
The FDA on November 24, 2015 granted approval to PORTRAZZA® in combination with Gemcitabine and Cisplatin for first-line treatment of patients with metastatic squamous Non-Small Cell Lung Cancer (NSCLC). PORTRAZZA® is not indicated for treatment of non-squamous NSCLC and is a product of Eli Lilly and Company.
Author: RR
OPDIVO® (Nivolumab)
The FDA on November 23, 2015 approved OPDIVO® Injection, for the treatment of advanced renal cell carcinoma, in patients who have received prior anti-angiogenic therapy. OPDIVO® is a product of Bristol-Myers Squibb Company.
MEKINIST® (Trametinib) and TAFINLAR® (Dabrafenib)
The FDA on November 20, 2015 approved MEKINIST® and TAFINLAR® for use in combination, for the treatment of patients with unresectable or metastatic melanoma with BRAF V600E or V600K mutations, as detected by an FDA-approved test. MEKINIST® and TAFINLAR® are products of Novartis Pharmaceuticals Corp.
NINLARO® (Ixazomib)
The FDA on November 20, 2015 approved NINLARO® in combination with Lenalidomide and Dexamethasone for the treatment of patients with multiple myeloma who have received at least one prior therapy. NINLARO® is the first approved oral proteasome inhibitor and is a product of Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited.
DARZALEX® (Daratumumab)
The FDA on November 16, 2015 granted accelerated approval to DARZALEX®, administered as a single agent, for the treatment of patients with multiple myeloma who have received at least three prior lines of therapy, including a Proteasome Inhibitor (PI) and an immunomodulatory agent, or who are double-refractory to a PI and an immunomodulatory agent. DARZALEX® is a product of Janssen Biotech, Inc.
TAGRISSO® (Osimertinib)
The FDA on November 13, 2015 granted accelerated approval to TAGRISSO® once daily tablets, for the treatment of patients with metastatic Epidermal Growth Factor Receptor (EGFR) T790M mutation-positive Non-Small Cell Lung Cancer (NSCLC), as detected by an FDA-approved test, who have progressed on or after EGFR Tyrosine Kinase Inhibitor (TKI) therapy. TAGRISSO® is a product of AstraZeneca Pharmaceuticals LP.
COTELLIC® (Cobimetinib)
The FDA on November 10, 2015 approved COTELLIC® Tablets for the treatment of patients with unresectable or metastatic melanoma with BRAF V600E or V600K mutation, in combination with Vemurafenib. COTELLIC® is not indicated for treatment of patients with wild-type BRAF melanoma. COTELLIC® is a product of Genentech, Inc.
IMLYGIC® (Talimogene laherparepvec)
The FDA on October 27, 2015 approved IMLYGIC®, a genetically-modified oncolytic viral therapy indicated for the local treatment of unresectable cutaneous, subcutaneous, and nodal lesions in patients with melanoma, recurrent after initial surgery. IMLYGIC® is a product of Amgen, Inc.
Adjuvant AROMASIN® Most Beneficial for Premenopausal Women with High Risk Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 246,660 new cases of invasive breast cancer will be diagnosed in 2016 and 40,450 women will die of the disease. Approximately 75% of patients with breast cancer are hormone receptor positive (Estrogen Receptor/Progesterone Receptor positive) and this is a predictor of response to endocrine therapy. In premenopausal woman, the ovary is the main source of estrogen production, whereas in postmenopausal women, the primary source of estrogen is the Aromatase enzyme mediated conversion of androstenedione and testosterone to estrone and estradiol in extragonadal/peripheral tissues. Presently available therapies include Tamoxifen and other Selective Estrogen Receptor (ER) Modulators, which modulate ER alpha activity, Aromatase Inhibitors (AIs) and Ovarian ablation that decrease estrogen production and FASLODEX® (Fulvestrant) that down regulates Estrogen Receptor. Aromatase Inhibitors are often prescribed due to their superiority over Tamoxifen, for postmenopausal women with Hormone Receptor positive breast tumors, in adjuvant as well as metastatic settings. Aromatase Inhibitors by themselves however, are not effective in premenopausal women, as these individuals derive their estrogen mainly from ovaries and not extragonadal tissue.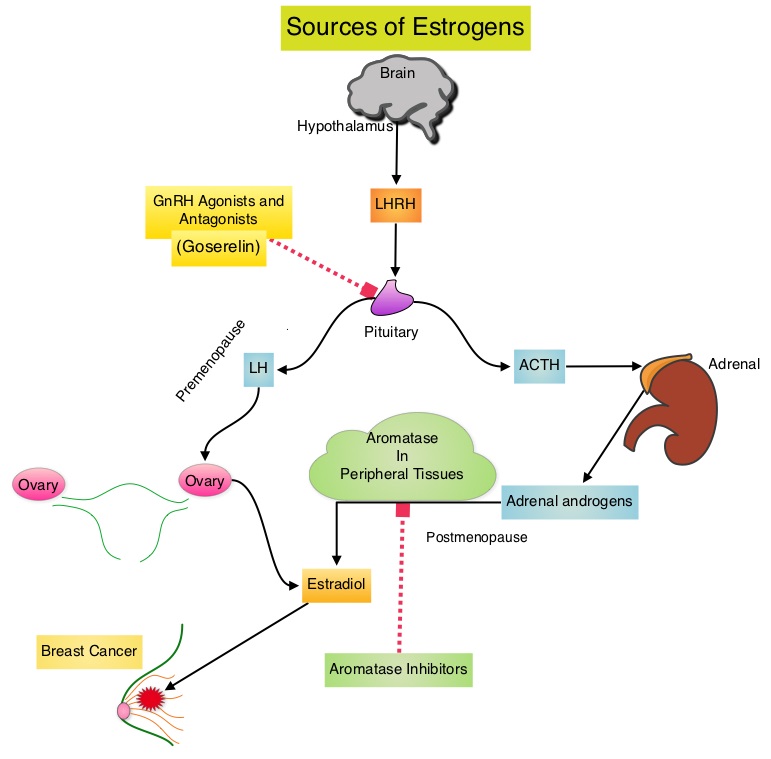
The TEXT (Tamoxifen and Exemestane Trial) and SOFT (Suppression of Ovarian Function Trial) are two phase III randomized trials, conducted at the same time and included premenopausal women (average age was 43 years) with hormone receptor positive, early breast cancer. In the joint analysis of these two trials which included 4,891 women, the authors set out to answer 2 important questions – whether adjuvant AI treatment improves outcomes in this patient group, when their Ovarian Function is suppressed and whether there is any benefit with Ovarian Function suppression in premenopausal women suitable for adjuvant Tamoxifen. TEXT randomized patients within 3 months of surgery to 5 years of AROMASIN® (Exemestane) plus Ovarian Function Suppression (OFS) or 5 years of Tamoxifen plus OFS. The SOFT study randomized patients to 5 years of AROMASIN® plus OFS or 5 years of Tamoxifen plus OFS or 5 years of Tamoxifen alone. OFS choices included oophorectomy, ovarian irradiation or 5 years of TRELSTAR® (Triptorelin), a GnRH (Gonadotropin Releasing Hormone) agonist. The 5 year Disease Free Survival was 91.1% in the AROMASIN® plus OFS group and 87.3% in the Tamoxifen plus OFS group (HR=0.72, P<0.0002). Compared to patients receiving Tamoxifen plus OFS, AROMASIN® plus OFS reduced the relative risk of premenopausal women developing a subsequent invasive breast cancer by 28% and the relative risk of breast cancer recurrence by 34%.
The authors in this analysis examined the absolute treatment effect in the TEXT and SOFT trials across a continuum of recurrence risk, to help individualize decision making for endocrine therapy, in premenopausal women with Human Epidermal growth factor Receptor 2 (HER2) -negative disease. Incorporating age, nodal status, tumor size, grade, Ki-67 expression levels and hormone receptor status, a composite recurrence risk for each patient was determined, from a Cox model.
It was noted that patients in the SOFT trial who remained premenopausal after chemotherapy experienced absolute improvement of 5% or more in 5-year Breast Cancer-Free Interval with AROMASIN® plus OFS compared with Tamoxifen plus OFS or Tamoxifen alone, and this benefit was even higher, reaching 10% to 15% for the intermediate to high composite recurrence risk group of patients. Patients in the SOFT trial whose composite recurrence risk was low did not receive chemotherapy and did well with all endocrine therapies. For patients in the TEXT trial, the benefit of AROMASIN® plus OFS compared with Tamoxifen plus OFS was similar to the SOFT trial, with the 5-year Breast Cancer-Free Interval ranging from 5-15%. Again, patients not receiving chemotherapy and with lowest composite recurrence risk did well with both endocrine therapies.
The authors concluded that premenopausal women with hormone receptor-positive, HER2-negative disease, with high risk for recurrence based on clinicopathologic features, may experience a 10% to 15% improvement in the 5-year Breast Cancer-Free Interval with AROMASIN® plus OFS compared with Tamoxifen alone. Absolute Benefit of Adjuvant Endocrine Therapies for Premenopausal Women with Hormone Receptor–Positive, Human Epidermal Growth Factor Receptor 2–Negative Early Breast Cancer: TEXT and SOFT Trials.Regan MM, Francis PA, Pagani O, et al. Published online before print April 4, 2016, doi: 10.1200/JCO.2015.64.3171 JCO April 4, 2016 JCO643171
FOLFIRINOX Associated with Prolonged Survival in Locally Advanced Pancreatic Cancer
SUMMARY: The American Cancer Society estimates that in 2016, over 53,000 people will be diagnosed with pancreatic cancer in the United States and close to 42,000 patients will die of the disease. Some important risk factors for pancreatic cancer include increasing age, obesity, smoking history, genetic predisposition, exposure to certain dyes and chemicals, heavy alcohol use and pancreatitis. The best chance for long term survival is complete surgical resection, although this may not be feasible in a majority of the patients, as they present with advanced disease at the time of diagnosis. Approximately 35% of patients with pancreatic cancer have unresectable, locally advanced disease at diagnosis. Based on the National Cancer Data Base, the 5 year observed survival rate for patients diagnosed with exocrine cancer of the pancreas is 14% for those with Stage IA disease and 1% for those with Stage IV disease.
In a previously published study (N Engl J Med 2011; 364:1817-1825), FOLFIRINOX regimen, a combination of Fluorouracil, Leucovorin, Irinotecan (CAMPTOSAR®) and Oxaliplatin (ELOXATIN®) was significantly superior to single agent Gemcitabine (GEMZAR®), as first-line therapy, in patients with metastatic pancreatic cancer. FOLFIRINOX resulted in a significantly improved median Overall Survival (OS), median Progression Free Survival (PFS) and Objective Response Rate (ORR).
The researchers in this study evaluated the effectiveness of FOLFIRINOX as first-line treatment in patients with newly diagnosed, locally advanced, unresectable, pancreatic cancer. The authors searched large databases for studies which involved treatment-naive patients of any age, who had received FOLFIRINOX as first-line treatment for locally advanced pancreatic cancer. They were able to include 689 patients from 13 studies, of whom 355 (52%) patients had locally advanced pancreatic cancer. In his retrospective review, the authors looked at Overall Survival as the Primary outcome. Secondary outcomes were Progression Free Survival, rates of Grade 3 or 4 toxicities, proportion of patients who underwent Radiotherapy or Chemoradiotherapy, surgical resection after FOLFIRINOX and R0 resection.
It was noted that across studies, the pooled median OS was 24.2 months, median PFS was 15 months, Grade 3 or 4 adverse events were 60 events per 100 patients and no deaths were attributed to FOLFIRINOX toxicity. The proportion of patients who underwent Radiotherapy or Chemoradiation after FOLFIRINOX ranged from 31% to 100% across studies and the pooled proportion of patients who received any Radiotherapy treatment was 63.5%. The pooled proportion of patients who had surgical resection was 25.9% and the pooled proportion of patients who had R0 resection was 78.4%.
The authors concluded that patients with locally advanced pancreatic cancer treated with FOLFIRINOX had a longer median Overall Survival (24.2 months), compared with single agent GEMZAR® (6-13 months) and future studies should establish which patients might benefit from Radiotherapy or Chemoradiotherapy or surgical resection, following treatment with FOLFIRINOX. FOLFIRINOX for locally advanced pancreatic cancer: a systematic review and patient-level meta-analysis. Suker M, Beumer BR, Sadot, F, et al. Published Online: May 6, 2016. DOI: http://dx.doi.org/10.1016/S1470-2045(16)00172-8