SUMMARY: The FDA on December 7, 2016 approved AVASTIN® (Bevacizumab), either in combination with Carboplatin and Paclitaxel or in combination with Carboplatin and Gemcitabine chemotherapy, followed by AVASTIN® alone, for the treatment of patients with platinum-sensitive recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer. Platinum-sensitive disease is defined as relapse occurring six months or longer following the last treatment with a platinum-based chemotherapy. The American Cancer Society estimates that over 22,280 women will be diagnosed with ovarian cancer in the United States for 2016 and over 14,240 will die of the disease. Ovarian cancer ranks fifth in cancer deaths among women, accounting for more deaths than any other cancer of the female reproductive system. The FDA had approved AVASTIN® in combination with Paclitaxel, Pegylated Liposomal Doxorubicin, or Topotecan in 2014, for the treatment of patients with Platinum-resistant, recurrent epithelial Ovarian, Fallopian tube, or Primary Peritoneal cancer.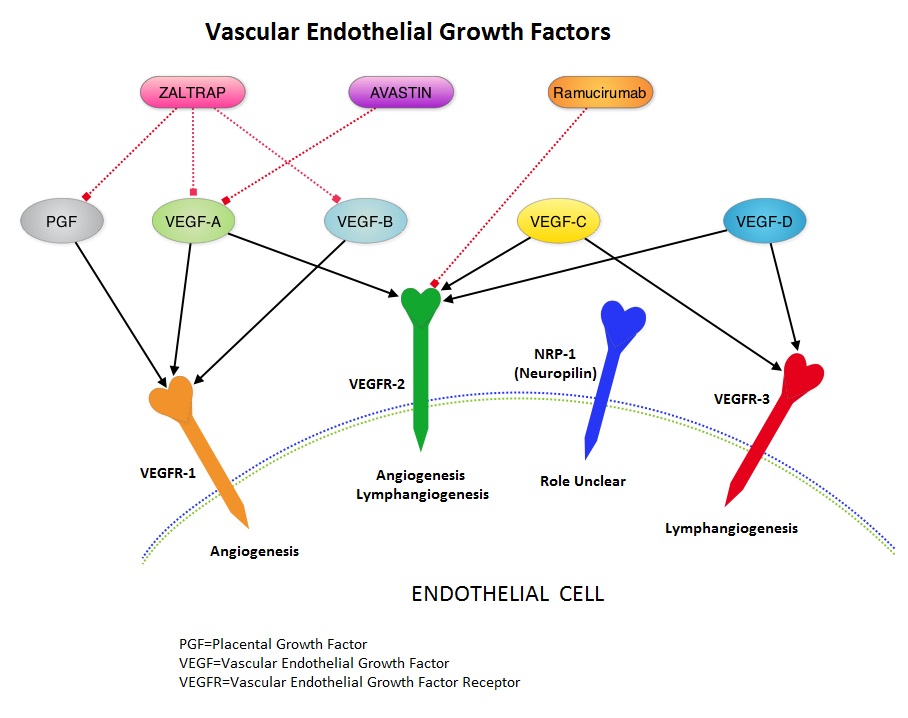
The present approval was based on results from two randomized, controlled Phase III studies, GOG-0213 and OCEANS trial. GOG-0213 is phase III study and was conducted by the Gynecologic Oncology Group (GOG) that enrolled 673 women with platinum-sensitive recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer. This study enrolled 673 patients with predominantly serous adenocarcinoma histology. The patients were randomly assigned to receive combination chemotherapy with Paclitaxel and Carboplatin (N=336) or the same chemotherapy along with Avastin 15 mg/kg IV every 3 weeks (N=337), followed by AVASTIN® maintenance. The median age was 60 years. The Primary endpoint of this study was Overall Survival (OS) and Secondary endpoints included Progression Free Survival (PFS) and Objective Response Rate (ORR).
There was a 5 month improvement in the median Overall Survival with the addition of AVASTIN® to chemotherapy compared with chemotherapy alone (42.6 months vs 37.3 months, respectively; HR=0.84). There was a 3.4 improvement in the median PFS in the AVASTIN® group compared to chemotherapy alone (13.8 months vs 10.4 months, respectively; HR=0.61). The Objective Response Rate (ORR) was 78% with the addition of AVASTIN® to chemotherapy versus 56% with chemotherapy alone.
OCEANS trial is a placebo-controlled, randomized, multicentre Phase III study that evaluated the safety and efficacy of AVASTIN® in combination with Carboplatin and Gemcitabine chemotherapy. This study included 484 patients with platinum-sensitive recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who were randomly assigned to receive combination chemotherapy with Carboplatin and Gemcitabine along with placebo (N=242) or combination chemotherapy along with Avastin (N=242). The Primary endpoint of the study was Progression Free Survival and Secondary endpoints included Objective Response Rate, Overall Survival and safety.
The addition of AVASTIN® to chemotherapy significantly improved PFS compared to chemotherapy alone (12.4 months vs. 8.4 months; HR=0.46, P<0.0001). The ORR was 78% in the AVASTIN® group compared with 57% in the chemotherapy alone group.
These studies supports the use of AVASTIN® either in combination with Carboplatin and Paclitaxel or in combination with Carboplatin and Gemcitabine chemotherapy, followed by AVASTIN® alone, for patients with platinum-sensitive recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer. A phase III randomized controlled clinical trial of carboplatin and paclitaxel alone or in combination with bevacizumab followed by bevacizumab and secondary cytoreductive surgery in platinum-sensitive, recurrent ovarian, peritoneal primary and fallopian tube cancer (Gynecologic Oncology Group 0213). Coleman RL , Bradya MF, Herzog TJ, et al. Scientific Plenary (Late-Breaking Abstract). SGO 2015. Abstract 3. Presented March 28, 2015

 JAKAFI® (Ruxolitinib) is a potent JAK1 and JAK2 inhibitor approved by the FDA in 2011 to treat intermediate or high-risk Myelofibrosis. It is however not indicated for patients with platelet counts under 50,000/μl, and this group represents approximately one third of Myelofibrosis patients and have limited or no treatment options. Previously published PERSIST-1 trial showed that Pacritinib significantly reduced Spleen Volume and Myelofibrosis associated symptoms, in patients with low platelet count, when compared to Best Available Therapy (excluding JAKAFI®).
JAKAFI® (Ruxolitinib) is a potent JAK1 and JAK2 inhibitor approved by the FDA in 2011 to treat intermediate or high-risk Myelofibrosis. It is however not indicated for patients with platelet counts under 50,000/μl, and this group represents approximately one third of Myelofibrosis patients and have limited or no treatment options. Previously published PERSIST-1 trial showed that Pacritinib significantly reduced Spleen Volume and Myelofibrosis associated symptoms, in patients with low platelet count, when compared to Best Available Therapy (excluding JAKAFI®).