
The FDA on November 16, 2017, approved SUTENT® for the adjuvant treatment of adult patients at high risk of recurrent Renal Cell Carcinoma, following nephrectomy. SUTENT® is a product of Pfizer Inc.
Author: RR
GAZYVA® (Obinutuzumab)
The FDA on November 16, 2017, granted regular approval to GAZYVA® in combination with chemotherapy, followed by GAZYVA® monotherapy, in patients achieving at least a Partial Remission, for the treatment of adult patients with previously untreated Stage II bulky, III, or IV Follicular Lymphoma (FL). GAZYVA® is a product of Genentech, Inc.
SPRYCEL® (Dasatinib)
The FDA on November 9, 2017, granted regular approval to SPRYCEL®, for the treatment of pediatric patients with Philadelphia chromosome-positive (Ph+) Chronic Myeloid Leukemia (CML) in the Chronic Phase. SPRYCEL® is a product of Bristol-Myers Squibb Co.
ADCETRIS® (Brentuximab vedotin)
The FDA on November 9, 2017 granted regular approval to ADCETRIS®, for the treatment of adult patients with primary cutaneous Anaplastic Large Cell Lymphoma (pcALCL) or CD30-expressing Mycosis Fungoides (MF), who have received prior systemic therapy. ADCETRIS® is a product of Seattle Genetics, Inc.
ALECENSA® (Alectinib)
The FDA on November 6, 2017, granted regular approval to ALECENSA®, for treatment of patients with Anaplastic Lymphoma Kinase (ALK)-positive metastatic Non-Small Cell Lung Cancer (NSCLC), as detected by an FDA-approved test. ALECENSA® is a product of Hoffmann-La Roche, Inc./Genentech, Inc.
ZELBORAF® (Vemurafenib)
The FDA on November 6, 2017, granted regular approval to ZELBORAF® for the treatment of patients with Erdheim-Chester Disease (ECD) with BRAF V600 mutation. ZELBORAF® is a product of Hoffmann-La Roche Inc.
FDA Grants Approval to CALQUENCE® for Mantle Cell Lymphoma
SUMMARY: The FDA on October 31, 2017, granted accelerated approval to CALQUENCE® (Acalabrutinib) for the treatment of adult patients with Mantle Cell Lymphoma (MCL) who have received at least one prior therapy. The American Cancer Society estimates that in 2017, about 72,240 people will be diagnosed with Non Hodgkin Lymphoma (NHL) in the United States and about 20,140 individuals will die of this disease. In the US, approximately 3,300 new cases of MCL are diagnosed each year. Mantle Cell Lymphoma is an aggressive B-cell lymphoma and accounts for approximately 6% of all Non Hodgkin Lymphomas in adults, and is associated with a high relapse rate, following dose-intensive therapies. Early and late relapses in patients with MCL have been attributed to persistence of residual disease.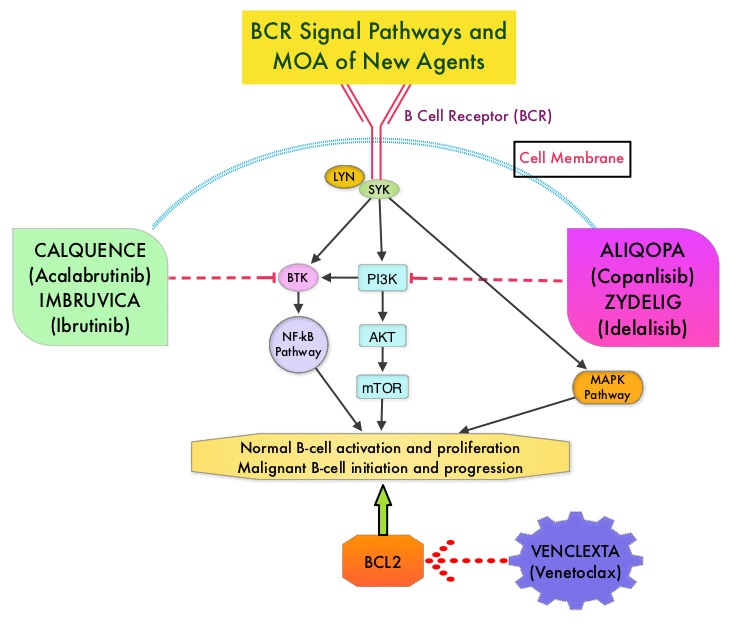
Normal B-cell activation and proliferation is dependent on B-cell receptor (BCR) signaling. This signaling is also important for initiation and progression of B-cell lymphoproliferative disorders. Bruton’s Tyrosine Kinase (BTK) is a member of the Tec family of kinases, downstream of the B-cell receptor and is predominantly expressed in B-cells. It is a mediator of B-cell receptor signaling in normal and transformed B-cells. Following binding of antigen to the B-Cell Receptor, kinases such as Syk (Spleen Tyrosine Kinase), Lyn (member of the Src family of protein tyrosine kinases) and BTK (Bruton’s Tyrosine Kinase) are activated, with subsequent propagation through PI3K/Akt, MAPK, and NF-κB pathways. This results in B-cell activation and proliferation. Three previously approved agents by the FDA for MCL include, IMBRUVICA® (Ibrutinib), REVLIMID® (Lenalidomide) and VELCADE® (Bortezomib).
CALQUENCE® is a novel, irreversible, second-generation BTK inhibitor, designed to be more potent and selective than IMBRUVICA®. Unlike IMBRUVICA®, CALQUENCE® has reduced off-target activity on EGFR, TEC, etc., which may lead to less untoward toxicities such as bleeding, rash, and atrial fibrillation. The approval of CALQUENCE® was based on ACE-LY-004 study, which is a Phase II, open label, single-arm clinical trial, in which 124 adult patients with Relapsed or Refractory MCL were enrolled. Patients had a confirmed diagnosis of MCL, 93% of the patients had an ECOG PS of 1 or less, median number of prior treatments were 2, which included stem cell transplant for 18% of patients, and 24% of the patients were refractory to their most recent prior treatment. Those treated with a prior BTK inhibitor were excluded from this study. The median age was 68 years. CALQUENCE® was administered orally at 100 mg twice daily until progressive disease or unacceptable toxicity. The Primary endpoint was Objective Response Rate (Complete Response + Partial Response) and Secondary endpoints included Duration of Response (DOR), Progression Free Survival (PFS), Overall Survival (OS) and safety.
At a median follow up of 15.2 months, the Objective Response Rate was 81% with a Complete Response rate of 40% and Partial Response rate of 41%. The median Duration of Response was not yet reached at the time of analysis, with ongoing responses at 20+ months. The response rates were consistent across prespecified subgroups of age, tumor bulk of 10 cm or more and number and types of prior treatment. The median time to best response was 1.9 months. The median Duration of Response (DOR) was not reached and the 12-month DOR was 72%. The median PFS and OS were not reached, whereas the 12-month PFS and OS rates were 67% and 87% respectively. The most common toxicities of any grade included cytopenias, headache, diarrhea, fatigue, myalgia and bruising.
It was concluded that for patients with Relapsed/Refractory Mantle Cell Lymphoma, CALQUENCE® given as a single agent resulted in a high and durable Objective Response Rate as well as Complete Response Rate, with a favorable safety profile. CALQUENCE® is a new treatment option for this aggressive malignancy. Efficacy and Safety of Acalabrutinib Monotherapy in Patients with Relapsed/Refractory Mantle Cell Lymphoma in the Phase 2 ACE-LY-004 Study. Wang M, Rule S, Zinzani PL, et al. 59th Annual Meeting & Exposition Atlanta, GA. December 9-12, 2017. #155
Alcohol and Cancer A Statement of the American Society of Clinical Oncology
SUMMARY: It has been estimated that in the United States, 3-4% of all cancer deaths are attributable to drinking alcohol. According to the Centers for Disease Control and Prevention, approximately 88,000 deaths were attributed to excessive alcohol use in the United States between 2006 and 2010. Alcohol consumption is an established risk factor for several malignancies, and is a potentially modifiable risk factor for cancer. The International Agency for Research on Cancer (IARC), a branch of WHO, classified alcohol as a group 1 carcinogen. The Cancer Prevention Committee of the American Society of Clinical Oncology has now provided an overview of the evidence of the links between alcohol drinking and cancer risk and cancer outcomes.
DRINKING GUIDELINES AND DEFINITIONS
The American Heart Association, American Cancer Society, and US Department of Health and Human Services all recommend that men limit intake to one to two drinks per day and women to one drink per day. People who do not currently drink alcohol should not start for any reason. A standard drink is defined as one that contains roughly 14 g of pure alcohol, which is the equivalent of 1.5 ounces of distilled spirits, 5 ounces of wine or 12 ounces of regular beer. Moderate drinking is defined at up to one drink per day for women and up to 2 drinks per day for men whereas heavy drinking is defined as 8 or more drinks per week or 3 or more drinks per day for women, and as many as 15 or more drinks per week or 4 or more drinks per day for men. Hispanics and blacks have a higher risk than whites, for developing alcohol-related liver disease. Use of alcohol during childhood and adolescence is a predictor of increased risk of alcohol related disorders later in life.
ROLE OF ALCOHOL IN CARCINOGENESIS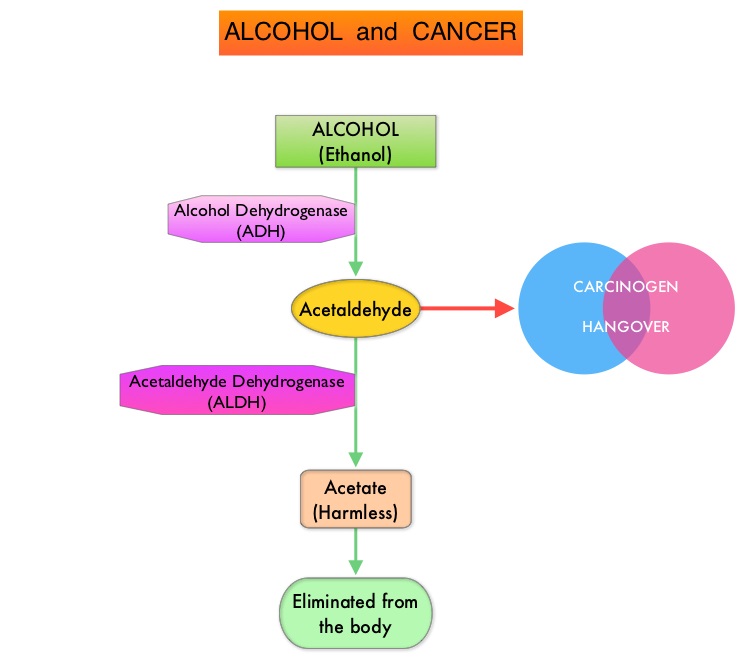
Alcohol is predominantly metabolized in the liver to acetaldehyde, which is a carcinogen and is responsible for many “hangover” symptoms. Acetaldehyde is then converted into harmless acetic acid radicals also known as acetyl radicals, and eliminated from the body. There is strong evidence to suggest that acetaldehyde damages DNA. Acetaldehyde generated during alcohol metabolism in the human body is eliminated by Aldehyde Dehydrogenase-2 (ALDH2). However, a genetic variant of ALDH2, which is an inactive form, exists and individuals with the inactive form of ALDH2 who consume alcohol, accumulate excessive amounts of acetaldehyde, which in turn can lead to greater susceptibility to alcohol-induced cancer. It has been noted that this high-risk genotype in prevalent in about 50% of North East Asian population and in 5–10% of blond-haired blue-eyed people of Northern European descent. Alcohol consumption in this group is more strongly associated with cancers of the upper aerodigestive tract. Breast tissue is also more susceptible to alcohol than other sites. Even moderate alcohol intake has been associated with increased levels of circulating sex hormones, which in turn can activate cellular proliferation. Alcohol consumption is associated with lower serum folate concentrations and this may play a role in the etiology of colon cancer.
ALCOHOL AND CANCER
There is a clear association between alcohol and upper aerodigestive tract cancers (larynx, esophagus, and oral cavity/pharynx), as a result of direct contact of ingested alcohol with the involved tissues.
Continued alcohol use among survivors of upper aerodigestive tract cancers is associated with a 3 fold increase in the risk of a second primary tumor in the upper aerodigestive tract. Additionally, there is a synergistic interaction between alcohol consumption and cigarette smoking. Smoking and alcohol use during and after radiation therapy have been associated with an increased risk of osteoradionecrosis of the jaw, in patients with oral and oropharyngeal cancers.
Among women with Estrogen Receptor-positive breast cancer, those consuming 7 or more drinks per week have a 90% increased risk of asynchronous contralateral breast cancer, versus those who do not consume alcohol. It is estimated that there is a 5% increase in premenopausal breast cancer per 10 grams of ethanol consumed per day and the risk is even greater at 9%, for postmenopausal breast cancer.
A recent meta-analysis of cohort studies among 209,597 cancer survivors showed an 8% increase in overall mortality and a 17% increased risk for recurrence in the highest versus lowest alcohol consumers and these numbers were statistically significant.
The benefit of alcohol consumption on cardiovascular health likely has been overstated and nondrinkers have lower rates of coronary heart disease and stroke than even light drinkers. Given the increase in the risk of cancer even with low levels of alcohol consumption, the net effect of alcohol is harmful. Alcohol consumption should therefore not be recommended to prevent cardiovascular disease or all-cause mortality.
In conclusion, alcohol is a well-established risk factor for the development of certain cancers and further research is needed to understand the effects of alcohol exposure on the efficacy of chemotherapy, immunotherapy and radiation treatment. Alcohol and Cancer: A Statement of the American Society of Clinical Oncology. LoConte NK, Brewster AM, Kaur JS, et al. DOI: 10.1200/JCO.2017.76.1155 Journal of Clinical Oncology – published online before print November 7, 2017
CALQUENCE® (Acalabrutinib)
The FDA on October 31, 2017 granted accelerated approval to CALQUENCE® for treatment of adult patients with Mantle Cell Lymphoma (MCL) who have received at least one prior therapy. CALQUENCE® is a product of AstraZeneca Pharmaceuticals Inc. under license of Acerta Pharma BV.
YESCARTA® (Axicabtagene ciloleucel)
The FDA on October 18, 2017 granted regular approval to YESCARTA®, for the treatment of adult patients with relapsed or refractory large B-cell lymphoma after two or more lines of systemic therapy, including Diffuse Large B-Cell Lymphoma (DLBCL) Not Otherwise Specified, Primary Mediastinal large B-cell Lymphoma, high-grade B-cell lymphoma, and DLBCL arising from Follicular lymphoma. YESCARTA® is a product of Kite Pharma, Inc.