
SUMMARY: The FDA recently assigned a priority review designation to Daratumumab, as a treatment for patients with double refractory Myeloma. Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, close to 27,000 new cases will be diagnosed in 2015 and 11,240 will die of the disease. The choice of first line therapy for patients with Myeloma may depend on transplant eligibility, comorbid conditions, cytogenetics and patient performance status. Following progression on first line therapy, single agent therapy with KYPROLIS® (Carfilzomib) has an Objective Response Rate of 24%, with a median duration of response of 7.4 months, in patient groups refractory to both VELCADE® (Bortezomib) and REVLIMID® (Lenalidomide). POMALYST® (Pomalidomide) in combination with Dexamethasone is superior to high dose Dexamethasone alone, with a significant improvement in the Progression Free Survival and Overall Survival, in patients with relapsed and refractory Multiple Myeloma. More recently, data became available for three triplet regimens in patients with relapsed Myeloma – 1) The addition of KYPROLIS® to REVLIMID® and Dexamethasone resulted in significant improvement in Progression Free Survival, when compared with REVLIMID® and Dexamethasone alone, in patients with relapsed Multiple Myeloma 2) A combination of FARYDAK® (Panobinostat), a histone deacetylase (HDAC) inhibitor, VELCADE® and Dexamethasone significantly improves Progression Free Survival in patients with relapsed and refractory Multiple Myeloma when compared to VELCADE® and Dexamethasone 3) Elotuzumab (HuLuc63), a monoclonal antibody that binds to the Signal Lymphocyte Activation Molecule – SLAMF7 protein (CS1, CD319), when added to REVLIMID® and Dexamethasone, reduced the risk of disease progression by 30% in patients with Relapsed/Refractory Multiple Myeloma, when compared with REVLIMID® and Dexamethasone.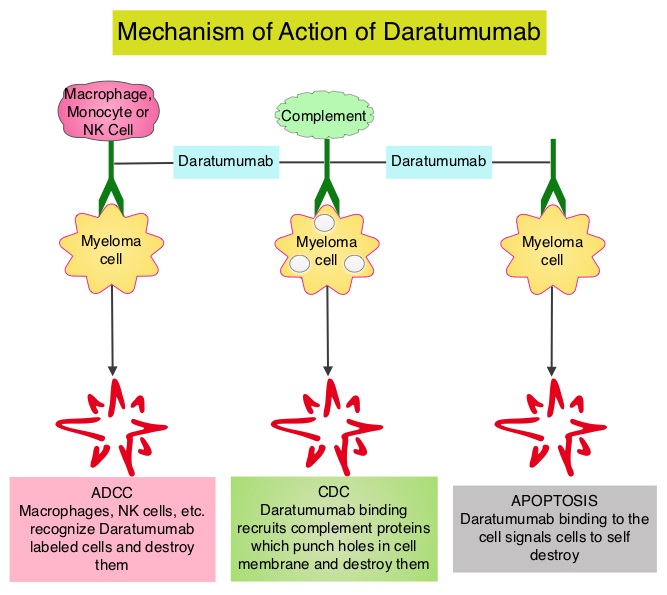
Daratumumab is a human IgG1 antibody that targets CD38, a transmembrane glycoprotein abundantly expressed on malignant plasma cells and with low levels of expression on normal lymphoid and myeloid cells. Daratumumab exerts its cytotoxic effect on myeloma cells by multiple mechanisms, including Antibody Dependent Cellular Cytotoxicity (ADCC), complement mediated cytotoxicity and direct apoptosis. Based on the anti-myeloma activity of Daratumumab in preclinical studies, a phase 1–2 clinical trial was conducted which involved patients with relapsed and refractory Myeloma, who were refractory to two or more prior lines of therapy. Patients in this study had received a median of four previous lines of therapy, 79% of the patients had disease that was refractory to their most recent therapy, including proteasome inhibitors and immunomodulators and 76% of the patients had also undergone autologous stem cell transplantation. This trial included a dose-expansion phase in which 30 patients received Daratumumab 8 mg/kg and 42 patients received 16 mg/kg, given once weekly for 8 doses, twice monthly for 8 doses, and monthly for up to 24 months. The primary end point was safety determined by frequency and severity of adverse events. Secondary end points included Objective Response Rate, duration of response, time to disease progression, Progression Free Survival, Overall Survival and pharmacokinetics.
It was noted that in the cohort that received Daratumumab 16 mg/kg, the overall response rate was 36% with a median Progression Free Survival of 5.6 months and 65% of the patients who had a response did not have disease progression at 12 months.
Infusion related reactions were mild and only 1% had grade 3 events. The other most common adverse events were pneumonia and thrombocytopenia. The authors concluded that Daratumumab has significant single agent activity in a very heavily pretreated and refractory Myeloma patient population, with a favorable safety profile. It remains to be seen if Daratumumab will be an important component of the induction, consolidation and maintenance phases, in the Myeloma treatment landscape. Targeting CD38 with Daratumumab Monotherapy in Multiple Myeloma. Lokhorst HM, Plesner T, Laubach JP, et al. N Engl J Med 2015; 373:1207-1219
