
SUMMARY: The American Cancer Society estimates that in 2017, approximately 79,030 new cases of Bladder Cancer will be diagnosed and 16,870 patients will die of the disease. Patients with urothelial carcinoma are currently treated in the first line setting with a platinum based chemotherapy regimen. Treatment options for patients who progress after platinum based chemotherapy are limited, with poor outcomes. The response rates with standard chemotherapy in this patient population, is about 10%.
The FDA approved KEYTRUDA® (Pembrolizumab) in May 2017 for the treatment of patients with locally advanced or metastatic urothelial carcinoma who have disease progression during or following platinum-containing chemotherapy, or within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy. The FDA subsequently in July 2017 granted an accelerated approval to frontline KEYTRUDA® for patients with locally advanced or metastatic urothelial carcinoma, who are not eligible for cisplatin-containing chemotherapy. KEYTRUDA® is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2. By doing so, it unleashes the tumor-specific effector T cells, and is thereby able to undo PD-1 pathway-mediated inhibition of the immune response. 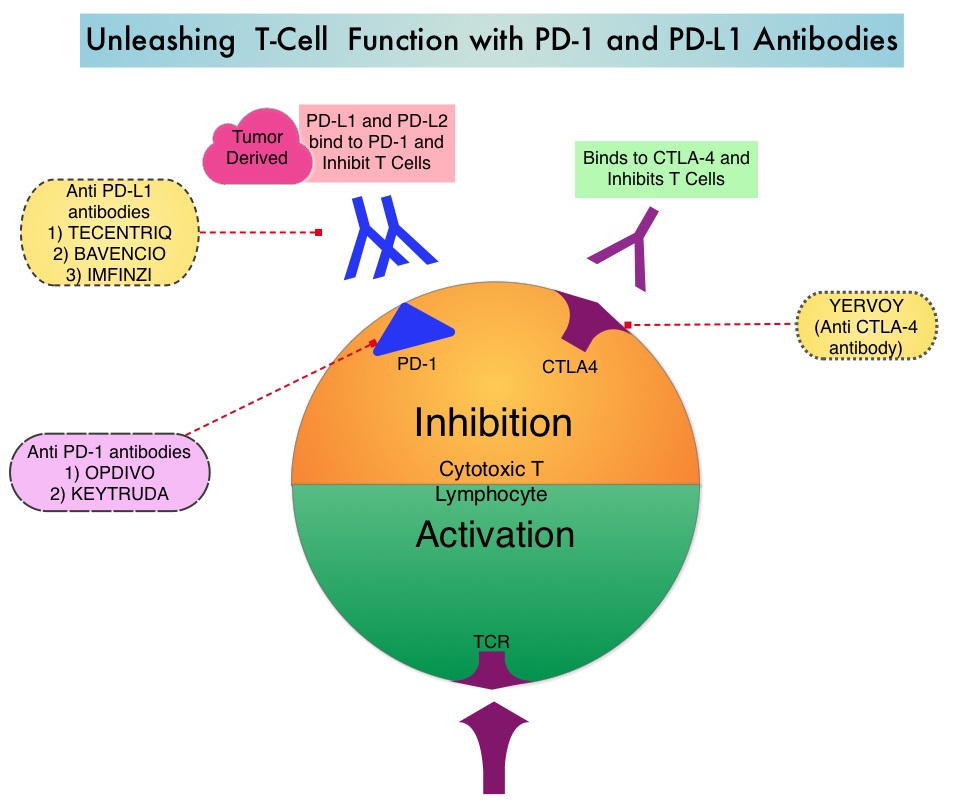
KEYNOTE-045 trial is an open-label, multicenter, phase III study in which 542 patients with advanced urothelial carcinoma who had progressed on prior therapies were randomly assigned to receive KEYTRUDA® or investigator's choice of Paclitaxel, Docetaxel, or Vinflunine. Eligible patients had histologically or cytologically confirmed urothelial carcinoma and had progressed on no more than 2 prior systemic therapies, including a platinum based regimen. Patients were randomly assigned in a 1:1 ratio to receive KEYTRUDA® 200 mg every 3 weeks (N=270) or investigator's choice of Paclitaxel 175 mg/m2 , Docetaxel 75 mg/m2, or Vinflunine 320 mg/m2, every 3 weeks (N=272). The primary endpoints were Overall Survival (OS) and Progression Free Survival (PFS), and the secondary endpoints included Objective Response Rate (ORR) and Safety. Efficacy was assessed in all patients as well as in patients with a PD-L1 Combined Positive Score (CPS) of 10% or more. (CPS is the percentage of PD-L1-expressing tumor and inflammatory cells).
In an updated analysis, with a median follow up of 22.5 months for both treatment groups, the median OS with KEYTRUDA® was 10.3 months compared with 7.4 months with chemotherapy (HR=0.70; P=0.0003) and among patients with a Combined Positive Score of 10% or more, the OS was 8.0 versus 5.2 months respectively (HR=0.58; P=0.003). The OS benefit was noted regardless of age, liver metastases, hemoglobin, visceral disease, and choice of chemotherapy. The 18 month OS rate was 33.2% with KEYTRUDA® versus 19.7% with chemotherapy. There was however no significant difference in the median PFS between the two treatment groups. The ORR was 21.1% with KEYTRUDA® and 11.0% with chemotherapy and the responses with KEYTRUDA® were more durable than with chemotherapy. The median response duration of response was not reached in the KEYTRUDA® group versus 4.4 months in the chemotherapy group. Treatment-related Adverse Events of any grade occurred in 62% of patients in the KEYTRUDA® group and 91% of patients in the chemotherapy group. Discontinuation due to toxicities occurred in 7.1% versus 12.5% of KEYTRUDA® vs chemotherapy patients, respectively.
It was concluded that KEYTRUDA® is the first agent to improve Overall Survival over chemotherapy, in the second line setting, for patients with recurrent, advanced urothelial carcinoma, and a significant proportion of patients who respond, have very durable responses. Pembrolizumab (pembro) versus paclitaxel, docetaxel, or vinflunine for recurrent, advanced urothelial cancer (UC): mature results from the phase 3 KEYNOTE-045 trial. De Wit R, Vaughn DJ, Fradet Y, et al. Annals of Oncology (2017) 28 (suppl_5): v605-v649. 10.1093/annonc/mdx440
