
The FDA on July 11, 2017 approved BLINCYTO® for the treatment of relapsed or refractory B-cell precursor Acute Lymphoblastic Leukemia (ALL) in adults and children. BLINCYTO® is a product of Amgen Inc.
Author: RR
NERLYNX ® (Neratinib)
The FDA on July 17, 2017 approved NERLYNX ® for the extended adjuvant treatment of adult patients with early stage HER2-overexpressed/amplified breast cancer, to follow adjuvant Trastuzumab-based therapy. NERLYNX ® is a product of Puma Biotechnology, Inc.
FDA’s First Tissue/Site-Agnostic Approval
The FDA for the first time approved a cancer treatment based on specific genetic biomarker, rather than location in the body where the tumor originated. KEYTRUDA®, an anti-PD1 monoclonal antibody was granted accelerated approval for treatment of adult and pediatric patients with unresectable or metastatic, MicroSatellite Instability-High (MSI-H) or MisMatch Repair deficient (dMMR) solid tumors that have progressed following prior treatment and who have no satisfactory alternative treatment options or with MSI-H or dMMR ColoRectal Cancer that has progressed following treatment with a Fluoropyrimidine, Oxaliplatin, and Irinotecan. MMR gene deficiency can be detected by ImmunoHistoChemistry and MSI testing is performed using a PCR based assay.
FDA Approves ENDARI® for Sickle Cell Disease
The FDA on July 7, 2017 approved ENDARI® (L-Glutamine oral powder) for oral administration to reduce the acute complications of Sickle Cell disease, in adult and pediatric patients 5 years and older. There is a higher L-glutamine utilization in Sickle Cell Anemia resulting in its depletion and thereby contributing to oxidative stress. This oxidative stress is an important contributing factor to hemoglobin polymerization, with polymer formation occurring only in the deoxy state. ENDARI® is the first treatment approved for patients with Sickle Cell disease in almost 20 years.
BAVENCIO® – First FDA Approved Agent for Merkel Cell Carcinoma
SUMMARY: The FDA on March 23, 2017, granted accelerated approval to BAVENCIO® (Avelumab) for the treatment of patients 12 years and older with metastatic Merkel Cell Carcinoma (MCC). It is estimated that about 1500 cases of MCC are diagnosed in the United States each year and the life expectancy for metastatic Merkel Cell Carcinoma is less than 1 year and is associated mortality three times that of Malignant Melanoma (46% vs. 15% respectively). Merkel Cell Carcinoma, also described as Trabecular tumor of the skin, is rare but aggressive form neuroendocrine skin cancer and is much more common in elderly Caucasians. The rapid rise in the incidence of MCC over the past several years has been attributed to increased life expectancy, more sun exposure and weakened immune systems. Approximately 80% of Merkel Cell Carcinoma tumors have been found to be infected with Merkel Cell PolyomaVirus (MCPyV) and the natural history of the MCC has been linked to virus-specific humoral and cellular immune responses. MCC tumors are able to evade the immune system in spite of persistent expression of immunogenic viral proteins. It has been postulated that a high mutation burden associated with Merkel Cell Carcinomas leads to many new antigens being presented to the immune system. Tumor cells as well as tumor-infiltrating immune cells express PD-L1 (Programmed cell Death Ligands), which can contribute to inhibition of antitumor immune response in the tumor microenvironment. The immune system is harnessed and Cytotoxic T-cell activity is suppressed by the binding of PD-L1 to PD-1(Programmed cell Death 1) and B7.1 receptors found on T cells. Merkel Cell Carcinoma is associated with increased PD-L1 expression.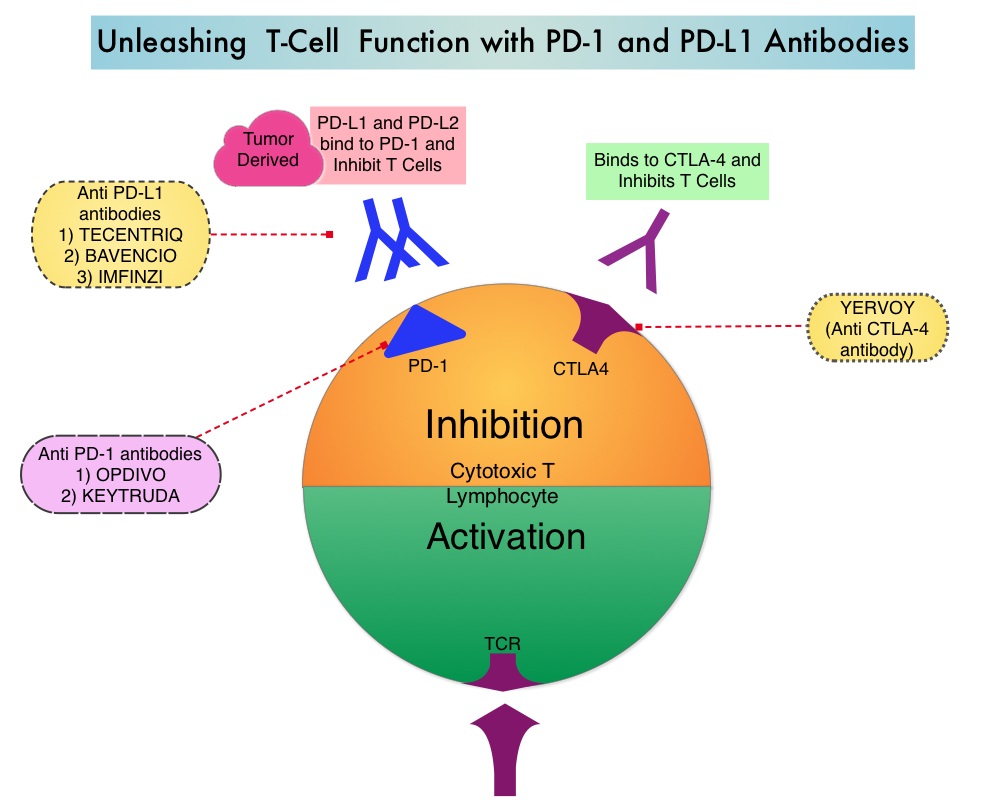
BAVENCIO® is a human, immunoglobulin G1 lambda, PD-L1 targeted monoclonal antibody that binds to PD-L1 and blocks the interaction between PD-L1 and its receptors PD-1. This in turn negates the inhibitory effects of PD-L1 on the immune response by unleashing the immune system and restoring antitumor immune responses. In addition, BAVENCIO® induces Antibody Dependent Cell-mediated Cytotoxicity (ADCC). The approval of BAVENCIO® for Merkel Cell Carcinoma was based on the phase II, prospective, open-label, international JAVELIN trial in which 88 patients with Stage IV Merkel Cell Carcinoma received BAVENCIO® 10 mg/kg IV infusion over 60 minutes, every 2 weeks, until disease progression or unacceptable toxicity. Enrolled patients had at least one prior chemotherapy regimen for metastatic disease. Over 50% of the patients had visceral metastases, two thirds of the patients had tumors with PD-L1 expression of 1% or more, by ImmunoHistoChemistry assay and 52% of the evaluable patients tested positive for Merkel cell Polyomavirus. However, patient selection in this study was not based on the level of PD-L1 expression or Polyomavirus status. The median age was 73 years. The Primary endpoint was Objective Response Rate (ORR). Secondary endpoints included Duration of Response and Progression Free Survival (PFS).
At a median follow up of 16 months, the Objective Response Rate at 1 year was 33% with a Complete Response Rate of 11%. The median time to response was 6 weeks. The 6-month durable response rate was 30.6% and the median Duration of Response had not yet been reached. These responses were noted irrespective of PD-L1 tumor cell expression or presence of Merkel cell Polyomavirus. The estimated one year PFS was 30% and one year Overall Survival was 52%. The most common adverse reactions were rash, fatigue, nausea, diarrhea, decreased appetite, musculoskeletal pain, infusion-related reaction and peripheral edema.
The authors concluded that BAVENCIO® showed durable antitumor activity with a manageable safety profile, in patients with metastatic Merkel Cell Carcinoma who had progressed on chemotherapy and is an important new treatment option for this patient population. BAVENCIO® is the very first drug approved by the FDA for Merkel Cell Carcinoma. Studies are also underway with KEYTRUDA® (Pembrolizumab), a PD-1 inhibitor, in this patient group, with promising outcomes thus far. Durable responses to avelumab (anti-PD-L1) in patients with Merkel cell carcinoma progressed after chemotherapy: 1-year efficacy update. Kaufman HL, Russell JS, Hamid O, et al. 2017 AACR Annual Meeting. Abstract CT079. Presented April 3, 2017.
Brachytherapy for Patients With Prostate Cancer American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update Summary
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer and 1 in 7 men will be diagnosed with Prostate cancer during their lifetime. It is estimated that in the United States, about 161,360 new cases of Prostate cancer will be diagnosed in 2017 and 26,730 men will die of the disease. Brachytherapy for prostate cancer is a type of Internal radiation treatment in which radioactive material sealed inside a seed, pellet, wire, or capsule is implanted in the prostate gland using a needle or catheter. Brachytherapy allows the delivery of higher doses of radiation to the intended site, compared with the conventional form of radiation therapy (External Beam Radiation Therapy).
Types of Brachytherapy
1) Low-dose rate (LDR) implants that stay in the prostate gland for 1 to 7 days and then are taken out.
2) High-dose rate (HDR) implants that stay in the prostate gland for a few minutes at a time and are then taken out.
3) Permanent implants that stay in the prostate gland and are not removed.
Prostate Cancer Risk Categories
Very Low Risk: T1c, Gleason score 6 or less, PSA less than 10 ng/ml, Fewer than 3 prostate biopsy cores positive with 50% or less cancer in each core
Low Risk: T1-T2a, Gleason score 6 or less, PSA less than 10 ng/ml
Intermediate Risk: T2b-T2c and/or Gleason score =7 and/or PSA 10-20 ng/ml
High Risk: T3a or Gleason score 8-10 or PSA more than 20 ng/ml
Very High Risk: T3b-T4
With the gathering of new evidence from randomized trials since the original publication in 2013, a guidelines update became necessary. The scope of this guideline covers Brachytherapy boost and monotherapy. The relevant evidence was evaluated for inclusion in this updated clinical practice guideline after a systematic review of the literature and five randomized controlled trials provided the evidence for this update.
Guideline Questions
1) In patients with newly diagnosed Prostate cancer, what is the efficacy of Brachytherapy alone for clinical outcomes compared with External Beam Radiation Therapy (EBRT) alone, or Radical Prostatectomy (RP) alone?
2) In patients with newly diagnosed Prostate cancer, what is the efficacy of Brachytherapy combined with EBRT for clinical outcomes compared with Brachytherapy alone, EBRT alone, or RP alone?
3) Among the isotopes used for low-dose-rate (LDR) Brachytherapy (eg, Iodine-125 [125I], Palladium-103 [103Pd], and Cesium-131 [131Cs]), which isotope maximizes clinical outcomes when used in patients with newly diagnosed Prostate cancer?
Updated recommendations
1) For patients with low-risk Prostate cancer who require or choose active treatment, LDR brachytherapy alone, EBRT alone, or RP should be offered to those who are eligible.
2) For patients with intermediate-risk Prostate cancer choosing EBRT with or without Androgen Deprivation Therapy (ADT), Brachytherapy boost (LDR or high–dose rate [HDR]) should be offered to eligible patients.
3) For low-intermediate risk Prostate cancer (Gleason 7, PSA 10 ng/mL or Gleason 6, PSA 10 to 20 ng/mL) LDR Brachytherapy alone may be offered as monotherapy.
4) For patients with high-risk Prostate cancer receiving EBRT and ADT, Brachytherapy boost (LDR or HDR) should be offered to eligible patients.
5)125I and 103Pd are each reasonable isotope options for patients receiving LDR Brachytherapy; no recommendation can be made for or against using 131Cs or HDR monotherapy.
6) Patients should be encouraged to participate in clinical trials
Qualifying Statements
1) Patients should be counseled about all of their management options (surgery, EBRT, Brachytherapy, or active surveillance, as applicable) in a balanced, objective manner, preferably by practitioners from multiple disciplines.
2) Recommendations for patients with low-risk disease are unchanged from the initial guideline because no new data from randomized studies informing this question have been presented or published since 2013.
3) Patients ineligible for Brachytherapy may include those with moderate to severe baseline urinary symptoms, large prostate volume, or prior transurethral resection of the prostate, those who are medically unfit, and those with contraindications to radiation treatment.
4) ADT may be given in neoadjuvant, concurrent, and/or adjuvant settings at the physician’s discretion. Note that neoadjuvant ADT may cytoreduce the prostate volume sufficiently to allow Brachytherapy.
5) There may be increased genitourinary toxicity with Brachytherapy compared with use of EBRT alone.
6) Brachytherapy should be performed at a center that has strict quality assurance standards.
7) It cannot be determined whether there is an overall or cause-specific survival advantage for Brachytherapy compared with EBRT alone because none of the trials were designed or powered to detect a meaningful difference in survival outcomes.
Brachytherapy for Patients With Prostate Cancer: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update. Chin J, Rumble RB, Kollmeier M, et al. Journal of Clinical Oncology 2017;35:1737-1743.
Weight Gain Increases the Risk for Postmenopausal Breast cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 255,180 new cases of invasive breast cancer will be diagnosed in 2017 and over 41,070 women will die of the disease. Obesity is an important contributing factor to postmenopausal breast cancer incidence and mortality. Based on recently published meta-analysis, in women diagnosed with breast cancer, there is an approximately 30% increased risk of disease recurrence or death in those who are obese compared to those with ideal body weight. Increasing physical activity may lower the risk of breast cancer recurrence. According to the consensus from the St Gallen Consensus Conference in 2015, obesity has been associated with poor breast cancer outcomes. Obesity is associated with alterations in insulin/glucose homeostasis, adipokines, and sex hormones, which may play a role in breast cancer outcomes. Weight loss can lead to reductions in C-reactive protein, insulin, glucose, and leptin. These mediators have all been implicated to have prognostic significance in breast cancer. 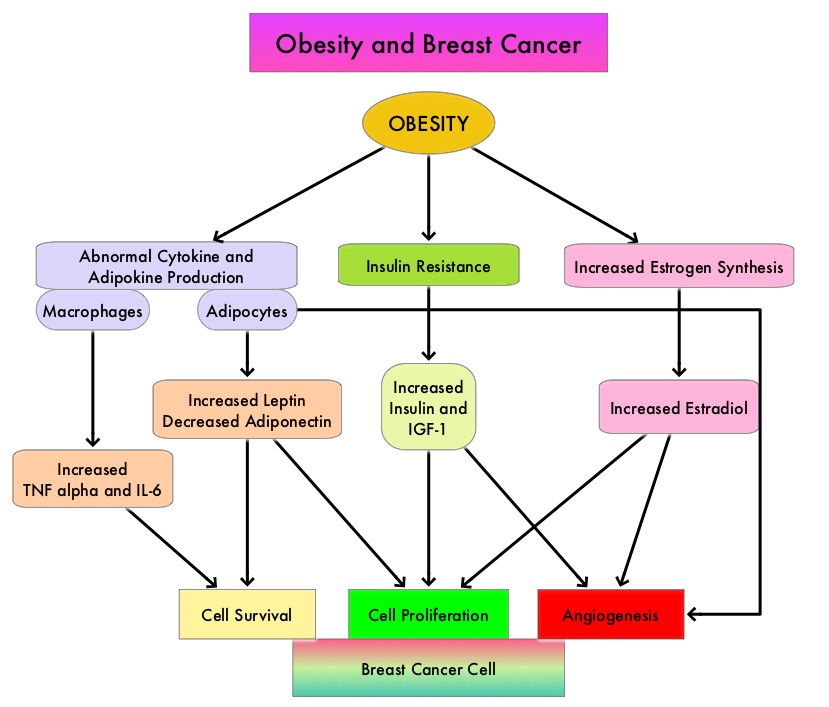
The Nurses’ Health Studies (NHS) are the largest and longest running investigations focused on women’s health. This was established in 1976 and the information provided by its 238,000 dedicated nurse-participants has allowed NHS to produce key advances impacting women’s health. These studies are conducted by researchers at Harvard School of Public Health and Brigham and Women's Hospital in Boston, Massachusetts. The authors conducted a clinical trial in this NHS cohort and studied the effects of weight and weight changes in early adulthood and risk of breast cancer later in life. A prospective observational study was conducted among 74,177 women from the Nurses' Health Study from 1980-2012. These women provided information on breast cancer risk factors such as reproductive factors, hormone therapy, anthropometric variable, benign breast disease, and family history of breast cancer. This information was updated every 2 years up to the time of data analysis. Each individual’s weight at age 18 was collected in 1980.
During the observation period, 4965 cases of invasive breast cancer were reported for the 74,177 women followed from 1980 to 2012. Weight gain over a long period of time from age 18, both during premenopause and postmenopause, were positively associated with postmenopausal breast cancer risk. However, premenopausal weight gain was not related to premenopausal breast cancer risk. Further, weight gain from age 18 yrs onwards was positively associated with ER+/PR+ postmenopausal breast cancer and there was a 50% increased risk for breast cancer with a weight gain of 30 kg. This direct association was not seen for ER+/PR- or ER-/PR- breast cancer. The authors noted that overall, 17% of ER+/PR+ postmenopausal breast cancer and 14% of total postmenopausal breast cancer are attributable to weight gain of more than 5 kg after age 18.
It was concluded that 14% of postmenopausal breast cancer could be prevented if women avoided excessive weight gain of more than 5 kg after age 18. This study adds new insights on weight gain during premenopausal years and risk for postmenopausal breast cancer. Weight and weight changes in early adulthood and later breast cancer risk. Rosner B, Eliassen AH, Toriola AT, et al. Int J Cancer. 2017 Jan 30. doi: 10.1002/ijc.30627 [Epub ahead of print]
FDA Approves ENDARI®, A New Treatment for Sickle Cell Disease
SUMMARY: The FDA on July 7, 2017 approved ENDARI® (L-Glutamine oral powder) for patients age five years and older with Sickle Cell disease to reduce severe complications associated with the blood disorder. Sickle cell disease or Sickle Cell anemia is an Autosomal Recessive disorder and affects approximately 100,000 Americans. It is estimated that it affects 1 out of every 365 African-American births and 1 out of every 16,300 Hispanic-American births. The average life expectancy for patients with Sickle Cell disease in the United States is approximately 40 to 60 years.
HbSS disease or Sickle Cell anemia is the most common Sickle Cell disease genotype and is associated with the most severe manifestations. HbSS disease is caused by a mutation substituting thymine for adenine in the sixth codon of the beta-globin chain gene. This in turn affects the hemoglobin’s ability to carry oxygen and causes it to polymerize. This results in decreased solubility thereby distorting the shape of the red blood cells, increasing their rigidity and resulting in red blood cells that are sickle shaped rather than biconcave. These sickle shaped red blood cells limit oxygen delivery to the tissues by restricting the flow in blood vessels, leading to severe pain and organ damage (vaso-occlusive crises). Oxidative stress is an important contributing factor to hemoglobin polymerization with polymer formation occurring only in the deoxy state. HbS/b-0 thalassemia (double heterozygote for HbS and b-0 thalassemia) is clinically indistinguishable from HbSS disease.
L-glutamine is a precursor for the synthesis of essential metabolic Oxidation-Reduction cofactors including Nicotinamide Adenine Dinucleotide (NAD). It has been shown in previous studies that there is higher L-glutamine utilization in Sickle Cell Anemia resulting in its depletion and thereby contributing to oxidative stress. Based on a phase II study showing favorable outcomes with ENDARI® compared with placebo, a phase III, randomized trial was conducted, in which the safety and efficacy of ENDARI® was studied in 230 Sickle Cell disease or beta-0 thalassemia patients, who had at least two episodes of painful crises during the 12 months before screening. Patients were randomized in a 2:1 ratio to receive ENDARI® (N=152) or placebo (N=78). Enrolled patients were 5-58 yrs old and ENDARI® was administered orally at 0.3 mg/kg/day for 48 weeks followed by a 3 week tapering period. Two thirds of the patients were on Hydroxyurea. The effect of treatment was evaluated over 48 weeks.
Patients who were treated with ENDARI® experienced fewer hospital visits for Sickle Cell crises pain management with parenteral narcotics or Ketorolac compared to those who received a placebo, fewer hospitalizations for Sickle Cell pain , and fewer days in the hospital (median 6.5 days versus median 11 days) compared to those on placebo. Further, patients who received ENDARI® also had fewer occurrences of acute chest syndrome (a life-threatening complication of sickle cell disease), compared with patients who received a placebo (8.6% versus 23.1%). The common side effects of ENDARI® included, nausea, constipation, headache, abdominal pain, cough, pain in the extremities, back pain and chest pain.
It was concluded that the benefit with ENDARI® for patients with Sickle Cell disease, was seen in all age groups and there was a consistent advantage with ENDARI® regardless of whether the patient was on Hydroxyurea or not. ENDARI® is the first treatment approved for patients with Sickle Cell disease in almost 20 years. Phase 3 Study of L-Glutamine Therapy in Sickle Cell Anemia and Sickle ß0-Thalassemia Subgroup Analyses Show Consistent Clinical Improvement. Niihara Y, Viswanathan K, Miller ST, et al. Abstarct#1318. Presented at ASH 58th Annual Meeting & Exposition, San Diego, CA. December 3-6, 2016
Three Months of Adjuvant Therapy Adequate for Stage III Colon Cancer
The IDEA Collaboration is a prospective, pre-planned pooled analysis of 6 concurrently conducted randomized phase III trials, which included 12,834 patients from 12 countries. They concluded that a risk-based approach has to be taken when making adjuvant chemotherapy recommendations for patients with stage III colon cancer. Three months of adjuvant chemotherapy is adequate for patients with T1-3, N1 disease. This study data was presented at 2017 ASCO Annual Meeting.
ENDARI® (L-Glutamine oral powder)
The FDA on July 7, 2017 approved ENDARI® for oral administration to reduce the acute complications of Sickle Cell disease, in adult and pediatric patients 5 years and older. ENDARI® is a product of Emmaus Medical, Inc.