
SUMMARY: The American Cancer Society estimates that in 2019, about 74,200 people will be diagnosed with Non Hodgkin Lymphoma (NHL) in the United States and about 19,970 individuals will die of this disease. Indolent Non Hodgkin Lymphomas are mature B cell lymphoproliferative disorders and include Follicular Lymphoma, Nodal Marginal Zone Lymphoma (NMZL), Extranodal Marginal Zone Lymphoma (ENMZL) of Mucosa-Associated Lymphoid Tissue (MALT), Splenic Marginal Zone Lymphoma (SMZL), LymphoPlasmacytic Lymphoma (LPL) and Small Lymphocytic Lymphoma (SLL). Follicular Lymphoma is the most indolent form and second most common form of all NHLs and they are a heterogeneous group of lymphoproliferative malignancies. Approximately 20% of all NHLs are Follicular Lymphomas (FL).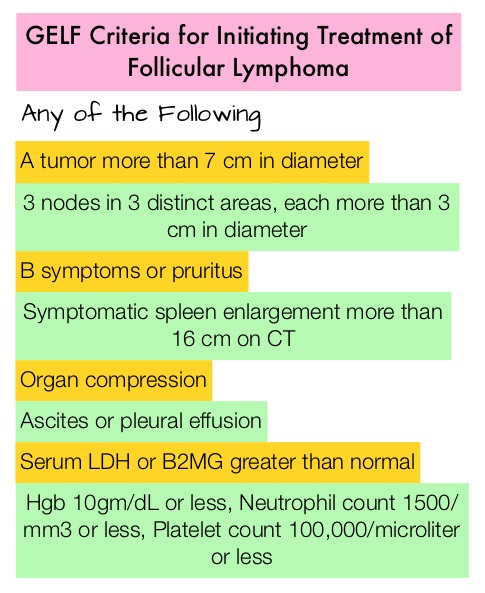
The Ann Arbor classification divides FL into four stages. Patients with Stages I and II have localized disease and those with Stages III and IV have advanced disease. The World Health Organization (WHO) further classified FL based on histology into low grade (grades 1 and 2) and high grade (grade 3a) FLs. Grade 3b FL which demonstrates diffuse areas of involvement is designated as Diffuse Large B-cell Lymphoma (DLBCL) and is treated as such. Advanced stage indolent NHL is not curable and as such, prolonging Progression Free Survival (PFS) and Overall Survival (OS), while maintaining Quality of Life, have been the goals of treatment intervention. Asymptomatic patients with indolent NHL are generally considered candidates for “watch and wait” approach. Patients with advanced stage symptomatic Follicular Lymphoma are often treated with induction chemoimmunotherapy followed by maintenance RITUXAN® (Rituximab). This can result in a median PFS of 6-8 yrs and a median OS of 12-15 yrs. However, approximately 30% of the patients will relapse in 3 years and treatment options are limited for patients with relapses, after multiple treatments.
REVLIMID® (Lenalidomide) is an oral immunomodulatory agent (IMiD) with activity in lymphoid malignancies, primarily through immune modulation, by reactivating and heightening immune system responses to malignant cells. REVLIMID® synergizes with anti-CD20 antibodies such as RITUXAN® and GAZYVA® (Obinutuzumab) and enhances the function of T and NK cells, increases Antibody-Dependent Cellular Cytotoxicity (ADCC), and repair defective synapse formation in B-cell lymphoma cells, thereby restoring the immune system’s ability to kill tumor cells, without permanently damaging the healthy microenvironment, or causing long-term immune suppression. Chemo-free combination immunotherapy with REVLIMID® and RITUXAN® or the R2 regimen, has shown promising activity in phase II studies. RELEVANCE phase III trial compared REVLIMID® plus RITUXAN®, followed by RITUXAN® maintenance, with the standard of care treatment of RITUXAN® plus chemotherapy, followed by RITUXAN® maintenance, in patients with previously untreated Follicular Lymphoma and concluded that R2 regimen showed similar efficacy, with a more favorable safety profile, making it a potential chemo-free first line option, for patients with Follicular Lymphoma. Single agent RITUXAN® is commonly used in the second-line treatment of Follicular Lymphoma (25-47% of patients), according to studies in the United States and Europe.
AUGMENT trial is a prospective, Phase III, multicenter, randomized study in which 358 patients with relapsed or refractory grades 1-3a Follicular Lymphoma (82%) or Marginal Zone Lymphoma (18%) were randomly assigned to receive either REVLIMID® plus RITUXAN® (N=178) or placebo plus RITUXAN® (N=180). Eligible patients had at least one prior chemotherapy, immunotherapy, or chemoimmunotherapy and two or more previous doses of RITUXAN®, and had relapsed, refractory, or progressive disease, but not RITUXAN®-refractory. Patients with greater than grade 1 neuropathy were excluded. The median age was 63 years, over 50% of the patients had high tumor burden based on GELF criteria, and over 40% of patients had at least 2 prior systemic regimens. REVLIMID® plus RITUXAN® regimen consisted of REVLIMID® 20 mg orally daily (10 mg for Creatinine Clearance 30-59 mL/min) on days 1 to 21 plus RITUXAN® 375 mg/m2 IV on days 1, 8, 15, and 22 of cycle 1 and day 1 of cycles 2 to 5 every 28 days for 12 cycles. Placebo plus RITUXAN® was administered similarly. The Primary end point was PFS assessed by the Independent Review Committee (IRC) and Secondary end points included Overall Response Rate (ORR), Complete Response (CR), Duration of Response, Overall Survival (OS), and time to next anti-lymphoma treatment. The median follow-up was 28.3 months.
The median PFS was 39.4 months in the REVLIMID®/ RITUXAN® group versus 14.1 months in the placebo plus RITUXAN® group (HR=0.46, P<0.001). This meant a reduced risk of disease progression by 54% and increased median PFS by more than 2 years compared with RITUXAN® monotherapy. This benefit was consistent across all prespecified subgroups, except for the Marginal Zone Lymphoma subgroup and it may be difficult to draw strong conclusions in this small subgroup because these patients made up only 18% of the overall patient population. Response rates as assessed by IRC were 78% in the REVLIMID®/ RITUXAN® group versus 53% in the placebo plus RITUXAN® group (P<0.001), with Complete Response occurring in 34% versus 18% respectively (P=0.001). The median Duration of Response was 36.6 versus 21.7 months (P =0.0015), median Event-Free Survival was 27.6 versus 13.9 months (HR = 0.51, P<0.001) and the median time to next anti-lymphoma treatment was Not Reached versus 32.2 months (P=0.007).
It was concluded that the R2 regimen (REVLIMID® plus RITUXAN®) significantly prolonged Progression Free Survival in patients with relapsed or refractory indolent lymphoma and represents an important new treatment option for this patient group. AUGMENT: A Phase III Study of Lenalidomide Plus Rituximab Versus Placebo Plus Rituximab in Relapsed or Refractory Indolent Lymphoma. Leonard JP, Trneny M, Izutsu K, et al. J Clin Oncol 2019;37:1188-1199.
