor cells with moderate-to-strong membranous CLDN18.2 staining and patients were stratified by region (Asia versus non-Asia), number of organs with metastases, and prior gastrectomy (yes versus no). The median patient age was 60 years, majority of patients were male from Asia, not having prior gastrectomy, having stomach as the primary tumor site, and having an ECOG performance status of 1. Basline characteristics were similar in both treatment groups. The Primary end point was Progression Free Survival (PFS) and Secondary endpoints included Overall Survival (OS), Overall Response Rate (ORR), Duration of Response (DOR), and Safety.
At a median follow up of 12.6 months, the combination of Zolbetuximab plus CAPOX significantly improved PFS, and the median PFS was 8.2 months, compared with 6.8 months for those given placebo plus CAPOX (HR=0.68; P=0.0007). The median OS was 14.4 months versus 12.2 months respectively (HR=0.77; P=0.01). The PFS and OS benefits were sustained at 24 months, and the benefits were observed across most subgroups. The most common side effects were nausea and vomiting and the authors recommended increasing the infusion duration time, or splitting the dose over a 2 day period, in addition to the administration of prophylactic antiemetics.
The researchers concluded that the addition of first-line Zolbetuximab to CAPOX significantly improved PFS and OS in patients with CLDN18.2-positive, HER2-negative, unresectable, locally advanced or metastatic Gastric or GEJ cancer. The authors added that Zolbetuximab plus CAPOX represents a potential new first-line therapy for this patient group. Taken together, both GLOW and SPOTLIGHT trials showed a similar reduction in the risk of disease progression or death and a similar reduction in the risk of death with the addition of Zolbetuximab to chemotherapy, when compared with placebo plus chemotherapy.
Zolbetuximab plus CAPOX in CLDN18.2-positive gastric or gastroesophageal junction adenocarcinoma: the randomized, phase 3 GLOW trial. Shah MA, Shitara K, Ajani JA, et al. Nature Medicine 2023; 29:2133–2141
Bispecific Immune Checkpoint Inhibitor Improves Survival in Gastric and GEJ Cancer Regardless of PD-L1 Status
SUMMARY: The American Cancer Society estimates that in the US about 26,890 new gastric cancer cases will be diagnosed in 2024 and about 10,880 people will die of the disease. It is one of the leading causes of cancer-related deaths in the world. Several hereditary syndromes such as Hereditary Diffuse Gastric Cancer (HDGC), Lynch syndrome (Hereditary Nonpolyposis Colorectal Cancer) and Familial Adenomatous Polyposis (FAP) have been associated with a predisposition for gastric cancer. Additionally, one of the strongest risk factor for gastric adenocarcinoma is infection with Helicobacter pylori (H.pylori), which is a gram-negative, spiral-shaped microaerophilic bacterium.
Patients with localized disease (Stage II and Stage III) are often treated with multimodality therapy and 40% of the patients may survive for 5 years or more. However, majority of the patients with gastric and gastroesophageal junction (GEJ) adenocarcinoma have advanced disease at the time of initial presentation and have limited therapeutic options with little or no chance for cure. The five-year relative survival rate for patients at the metastatic stage is approximately 15%. These patients frequently are treated with platinum containing chemotherapy along with a Fluoropyrimidine such as modified FOLFOX6 or CAPOX. Patients with HER2-positive disease are usually treated with chemotherapy plus Trastuzumab, and for those patients with HER2-negative disease, patients receive chemotherapy along with a checkpoint inhibitor, or checkpoint inhibitor alone, if the tumors express PD-L1.
Cadonilimab (AK104) is a human, bispecific IgG1 antibody with high binding avidity especially to high density of PD-1 and CTLA-4 due to its tetravalent design, and could simultaneously bind different cells expressing PD-1 and CTLA-4, respectively. By effective blocking both PD-1 and CTLA-4 pathways, Cadonilimab activates T cells by increasing interleukin-2 (IL-2) and interferon-gamma secretion to similar extent, as compared with anti-PD-1 and anti-CTLA-4 combination.
COMPASSION-15 is a double-blind, randomized, multicenter, Phase III trial that enrolled 610 patients diagnosed with locally advanced unresectable or metastatic gastric or gastroesophageal junction (GEJ) cancer. They were randomly assigned 1:1 to receive either Cadonilimab in combination with Oxaliplatin and Capecitabine chemotherapy, or placebo plus the same chemotherapy. Chemotherapy with Oxaliplatin and Capecitabine was given every 3 weeks for up to six cycles. Capecitabine was administered at 1000 mg/m2 orally twice daily on days 1 through 14 every 3 weeks and Oxaliplatin IV at 130 mg/m2 every 3 weeks. Cadonilimab 10 mg/kg IV or placebo was given on day 1 of each cycle every 3 weeks. Following the 6 cycles, patients then received Cadonilimab 10 mg/kg IV monotherapy or placebo every 3 weeks. Stratification factors included ECOG performance status (0 versus 1), PD-L1 expression (CPS 5% or more, or less than 5%), and the presence or absence of liver metastasis. The Primary endpoint was Overall Survival (OS) in the Intent to Treat (ITT) population.
The researchers herein presented the interim analysis data of COMPASSION-15 trial. The results revealed a significant improvement in Overall Survival with Cadonilimab combination therapy compared to placebo. The median OS was 15.0 months with Cadonilimab combination, compared with 10.8 months for those in the placebo arm (HR=0.60; P<0.001). The 18-month Overall Survival rate was 45.8% in the Cadonilimab group versus 25.5% in the placebo group.
Subgroup analysis based on PD-L1 expression levels (CPS 5% or more, or less than 5%) also demonstrated favorable outcomes with Cadonilimab across all strata. Among patients with a PD-L1 CPS of less than 5%, Cadonilimab combination achieved a median OS of 14.8 months, compared with 11.1 months in the placebo group. The 18-month OS rates were 44.1% compared with 27.5%, respectively.
Progression-Free Survival (PFS), another critical measure of treatment efficacy, showed consistent benefits with Cadonilimab combination compared to placebo plus chemotherapy, irrespective of PD-L1 expression. Median PFS was 7 months versus 5.3 months in the ITT population, with similar trends observed in CPS 5% or more, and less than 5% subgroups.
The safety analysis revealed no new safety signals. However, Grade 3 or higher treatment-related adverse events were more commonly reported in the combination therapy group compared to the placebo group. Treatment-related adverse events leading to therapy discontinuation were also more frequent in the Cadonilimab group.
It was concluded from this study that Cadonilimab is the first PD-1/CTLA-4 bispecific antibody to demonstrate substantial improvements in Overall Survival and Progression-Free Survival benefit in combination with chemotherapy, offering a potential new standard of care for patients diagnosed with locally advanced unresectable or metastatic gastric or gastroesophageal junction (GEJ) cancer. This study represents a significant milestone in the quest for improved first-line treatments for gastric and GEJ cancers, even for patients with low PD-L1 expression tumors.
Cadonilimab plus chemotherapy versus chemotherapy as first-line treatment for unresectable locally advanced or metastatic gastric or gastroesophageal junction (G/GEJ) adenocarcinoma (COMPASSION-15): A randomized, double-blind, phase 3 trial. Ji J, Shen L, Li Z, et al. Presented at: 2024 AACR Annual Meeting; April 5-10, 2024; San Diego, CA.
Durable survival with OPDIVO ® (nivolumab) + chemotherapy (fluoropyrimidine- and platinum-based) vs chemotherapy alone, a first-line treatment of metastatic gastric cancer, gastroesophageal junction cancer, and esophageal adenocarcinoma, regardless of PD-L1 status at 4 years of follow-up1,2
Ronan Kelly, MD, MBA,
The Charles A. Sammons Cancer Center,
Baylor University Medical Center, Dallas, Texas*
Content sponsored by: Bristol Myers Squibb
*Dr Kelly was compensated by BMS for his contribution in drafting this article.
Introduction: Overview of gastroesophageal adenocarcinoma
Gastroesophageal adenocarcinomas consist of a heterogeneous group of tumors, including gastric cancer (GC), gastroesophageal junction cancer (GEJC), and esophageal adenocarcinoma (EAC), all of which are aggressive malignancies with poor outcomes.3-6 The aggressive natures of GC and EAC may contribute to their respective statuses as two of the most common causes of cancer-related death globally.7
 Checkmate 649 led to the approval of nivolumab (OPDIVO) + chemotherapy as the first chemoimmunotherapy combination for all eligible patients with HER2-negative† GC/GEJC/EAC regardless of PD-L1 status.1,8,9 Prior to this approval, chemotherapy was the only available 1L treatment option for metastatic GC/GEJC/EAC.10 Furthermore, to date, Checkmate 649 has the longest follow-up survival data in GC vs chemotherapy for any I-O–based regimen with a minimum follow-up of 48.1 months (median of 59.3 months), and showed durable survival data with OPDIVO + chemotherapy in GC/GEJC/EAC.1,2,11 OPDIVO can be given q2w or q3w, which synchronizes with the q2w FOLFOX and q3w CapeOx dosing schedules.1 “The flexible dosing schedule of OPDIVO has made it more convenient to integrate into my clinical practice,” stated Dr. Kelly.
Checkmate 649 led to the approval of nivolumab (OPDIVO) + chemotherapy as the first chemoimmunotherapy combination for all eligible patients with HER2-negative† GC/GEJC/EAC regardless of PD-L1 status.1,8,9 Prior to this approval, chemotherapy was the only available 1L treatment option for metastatic GC/GEJC/EAC.10 Furthermore, to date, Checkmate 649 has the longest follow-up survival data in GC vs chemotherapy for any I-O–based regimen with a minimum follow-up of 48.1 months (median of 59.3 months), and showed durable survival data with OPDIVO + chemotherapy in GC/GEJC/EAC.1,2,11 OPDIVO can be given q2w or q3w, which synchronizes with the q2w FOLFOX and q3w CapeOx dosing schedules.1 “The flexible dosing schedule of OPDIVO has made it more convenient to integrate into my clinical practice,” stated Dr. Kelly.
†Indication has no restriction on HER2 status; trial included HER2-negative patients and patients with unknown HER2 status, while excluding those with known HER2-positive status.1
OPDIVO + chemotherapy in 1L metastatic GC/GEJC/EAC
With the longest follow-up survival data in GC vs chemotherapy for any I-O–based regimen and durable survival data in GC/GEJC/EAC, OPDIVO + fluoropyrimidine- and platinum-containing chemotherapy is currently FDA-approved in 1L metastatic non–HER2-positive† GC/GEJC/EAC, regardless of PD-L1 status (no testing required).1,2,9 The approval of this combination was based on the results of Checkmate 649, a global phase 3 study in patients with 1L metastatic GC/GEJC/EAC.1,8 Key exclusion criteria included known HER2-positive status and untreated CNS metastases.8 The study recruited all eligible patients regardless of PD-L1 expression.1,8
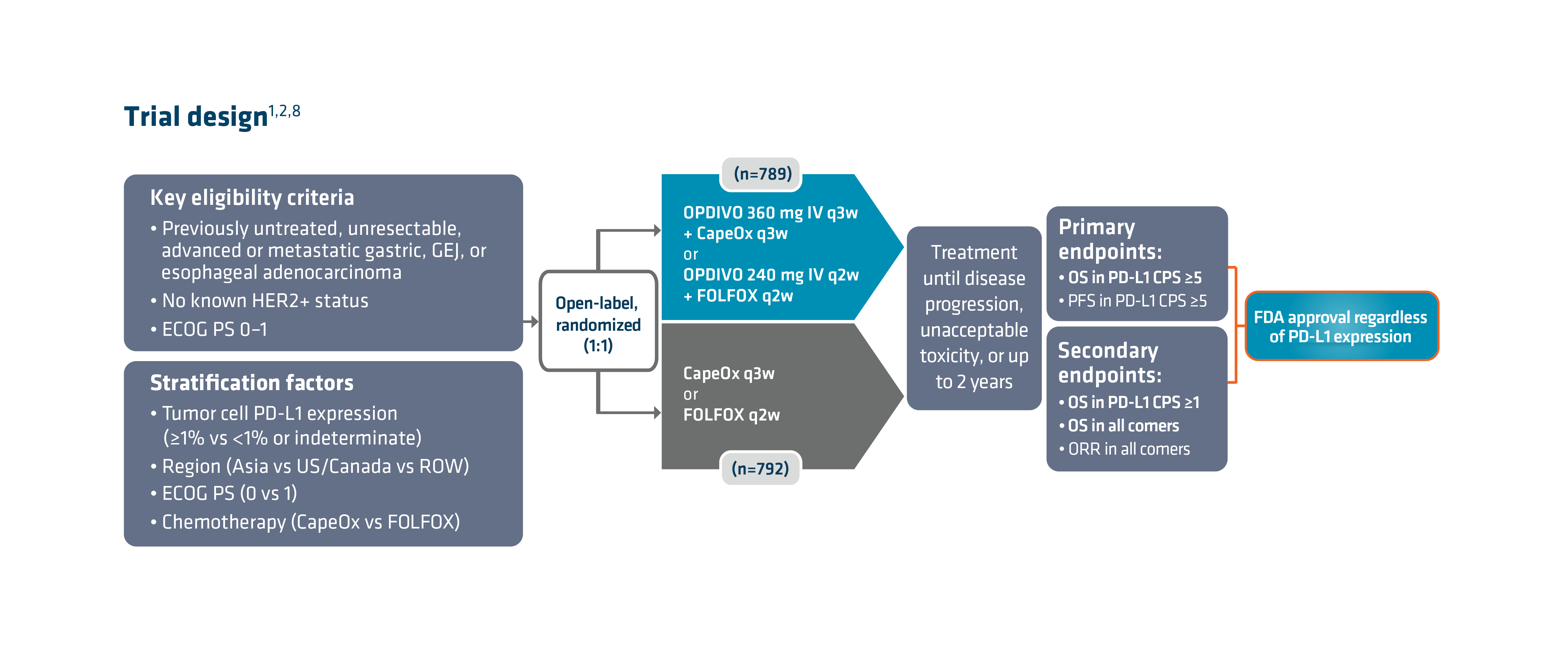 Checkmate 649 enrolled 1581 patients randomized 1:1 to receive either OPDIVO + chemotherapy (n=789) or chemotherapy alone (n=792). The dual primary endpoints were OS and PFS in PD-L1 CPS ≥5. OS in PD-L1 CPS ≥1 and in all-comers were secondary endpoints, but were powered to measure statistical significance through hierarchical analysis. Baseline characteristics were consistent among all randomized patients and patients with PD-L1 CPS ≥5. Checkmate 649 was the first phase 3 trial to achieve positive results in the evaluation of a PD-1 inhibitor in combination with FOLFOX or CapeOx, allowing for synchronized I-O dosing options with the preferred chemotherapy.8
Checkmate 649 enrolled 1581 patients randomized 1:1 to receive either OPDIVO + chemotherapy (n=789) or chemotherapy alone (n=792). The dual primary endpoints were OS and PFS in PD-L1 CPS ≥5. OS in PD-L1 CPS ≥1 and in all-comers were secondary endpoints, but were powered to measure statistical significance through hierarchical analysis. Baseline characteristics were consistent among all randomized patients and patients with PD-L1 CPS ≥5. Checkmate 649 was the first phase 3 trial to achieve positive results in the evaluation of a PD-1 inhibitor in combination with FOLFOX or CapeOx, allowing for synchronized I-O dosing options with the preferred chemotherapy.8
There are warnings and precautions associated with OPDIVO to keep in mind. These include severe and fatal immune-mediated adverse reactions, infusion-related reactions, complications of allogeneic hematopoietic stem cell transplantation, embryo-fetal toxicity, and increased mortality in patients with multiple myeloma when OPDIVO is added to a thalidomide analogue and dexamethasone, which is not recommended outside of controlled clinical trials.1 Additional information related to warnings and precautions can be found here .
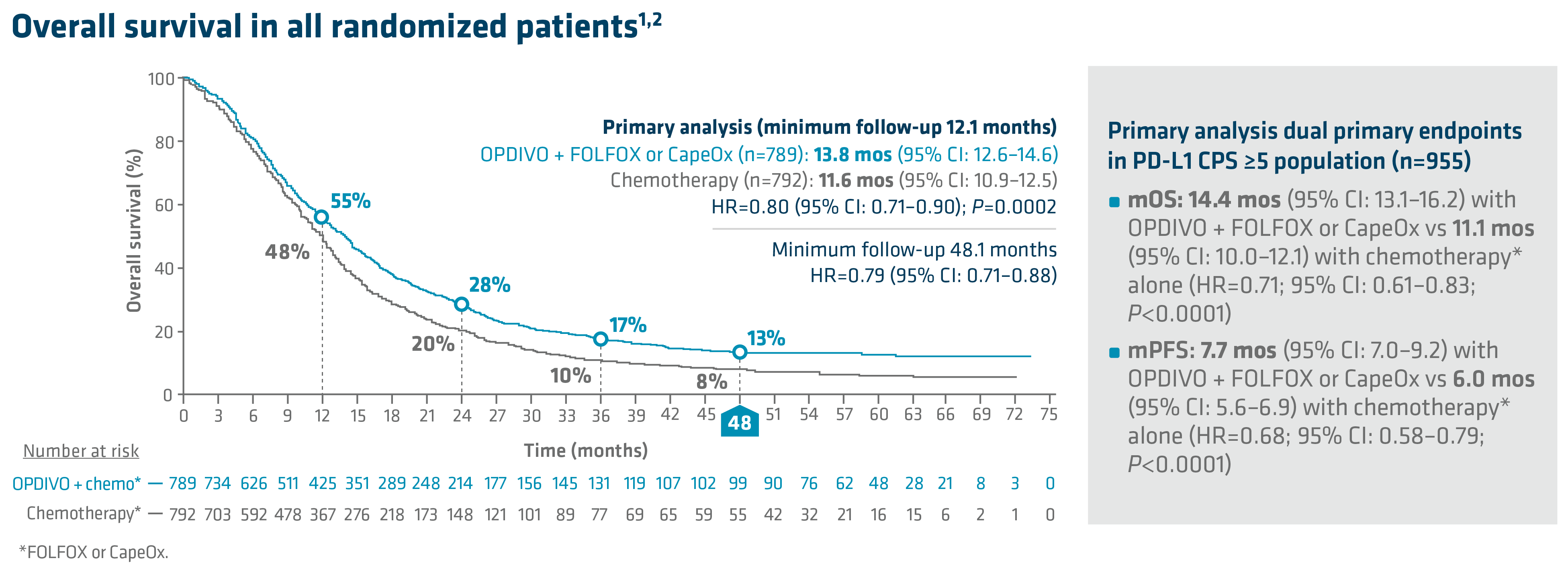 In the primary analysis (minimum follow-up of 12.1 months), OPDIVO + chemotherapy demonstrated superior OS in all randomized patients and patients with PD-L1 CPS ≥5, as compared to chemotherapy alone. In all randomized patients, mOS was 13.8 mos with OPDIVO + chemotherapy vs 11.6 mos with chemotherapy (HR=0.80; 95% CI: 0.71–0.90; P=0.0002). In patients with PD-L1 CPS ≥5 (n=955), mOS was 14.4 mos with OPDIVO + chemotherapy vs 11.1 mos with chemotherapy (HR=0.71; 95% CI: 0.61–0.83; P<0.0001).1 The 12-month OS rate in all randomized patients was 55% with OPDIVO + chemotherapy vs 48% with chemotherapy.8 “In my opinion, clinical trial data with OPDIVO + chemotherapy was a landmark. For the first time in a non–HER2-positive population, patients were able to break through the 1-year mOS barrier,” explained Dr. Kelly.
In the primary analysis (minimum follow-up of 12.1 months), OPDIVO + chemotherapy demonstrated superior OS in all randomized patients and patients with PD-L1 CPS ≥5, as compared to chemotherapy alone. In all randomized patients, mOS was 13.8 mos with OPDIVO + chemotherapy vs 11.6 mos with chemotherapy (HR=0.80; 95% CI: 0.71–0.90; P=0.0002). In patients with PD-L1 CPS ≥5 (n=955), mOS was 14.4 mos with OPDIVO + chemotherapy vs 11.1 mos with chemotherapy (HR=0.71; 95% CI: 0.61–0.83; P<0.0001).1 The 12-month OS rate in all randomized patients was 55% with OPDIVO + chemotherapy vs 48% with chemotherapy.8 “In my opinion, clinical trial data with OPDIVO + chemotherapy was a landmark. For the first time in a non–HER2-positive population, patients were able to break through the 1-year mOS barrier,” explained Dr. Kelly.
Durable survival data was observed for this OPDIVO-based regimen vs chemotherapy alone in GC/GEJC/EAC. The follow-up analysis at 48.1 months reported a mOS of 13.7 mos (95% CI: 12.4–14.5) with OPDIVO + chemotherapy vs 11.6 mos (95% CI: 10.9–12.5) with chemotherapy in all randomized patients (HR=0.79; 95% CI: 0.71–0.88), and 14.4 mos (95% CI: 13.1–16.2) with OPDIVO + chemotherapy vs 11.1 mos (95% CI: 10.1–12.1) with chemotherapy in patients with PD-L1 CPS ≥5 (HR=0.70; 95% CI: 0.61–0.81). The 48-month OS rate was 13% vs 8% for OPDIVO + chemotherapy vs chemotherapy, respectively, in all randomized patients.2
In Checkmate 649, the most common adverse reactions reported in ≥20% of patients treated with OPDIVO in combination with chemotherapy were peripheral neuropathy, nausea, fatigue, diarrhea, vomiting, decreased appetite, abdominal pain, constipation, and musculoskeletal pain. OPDIVO and/or chemotherapy were discontinued in 44% of patients and at least one dose was withheld in 76% of patients due to an adverse reaction. Serious adverse reactions occurred in 52% of patients treated with OPDIVO in combination with chemotherapy. The most frequent serious adverse reactions reported in ≥2% of patients treated with OPDIVO in combination with chemotherapy were vomiting (3.7%), pneumonia (3.6%), anemia (3.6%), pyrexia (2.8%), diarrhea (2.7%), febrile neutropenia (2.6%), and pneumonitis (2.4%). Fatal adverse reactions occurred in 16 (2.0%) patients who were treated with OPDIVO in combination with chemotherapy; these included pneumonitis (4 patients), febrile neutropenia (2 patients), stroke (2 patients), gastrointestinal toxicity, intestinal mucositis, septic shock, pneumonia, infection, gastrointestinal bleeding, mesenteric vessel thrombosis, and disseminated intravascular coagulation.1
An additional characteristic of OPDIVO is its flexible dosing schedule. Based on both the FDA-approved label and Checkmate 649 trial design, OPDIVO offers flexible synchronized dosing options based on chemotherapy preference, and “in my experience, allows scheduling according to the patient and clinician preference,” stated Dr. Kelly. Checkmate 649 evaluated OPDIVO (q2w or q3w) in combination with physician’s choice of either FOLFOX given q2w or CapeOx given q3w in the first-line treatment of certain metastatic gastroesophageal cancers. Treatment can be continued until disease progression, unacceptable toxicity, or up to 2 years.1

Summary and conclusions
With the longest follow-up survival data in GC vs chemotherapy for any I-O–based regimen and durable survival data in GC/GEJC/EAC, OPDIVO in combination with fluoropyrimidine- and platinum-containing chemotherapy is an approved 1L treatment option for all eligible patients with non–HER2-positive† GC/GEJC/EAC, regardless of PD-L1 status.1,2 OPDIVO also offers synchronized dosing options to align with preferred chemotherapies, including both FOLFOX and CapeOx, which can be used every 2 or 3 weeks, respectively.1 “I believe Checkmate 649 may act as a new benchmark moving forward and novel therapeutics may be compared against it,” stated Dr. Kelly.
1L=first line; CapeOx=capecitabine and oxaliplatin; CI=confidence interval; CNS=central nervous system; CPS=combined positive score; FOLFOX=leucovorin, fluorouracil, and oxaliplatin; GEJ=gastroesophageal junction; HER2=human epidermal growth factor receptor 2; HR=hazard ratio; I-O=immuno-oncology; IV=intravenous; mo=month; mOS=median OS; mPFS=median PFS; ORR=overall response rate; OS=overall survival; PD-1=programmed death receptor-1; PD-L1=programmed death ligand 1; PFS=progression-free survival; q2w=every 2 weeks; q3w=every 3 weeks; ROW=rest of world.
INDICATION
OPDIVO® (nivolumab), in combination with fluoropyrimidine- and platinum-containing chemotherapy, is indicated for the treatment of adult patients with advanced or metastatic gastric cancer, gastroesophageal junction cancer, and esophageal adenocarcinoma.
OPDIVO (10 mg/mL) is an injection for intravenous use.
IMPORTANT SAFETY INFORMATION
Severe and Fatal Immune-Mediated Adverse Reactions
• Immune-mediated adverse reactions listed herein may not include all possible severe and fatal immune-mediated adverse reactions.
• Immune-mediated adverse reactions, which may be severe or fatal, can occur in any organ system or tissue. While immune-mediated adverse reactions usually manifest during treatment, they can also occur after discontinuation of OPDIVO. Early identification and management are essential to ensure safe use of OPDIVO. Monitor for signs and symptoms that may be clinical manifestations of underlying immune-mediated adverse reactions. Evaluate clinical chemistries including liver enzymes, creatinine, and thyroid function at baseline and periodically during treatment with OPDIVO. In cases of suspected immune-mediated adverse reactions, initiate appropriate workup to exclude alternative etiologies, including infection. Institute medical management promptly, including specialty consultation as appropriate.
• Withhold or permanently discontinue OPDIVO depending on severity (please see section 2 Dosage and Administration in the accompanying Full Prescribing Information). In general, if OPDIVO interruption or discontinuation is required, administer systemic corticosteroid therapy (1 to 2 mg/kg/day prednisone or equivalent) until improvement to Grade 1 or less. Upon improvement to Grade 1 or less, initiate corticosteroid taper and continue to taper over at least 1 month. Consider administration of other systemic immunosuppressants in patients whose immune-mediated adverse reactions are not controlled with corticosteroid therapy. Toxicity management guidelines for adverse reactions that do not necessarily require systemic steroids (e.g., endocrinopathies and dermatologic reactions) are discussed below.
Immune-Mediated Pneumonitis
• OPDIVO can cause immune-mediated pneumonitis. The incidence of pneumonitis is higher in patients who have received prior thoracic radiation. In patients receiving OPDIVO monotherapy, immune-mediated pneumonitis occurred in 3.1% (61/1994) of patients, including Grade 4 (<0.1%), Grade 3 (0.9%), and Grade 2 (2.1%).
Immune-Mediated Colitis
• OPDIVO can cause immune-mediated colitis. A common symptom included in the definition of colitis was diarrhea. Cytomegalovirus (CMV) infection/reactivation has been reported in patients with corticosteroid-refractory immune-mediated colitis. In cases of corticosteroid-refractory colitis, consider repeating infectious workup to exclude alternative etiologies. In patients receiving OPDIVO monotherapy, immune-mediated colitis occurred in 2.9% (58/1994) of patients, including Grade 3 (1.7%) and Grade 2 (1%).
Immune-Mediated Hepatitis and Hepatotoxicity
• OPDIVO can cause immune-mediated hepatitis. In patients receiving OPDIVO monotherapy, immune-mediated hepatitis occurred in 1.8% (35/1994) of patients, including Grade 4 (0.2%), Grade 3 (1.3%), and Grade 2 (0.4%).
Immune-Mediated Endocrinopathies
• OPDIVO can cause primary or secondary adrenal insufficiency, immune-mediated hypophysitis, immune-mediated thyroid disorders, and Type 1 diabetes mellitus, which can present with diabetic ketoacidosis. Withhold OPDIVO depending on severity (please see section 2 Dosage and Administration in the accompanying Full Prescribing Information). For Grade 2 or higher adrenal insufficiency, initiate symptomatic treatment, including hormone replacement as clinically indicated. Hypophysitis can present with acute symptoms associated with mass effect such as headache, photophobia, or visual field defects. Hypophysitis can cause hypopituitarism; initiate hormone replacement as clinically indicated. Thyroiditis can present with or without endocrinopathy. Hypothyroidism can follow hyperthyroidism; initiate hormone replacement or medical management as clinically indicated. Monitor patients for hyperglycemia or other signs and symptoms of diabetes; initiate treatment with insulin as clinically indicated.
• In patients receiving OPDIVO monotherapy, adrenal insufficiency occurred in 1% (20/1994), including Grade 3 (0.4%) and Grade 2 (0.6%).
• In patients receiving OPDIVO monotherapy, hypophysitis occurred in 0.6% (12/1994) of patients, including Grade 3 (0.2%) and Grade 2 (0.3%).
• In patients receiving OPDIVO monotherapy, thyroiditis occurred in 0.6% (12/1994) of patients, including Grade 2 (0.2%).
• In patients receiving OPDIVO monotherapy, hyperthyroidism occurred in 2.7% (54/1994) of patients, including Grade 3 (<0.1%) and Grade 2 (1.2%).
• In patients receiving OPDIVO monotherapy, hypothyroidism occurred in 8% (163/1994) of patients, including Grade 3 (0.2%) and Grade 2 (4.8%).
• In patients receiving OPDIVO monotherapy, diabetes occurred in 0.9% (17/1994) of patients, including Grade 3 (0.4%) and Grade 2 (0.3%), and 2 cases of diabetic ketoacidosis.
Immune-Mediated Nephritis with Renal Dysfunction
• OPDIVO can cause immune-mediated nephritis. In patients receiving OPDIVO monotherapy, immune-mediated nephritis and renal dysfunction occurred in 1.2% (23/1994) of patients, including Grade 4 (<0.1%), Grade 3 (0.5%), and Grade 2 (0.6%).
Immune-Mediated Dermatologic Adverse Reactions
• OPDIVO can cause immune-mediated rash or dermatitis. Exfoliative dermatitis, including Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and drug rash with eosinophilia and systemic symptoms (DRESS) has occurred with PD-1/PD-L1 blocking antibodies. Topical emollients and/or topical corticosteroids may be adequate to treat mild to moderate nonexfoliative rashes.
• Withhold or permanently discontinue OPDIVO depending on severity (please see section 2 Dosage and Administration in the accompanying Full Prescribing Information).
• In patients receiving OPDIVO monotherapy, immune-mediated rash occurred in 9% (171/1994) of patients, including Grade 3 (1.1%) and Grade 2 (2.2%).
Other Immune-Mediated Adverse Reactions
• The following clinically significant immune-mediated adverse reactions occurred at an incidence of <1% (unless otherwise noted) in patients who received OPDIVO monotherapy or were reported with the use of other PD-1/PD-L1 blocking antibodies. Severe or fatal cases have been reported for some of these adverse reactions: cardiac/vascular: myocarditis, pericarditis, vasculitis; nervous system: meningitis, encephalitis, myelitis and demyelination, myasthenic syndrome/myasthenia gravis (including exacerbation), Guillain-Barré syndrome, nerve paresis, autoimmune neuropathy; ocular: uveitis, iritis, and other ocular inflammatory toxicities can occur; gastrointestinal: pancreatitis to include increases in serum amylase and lipase levels, gastritis, duodenitis; musculoskeletal and connective tissue: myositis/polymyositis, rhabdomyolysis, and associated sequelae including renal failure, arthritis, polymyalgia rheumatica; endocrine: hypoparathyroidism; other (hematologic/immune): hemolytic anemia, aplastic anemia, hemophagocytic lymphohistiocytosis (HLH), systemic inflammatory response syndrome, histiocytic necrotizing lymphadenitis (Kikuchi lymphadenitis), sarcoidosis, immune thrombocytopenic purpura, solid organ transplant rejection.
• Some ocular IMAR cases can be associated with retinal detachment. Various grades of visual impairment, including blindness, can occur. If uveitis occurs in combination with other immune-mediated adverse reactions, consider a Vogt-Koyanagi-Harada–like syndrome, which has been observed in patients receiving OPDIVO, as this may require treatment with systemic corticosteroids to reduce the risk of permanent vision loss.
Infusion-Related Reactions
• OPDIVO can cause severe infusion-related reactions. Discontinue OPDIVO in patients with severe (Grade 3) or life-threatening (Grade 4) infusion-related reactions. Interrupt or slow the rate of infusion in patients with mild (Grade 1) or moderate (Grade 2) infusion-related reactions. In patients receiving OPDIVO monotherapy as a 60-minute infusion, infusion-related reactions occurred in 6.4% (127/1994) of patients. In a separate trial in which patients received OPDIVO monotherapy as a 60-minute infusion or a 30-minute infusion, infusion-related reactions occurred in 2.2% (8/368) and 2.7% (10/369) of patients, respectively. Additionally, 0.5% (2/368) and 1.4% (5/369) of patients, respectively, experienced adverse reactions within 48 hours of infusion that led to dose delay, permanent discontinuation or withholding of OPDIVO.
Complications of Allogeneic Hematopoietic Stem Cell Transplantation
• Fatal and other serious complications can occur in patients who receive allogeneic hematopoietic stem cell transplantation (HSCT) before or after being treated with OPDIVO. Transplant-related complications include hyperacute graft-versus-host-disease (GVHD), acute GVHD, chronic GVHD, hepatic veno-occlusive disease (VOD) after reduced intensity conditioning, and steroid-requiring febrile syndrome (without an identified infectious cause). These complications may occur despite intervening therapy between OPDIVO and allogeneic HSCT.
• Follow patients closely for evidence of transplant-related complications and intervene promptly. Consider the benefit versus risks of treatment with OPDIVO prior to or after an allogeneic HSCT.
Embryo-Fetal Toxicity
• Based on its mechanism of action and findings from animal studies, OPDIVO can cause fetal harm when administered to a pregnant woman. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with OPDIVO and for at least 5 months after the last dose.
Increased Mortality in Patients with Multiple Myeloma when OPDIVO is Added to a Thalidomide Analogue and Dexamethasone
• In randomized clinical trials in patients with multiple myeloma, the addition of OPDIVO to a thalidomide analogue plus dexamethasone resulted in increased mortality. Treatment of patients with multiple myeloma with a PD-1 or PD-L1 blocking antibody in combination with a thalidomide analogue plus dexamethasone is not recommended outside of controlled clinical trials.
Lactation
• There are no data on the presence of OPDIVO in human milk, the effects on the breastfed child, or the effects on milk production. Because of the potential for serious adverse reactions in breastfed children, advise women not to breastfeed during treatment and for 5 months after the last dose.
Serious Adverse Reactions
• In Checkmate 649, serious adverse reactions occurred in 52% of patients treated with OPDIVO in combination with chemotherapy (n=782). The most frequent serious adverse reactions reported in ≥2% of patients treated with OPDIVO in combination with chemotherapy were vomiting (3.7%), pneumonia (3.6%), anemia (3.6%), pyrexia (2.8%), diarrhea (2.7%), febrile neutropenia (2.6%), and pneumonitis (2.4%). Fatal adverse reactions occurred in 16 (2.0%) patients who were treated with OPDIVO in combination with chemotherapy; these included pneumonitis (4 patients), febrile neutropenia (2 patients), stroke (2 patients), gastrointestinal toxicity, intestinal mucositis, septic shock, pneumonia, infection, gastrointestinal bleeding, mesenteric vessel thrombosis, and disseminated intravascular coagulation.
Common Adverse Reactions
• In Checkmate 649, the most common adverse reactions (≥20%) in patients treated with OPDIVO in combination with chemotherapy (n=782) were peripheral neuropathy (53%), nausea (48%), fatigue (44%), diarrhea (39%), vomiting (31%), decreased appetite (29%), abdominal pain (27%), constipation (25%), and musculoskeletal pain (20%).
Please see US Full Prescribing Information for OPDIVO.
References:
1. OPDIVO [package insert]. Princeton, NJ: Bristol-Myers Squibb Company.
2. Shitara K, Moehler M, Ajani JA, et al. Nivolumab plus chemotherapy vs chemotherapy as first-line treatment for advanced gastric cancer/gastroesophageal junction cancer/esophageal adenocarcinoma: 4-year follow-up of the CheckMate 649 study. Oral presentation at ASCO GI 2024. Abstract 306.
3. Mantziari S, St Amour P, Abboretti F, et al. A comprehensive review of prognostic factors in patients with gastric adenocarcinoma. Cancers (Basel). 2023;15(5):1628.
4. Imamura Y, Watanabe M, Oki E, Morita M, Baba H. Esophagogastric junction adenocarcinoma shares characteristics with gastric adenocarcinoma: literature review and retrospective multicenter cohort study. Ann Gastroenterol Surg. 2020;5(1):46-59.
5. Rogers MP, DeSantis AJ, DuCoin CG. Oligometastatic adenocarcinoma of the esophagus: current understanding, diagnosis, and therapeutic strategies. Cancers (Basel). 2021;13(17):4352.
6. Paydary K, Reizine N, Catenacci DVT. Immune-checkpoint inhibition in the treatment of gastro-esophageal cancer: a closer look at the emerging evidence. Cancers (Basel). 2021;13(23):5929.
7. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249.
8. Janjigian YY, Shitara K, Moehler M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet. 2021;398(10294):27-40.
9. Janjigian YY, Ajani JA, Moehler M, et al. Nivolumab plus chemotherapy or ipilimumab vs chemotherapy as first-line treatment for advanced gastric cancer/gastroesophageal junction cancer/esophageal adenocarcinoma: CheckMate 649 study. Oral presentation at ESMO 2021. Abstract LBA7.
10. Shankaran V, Xiao H, Bertwistle D, et al. A comparison of real-world treatment patterns and clinical outcomes in patients receiving first-line therapy for unresectable advanced gastric or gastroesophageal junction cancer versus esophageal adenocarcinomas. Adv Ther. 2021;38:
707-720.
11. BMS-REF-NIVO-0256. Princeton, NJ: Bristol-Myers Squibb Company; 2024.
© 2024 Bristol-Myers Squibb Company. OPDIVO® is a registered trademark of Bristol-Myers Squibb Company.
1506-US-2300555 01/24
KEYTRUDA® (Pembrolizumab)
The FDA on November 16, 2023, approved KEYTRUDA® (Pembrolizumab) with Fluoropyrimidine and Platinum-containing chemotherapy for the first-line treatment of adults with locally advanced unresectable or metastatic HER2-negative Gastric or GastroEsophageal Junction (GEJ) adenocarcinoma. KEYTRUDA® is a product of Merck & Co., Inc.
KEYTRUDA® (Pembrolizumab)
The FDA on November 7, 2023, revised the existing indication of KEYTRUDA® (Pembrolizumab) with Trastuzumab, Fluoropyrimidine, and Platinum-containing chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-positive Gastric or GastroEsophageal Junction (GEJ) adenocarcinoma. This updated indication, which remains approved under accelerated approval regulations, restricts its use to patients whose tumors express PD-L1 (CPS ≥ 1) as determined by an FDA-approved test. KEYTRUDA® is a product of MERCK & Co., Inc.
FDA Approves KEYTRUDA® with Chemotherapy for HER2-Negative Gastric or GE Junction Adenocarcinoma
SUMMARY: The FDA on November 16, 2023, approved Pembrolizumab (KEYTRUDA®) with Fluoropyrimidine and Platinum containing chemotherapy for the first-line treatment of adults with locally advanced unresectable or metastatic HER2-negative Gastric or GastroEsophageal Junction (GEJ) adenocarcinoma. The American Cancer Society estimates that in the US about 26,500 new Gastric cancer cases will be diagnosed in 2023 and about 11,130 people will die of the disease. It is one of the leading causes of cancer-related deaths in the world. Several hereditary syndromes such as Hereditary Diffuse Gastric Cancer (HDGC), Lynch syndrome (Hereditary Nonpolyposis Colorectal Cancer) and Familial Adenomatous Polyposis (FAP) have been associated with a predisposition for Gastric cancer. Additionally, one of the strongest risk factor for Gastric adenocarcinoma is infection with Helicobacter pylori (H.pylori), which is a gram-negative, spiral-shaped microaerophilic bacterium.
Patients with localized disease (Stage II and Stage III) are often treated with multimodality therapy and 40% of the patients may survive for 5 years or more. However, majority of the patients with Gastric and GastroEsophageal junction Adenocarcinoma have advanced disease at the time of initial presentation and have limited therapeutic options with little or no chance for cure. These patients frequently are treated with Platinum containing chemotherapy along with a Fluoropyrimidine and, if appropriate, HER2/neu-targeted therapy. This can however be associated with significant toxicities impacting patient’s quality of life. The efficacy of PD-1 inhibitors in combination with chemotherapy has been demonstrated in Gastric and GastroEsophageal cancer.
KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2. It thereby reverses the PD-1 pathway-mediated inhibition of the immune response and unleashes the tumor-specific effector T cells.
The present FDA approval was based on KEYNOTE-859, which is a double-blind, placebo-controlled, randomized Phase III trial, conducted to evaluate the benefit of adding Pembrolizumab to Fluoropyrimidine and Platinum-containing doublet chemotherapy in patients with advanced HER2-negative Gastric or GastroEsophageal cancer. In this study, 1,579 patients with locally advanced or metastatic HER2-negative Gastric or GastroEsophageal adenocarcinoma, with known a PD-L1 Combined Positive Score (CPS), were randomly assigned 1:1 to receive Pembrolizumab 200 mg IV (N=790) or placebo (N=789), every 3 weeks for 35 cycles or less, given along with investigator’s choice of 5-FU plus Cisplatin or Capecitabine plus Oxaliplatin (CAPOX). Baseline characteristics were balanced between treatment groups and randomization was stratified by region, PD-L1 CPS (less than 1 versus 1 or more), and choice of chemotherapy. At baseline, 78% of patients had PD-L1 CPS 1 or more, while 35% had tumors with CPS 10 or more. The Primary end point was Overall Survival (OS) by blinded Independent Central Review. Secondary end points included Progression Free Survival (PFS), Objective Response Rate (ORR), Duration of Response (DOR) and Safety. The researchers provided the data from the interim analysis, at a median follow up of 31.0 months.
The median Overall Survival was 12.9 months with Pembrolizumab plus chemotherapy versus 11.5 months with chemotherapy alone (HR=0.78, P<0.0001). The median PFS was 6.9 months versus 5.6 months, respectively (HR=0.76, P<0.0001). The benefit with Pembrolizumab was consistent across subgroups, including those by PD-L1 CPS. The risk reduction was especially notable among patients with MicroSatellite Instability (MSI)-High status, who had a 66% relative reduction in the risk of death, and patients with PD-L1 CPS 10 or more, whose risk was reduced by 36%. The Objective Response Rate was 51.3% in the Pembrolizumab group and 42.0% in the control group (P=0.00009), and the median Duration of Response was 8.0 months versus 5.7 months, respectively. Immune-related toxicities, especially hypothyroidism, were more common with Pembrolizumab plus chemotherapy and no new safety signals were seen.
It was concluded that treatment with Pembrolizumab plus chemotherapy resulted in a statistically significant and clinically meaningful improvement in Overall Survival, Progression Free Survival and Objective Response Rate, among patients with locally advanced or metastatic, HER2-negative Gastric or GastroEsophageal adenocarcinoma of any PD-L1 expression level, thus providing a new treatment option for this patient group.
Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for HER2-negative advanced gastric cancer (KEYNOTE-859): a multicentre, randomised, double-blind, phase 3 trial. Rha SY, Oh D-Y, Yanez P, et al. The Lancet Oncology 2023; 24:1181-1195.
KEYTRUDA® in Combination with HER2 Blockade Improves PFS in Gastric and GE Junction Cancer
SUMMARY: Gastroesophageal cancers consist of a group of heterogeneous tumors, including gastric cancer, gastroesophageal junction cancer, and esophageal cancer. The majority of gastric and gastroesophageal junction cancers are adenocarcinomas, while the two main histological subtypes of esophageal cancer are esophageal adenocarcinoma and esophageal squamous cell carcinoma. The American Cancer Society estimates that in the US about 26,500 new gastric cancer cases and 21,560 new esophageal cancers will be diagnosed in 2023 and about 11,130 and 16,120 people respectively, will die of the disease. It is one of the leading causes of cancer-related deaths in the world. Patients with localized disease (Stage II and Stage III) are often treated with multimodality therapy and 40% of the patients may survive for 5 years or more. However, majority of the patients with gastric and gastroesophageal junction adenocarcinoma have advanced disease at the time of initial presentation and have limited therapeutic options with little or no chance for cure.
The Human Epidermal growth factor Receptor (HER) or erbB family of receptors, consist of HER1, HER2, HER3 and HER4. Approximately 15-20% of advanced gastric and gastroesophageal (GE) junction cancers, overexpress or have amplification of the HER2 oncogene. These patients often receive first line treatment with a combination of chemotherapy plus anti-HER2 antibody, Trastuzumab, as there is Overall Survival (OS) benefit with this combination regimen. Pembrolizumab (KEYTRUDA®) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor expressed on activated T cells, and blocks its interaction with ligands PD-L1 and PD-L2. It thereby reverses the PD-1 pathway-mediated inhibition of the immune response and unleashes the tumor-specific effector T cells. In two Phase II studies, Pembrolizumab in combination with Trastuzumab and chemotherapy showed promising efficacy with manageable toxicities. The FDA in 2021 granted accelerated approval to Pembrolizumab in combination with Trastuzumab, Fluoropyrimidine and Platinum-containing chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic HER2 positive gastric or gastroesophageal junction adenocarcinoma, based on Overall Response Rates (ORR).
KEYNOTE-811 is an ongoing, global, multicenter, randomized Phase III trial which evaluated the benefit of adding Pembrolizumab to Trastuzumab and chemotherapy in patients with locally advanced unresectable or metastatic HER2-positive gastric or gastroesophageal junction adenocarcinoma. In this study, 698 treatment naïve eligible patients (N=698) were randomly assigned 1:1 to receive Pembrolizumab 200 mg IV (N=350) or placebo (N=348) every 3 weeks plus Trastuzumab and investigator’s choice of Fluorouracil/Cisplatin or Capecitabine/Oxaliplatin. Trastuzumab was given at 6 mg/kg IV once every 3 weeks after a loading dose of 8 mg/kg IV. Chemotherapy consisted of 5-FU 800 mg/m2 IV on days 1 to 5 of each 3-week cycle and Cisplatin 80 mg/m2 IV once every 3 weeks, or Capecitabine 1,000 mg/m2 orally twice daily on days 1 to 14 of each 3-week cycle and Oxaliplatin 130 mg/m2 IV once every 3 weeks. Treatment was continued for up to 35 cycles or until disease progression or unacceptable toxicity. Approximately 81% were male and patients were stratified by PD-L1 status, and chemotherapy received. Over 80% of patients had a PD-L1 Combined Positive Score of 1 or more. The dual Primary end points of the trial were Progression Free Survival (PFS) and Overall Survival (OS). Secondary end points included Objective Response Rate (ORR), Duration of Response, and Safety. The researchers reported the results at the third interim analysis, after a median follow up of 38.5 months.
At the third interim analysis, the results continued to show superiority with the addition of Pembrolizumab to Trastuzumab and chemotherapy. The median PFS with Pembrolizumab versus placebo was 10 months versus 8.1 months, respectively (HR = 0.73; P=0.0002). This represented a 27% reduction in risk for progression with Pembrolizumab versus placebo. The median OS showed numerical improvement and was 20.0 months versus 16.8 months (HR=0.84), but did not meet prespecified criteria for significance. Follow up for Overall Survival is continuing, and results will be updated at the final analysis. Patients whose tumors had PD-L1 Combined Positive Score of 1 or more benefitted the most, and there was little to no benefit among patients whose tumors had PD-L1 Combined Positive Scores less than 1. The researchers had previously reported an ORR of 74% in the the Pembrolizumab group and 52% in the placebo group, yielding a 22% improvement for the Pembrolizumab group (P=0.00006). Disease Control Rates were 96.2% versus 89.3% respectively. Grade 3 or more treatment-related adverse events were higher among patients assigned to Pembrolizumab versus placebo group (58% versus 51%). The most common treatment-related adverse events of any grade were diarrhea, nausea and anemia.
The authors concluded that Pembrolizumab when combined with first line Trastuzumab and chemotherapy significantly improved Progression Free Survival when compared to placebo, in metastatic HER2-positive gastroesophageal cancer. This benefit was specifically noted among patients with tumors with a PD-L1 Combined Positive Score of 1 or more. Follow up for Overall Survival is ongoing and will be updated at the final analysis.
Pembrolizumab plus trastuzumab and chemotherapy for HER2-positive gastric or gastro-oesophageal junction adenocarcinoma: interim analyses from the phase 3 KEYNOTE-811 randomised placebo-controlled trial. Janjigian YY, Kawazoe A, Bai Y, et al. Published:October 20, 2023. DOI:https://doi.org/10.1016/S0140-6736(23)02033-0
Zolbetuximab plus CAPOX in Biomarker Positive Advanced Gastric or GEJ Cancer
SUMMARY: The American Cancer Society estimates that in the US about 26,500 new gastric cancer cases will be diagnosed in 2023 and about 11,130 people will die of the disease. It is one of the leading causes of cancer-related deaths in the world. Several hereditary syndromes such as Hereditary Diffuse Gastric Cancer (HDGC), Lynch syndrome (Hereditary Nonpolyposis Colorectal Cancer) and Familial Adenomatous Polyposis (FAP) have been associated with a predisposition for Gastric cancer. Additionally, one of the strongest risk factor for Gastric adenocarcinoma is infection with Helicobacter pylori (H.pylori), which is a gram-negative, spiral-shaped microaerophilic bacterium.
Patients with localized disease (Stage II and Stage III) are often treated with multimodality therapy and 40% of the patients may survive for 5 years or more. However, majority of the patients with Gastric and GastroEsophageal junction (GEJ) adenocarcinoma have advanced disease at the time of initial presentation and have limited therapeutic options with little or no chance for cure. The five-year relative survival rate for patients at the metastatic stage is approximately 6%. These patients frequently are treated with platinum containing chemotherapy along with a Fluoropyrimidine such as modified FOLFOX6 or CAPOX. Patients with HER2-positive disease are usually treated with chemotherapy plus Trastuzumab, and for those patients with HER2-negative disease, patients receive chemotherapy along with a checkpoint inhibitor, or checkpoint inhibitor alone, if the tumors express PD-L1.
CLDN18.2 protein found in normal gastric cells, and is a major component of epithelial and endothelial tight junctions controlling the flow of molecules between cells. Pre-clinical studies have shown that CLDN18.2 expression which can also be present in gastric tumors, increases as cancer progresses, and may become more exposed on the surface of the cancer cells and accessible to targeted therapies with antibodies. CLDN18.2 is expressed in 35% of Gastric adenocarcinomas.
Zolbetuximab is a first-in-class chimeric IgG1 monoclonal antibody that targets and binds to CLDN18.2, a transmembrane protein. The binding interaction of Zolbetuximab to CLDN18.2 activates Antibody-Dependent Cellular Cytotoxicity (ADCC) and Complement Dependent Cytotoxicity (CDC) resulting in cancer cell death. About 30-40% of patients with Gastric cancer have CLDN18.2 expression.
SPOTLIGHT trial is a Phase III, global, multi-center, double-blind, randomized study, in which the efficacy and safety of Zolbetuximab plus mFOLFOX6 was compared with placebo plus mFOLFOX6, as first-line treatment of patients with CLDN18.2-positive, HER2- negative, locally advanced unresectable or metastatic Gastric or GastroEsophageal Junction cancer. This study met the Primary endpoint and the median Progression Free Survival (PFS) was 10.61 months with the Zolbetuximab plus mFOLFOX6 combination versus 8.67 months with placebo plus mFOLFOX6 (HR=0.75; P=0.0066) and this was statistically significant. The Overall Survival (OS) was also significantly improved (18.23 versus 15.54 months, HR=0.750; P=0.0053), making this one of the longest durations of median OS seen in Phase III trials for this patient population.
GLOW trial is a global, multi-center, double-blind, randomized Phase III study, conducted to assess the efficacy and safety of Zolbetuximab plus CAPOX (N=254) versus placebo plus CAPOX (N=253) as a first-line treatment for patients with CLDN18.2-positive/HER2-negative, unresectable, locally advanced or metastatic Gastric or GEJ cancer. In this trial, 507 eligible patients were randomly assigned 1:1 to receive Zolbetuximab 800 mg/m2 IV as a loading dose on cycle 1, day 1, of the first 21-day cycle, followed by 600 mg/m2 IV on day 1 of subsequent cycles, along with CAPOX regimen consisting of Capecitabine 1000 mg/m2 orally twice daily on days 1-14 of each cycle and Oxaliplatin 130 mg/m2 IV on day 1 of each cycle, or the same CAPOX regimen plus placebo. CAPOX was given for 8 cycles in both treatment groups and patients could continue beyond 8 cycles with Zolbetuximab or placebo plus Capecitabine at investigator’s decision, and treatment continued until disease progression or unacceptable toxicities. CLDN18.2 positive was defined as at least 75% of tumor cells with moderate-to-strong membranous CLDN18.2 staining and patients were stratified by region (Asia versus non-Asia), number of organs with metastases, and prior gastrectomy (yes versus no). The median patient age was 60 years, majority of patients were male from Asia, not having prior gastrectomy, having stomach as the primary tumor site, and having an ECOG performance status of 1. Basline characteristics were similar in both treatment groups. The Primary end point was Progression Free Survival (PFS) and Secondary endpoints included Overall Survival (OS), Overall Response Rate (ORR), Duration of Response (DOR), and Safety.
At a median follow up of 12.6 months, the combination of Zolbetuximab plus CAPOX significantly improved PFS, and the median PFS was 8.2 months, compared with 6.8 months for those given placebo plus CAPOX (HR=0.687; P=0.0007). The median OS was 14.4 months versus 12.2 months respectively (HR=0.771; P=0.01). The PFS and OS benefits were sustained at 24 months, and the benefits were observed across most subgroups. The most common side effects were nausea and vomiting and the authors recommended increasing the infusion duration time, or splitting the dose over a 2 day period, in addition to the administration of prophylactic antiemetics.
The researchers concluded that the addition of first-line Zolbetuximab to CAPOX significantly improved PFS and OS in patients with CLDN18.2-positive, HER2-negative, unresectable, locally advanced or metastatic Gastric or GEJ cancer. The authors added that Zolbetuximab plus CAPOX represents a potential new first-line therapy for this patient group. Taken together, both GLOW and SPOTLIGHT trials showed a similar reduction in the risk of disease progression or death and a similar reduction in the risk of death with the addition of Zolbetuximab to chemotherapy, when compared with placebo plus chemotherapy.
Zolbetuximab plus CAPOX in CLDN18.2-positive gastric or gastroesophageal junction adenocarcinoma: the randomized, phase 3 GLOW trial. Shah MA, Shitara K, Ajani JA, et al. Nature Medicine 2023; 29:2133–2141
Zolbetuximab Plus Chemotherapy Improves Survival in CLDN18.2 Positive Metastatic Gastric and Gastroesophageal Junction Cancer
SUMMARY: The American Cancer Society estimates that in the US about 26,500 new gastric cancer cases will be diagnosed in 2023 and about 11,130 people will die of the disease. It is one of the leading causes of cancer-related deaths in the world. Several hereditary syndromes such as Hereditary Diffuse Gastric Cancer (HDGC), Lynch syndrome (Hereditary Nonpolyposis Colorectal Cancer) and Familial Adenomatous Polyposis (FAP) have been associated with a predisposition for Gastric cancer. Additionally, one of the strongest risk factor for Gastric adenocarcinoma is infection with Helicobacter pylori (H.pylori), which is a gram-negative, spiral-shaped microaerophilic bacterium.
Patients with localized disease (Stage II and Stage III) are often treated with multimodality therapy and 40% of the patients may survive for 5 years or more. However, majority of the patients with Gastric and GastroEsophageal junction Adenocarcinoma have advanced disease at the time of initial presentation and have limited therapeutic options with little or no chance for cure. The five-year relative survival rate for patients at the metastatic stage is approximately 6%.
These patients frequently are treated with platinum containing chemotherapy along with a Fluoropyrimidine such as modified FOLFOX6. Patients with HER2-positive disease are usually treated with chemotherapy plus trastuzumab, and for those patients with HER2-negative disease, patients receive chemotherapy along with a checkpoint inhibitor or checkpoint inhibitor alone if the tumors express PD-L1.
Zolbetuximab is a first-in-class chimeric IgG1 monoclonal antibody that targets and binds to CLDN18.2, a transmembrane protein. CLDN18.2 protein found in normal gastric cells, and is a major component of epithelial and endothelial tight junctions controlling the flow of molecules between cells. Pre-clinical studies have shown that CLDN18.2 expression which can also be present in gastric tumors, increases as cancer progresses, and may become more exposed and accessible to targeted therapies with antibodies as gastric tumors develop. The binding interaction of Zolbetuximab to CLDN18.2 activates Antibody-Dependent Cellular Cytotoxicity (ADCC) and Complement Dependent Cytotoxicity (CDC) resulting in cancer cell death. About 30-40% of patients with gastric cancer have CLDN18.2 expression.
SPOTLIGHT trial is a Phase III, global, multi-center, double-blind, randomized study, in which the efficacy and safety of Zolbetuximab plus mFOLFOX6 was compared with placebo plus mFOLFOX6, as first-line treatment of patients with CLDN18.2-positive, HER2- negative, locally advanced unresectable or metastatic Gastric or GastroEsophageal Junction cancer. In this study, 565 enrolled patients were randomly assigned 1:1 to receive the combination of Zolbetuximab and mFOLFOX6 (N=283) or placebo and mFOLFOX6 (N=282). Zolbetuximab was given at 800 mg/m2 IV on day 1 of cycle 1 followed by 600 mg/m2 on day 22 of cycle 1, and days 1 and 22 of subsequent cycles, every 3 weeks. mFOLFOX6 (Oxaliplatin, 5-Fluorouracil and Leucovorin) was given IV every 2 weeks in cycles 1 to 4 of 42-day cycles. For cycles 5 and beyond, Zolbetuximab was given at the same dosing schedule in combination with 5-Fluorouracil and Leucovorin IV every 2 weeks. Those in the placebo arm were given placebo at the every 3-week schedule and chemotherapy was administered at the same dosing schedule. Treatment was continued until disease progression or discontinuation criteria were met. Enrolled patients had moderate-to-strong CLDN18 staining intensity in at least 75% of tumor cells based on a validated ImmunoHistoChemistry assay, had HER2-negative disease, and an ECOG performance status of 0 or 1. Patients were stratified by region (Asian versus non-Asian), number of organs with metastases (0-2 versus 3 or more), and prior gastrectomy. The median age was 61 years and 31.4% of patients were from Asia. Majority of patients had 0-2 organs with metastases, 30% had prior gastrectomy. Approximately 13% of patients had tumors with a PD-L1 CPS of at least 5. The primary disease site was stomach in 76% of patients and was GastroEsophageal Junction in 24%. The Primary endpoint was Progression Free Survival (PFS). Secondary endpoints included Overall Survival (OS), Objective Response Rate (ORR), and Safety.
This study met the Primary endpoint and the median PFS was 10.61 months with the Zolbetuximab plus mFOLFOX6 combination versus 8.67 months with placebo plus mFOLFOX6 (HR=0.75; P=0.0066) and this was statistically significant. The OS was also significantly improved (18.23 versus 15.54 months, HR=0.750; P=0.0053), making this one of the longest durations of median OS seen in Phase III trials for this patient population. The most common Adverse Events with Zolbetuximab plus mFOLFOX6 were nausea, vomiting and decreased appetite. The incidences of serious Adverse Events were similar between the two treatment groups.
The authors concluded that Zolbetuximab plus mFOLFOX6 is a new potential Standard-of-Care treatment for a biomarker-based subgroup of patients with CLDN18.2-positive/HER2-negative locally advanced unresectable or metastatic Gastric/GE Junction adenocarcinoma. It is unclear if this regimen is superior to chemotherapy plus a checkpoint inhibitor in patients with PD-L1–positive and CLDN18.2-positive disease.
Zolbetuximab + mFOLFOX6 as first-line (1L) treatment for patients (pts) withclaudin-18.2+ (CLDN18.2+) / HER2− locally advanced (LA) unresectable or metastatic gastric or gastroesophageal junction (mG/GEJ) adenocarcinoma: Primary results from phase 3 SPOTLIGHT study. Shitara K, Lordick F, Bang Y-J, et al. J Clin Oncol. 2023;41(suppl; abstr LBA292). doi:10.1200/JCO.2023.41.3_suppl.LBA292