
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, 32,110 new cases will be diagnosed in 2019 and 12,960 patients are expected to die of the disease. Multiple Myeloma (MM) in 2019 remains an incurable disease. The therapeutic goal therefore is to improve Progression Free Survival (PFS) and Overall Survival (OS). Almost all patients eventually will relapse, and patients with a high-risk cytogenetic profile or refractory disease have the worst outcomes.
Chimeric Antigen Receptor (CAR) T-cell therapy has been associated with long-term disease control in some hematologic malignancies and is emerging as a novel treatment for patients with Relapsed and Refractory Multiple Myeloma. B-cell Maturation Antigen (BCMA) is a member of the Tumor Necrosis Factor superfamily of proteins. It is a transmembrane signaling protein primarily expressed by malignant and normal plasma cells and some mature B cells. BCMA is involved in JNK and NF-kB signaling pathways that induce B-cell development and autoimmune responses. BCMA has been implicated in autoimmune disorders as well as B-lymphocyte malignancies, Leukemia, Lymphomas, and Multiple Myeloma.
Anti-BCMA CAR T-Cell Therapy bb2121 is a type of immunotherapy and consists of T cells collected from the patient’s blood in a leukapheresis procedure. These T cells are then stimulated by treating with interleukin 2 (IL-2) and anti-CD3 antibodies in vitro, so that they will actively proliferate and expand to large numbers. These T cells are then genetically engineered to produce special receptors on their surface called Chimeric Antigen Receptors (CAR), by transducing with a gene encoding the engineered CAR, via a retroviral vector such as lentiviral vector. These reprogrammed cytotoxic T cells with the Chimeric Antigen Receptors on their surface are now able to recognize a specific antigen such as BCMA on tumor cells. These genetically engineered and reprogrammed CAR T-cells are grown in the lab and are then infused into the patient. These cells in turn proliferate in the patient’s body and the engineered receptor on the cell surface help recognize and kill cancer cells that expresses that specific antigen such as BCMA. The patient undergoes lymphodepletion chemotherapy with Fludarabine and Cytoxan prior to the introduction of the engineered CAR T-cells. By depleting the number of circulating leukocytes, cytokine production is upregulated and reduces competition for resources, which in turn promotes the expansion of the engineered CAR T-cells. In a mouse model of human Multiple Myeloma, a single-dose administration of bb2121 showed rapid and durable tumor responses, with 100% survival. On the basis of these findings, the authors conducted a Phase 1 clinical study (CRB-401) of bb2121 involving patients with Relapsed or Refractory Multiple Myeloma and reported the initial results from this ongoing study.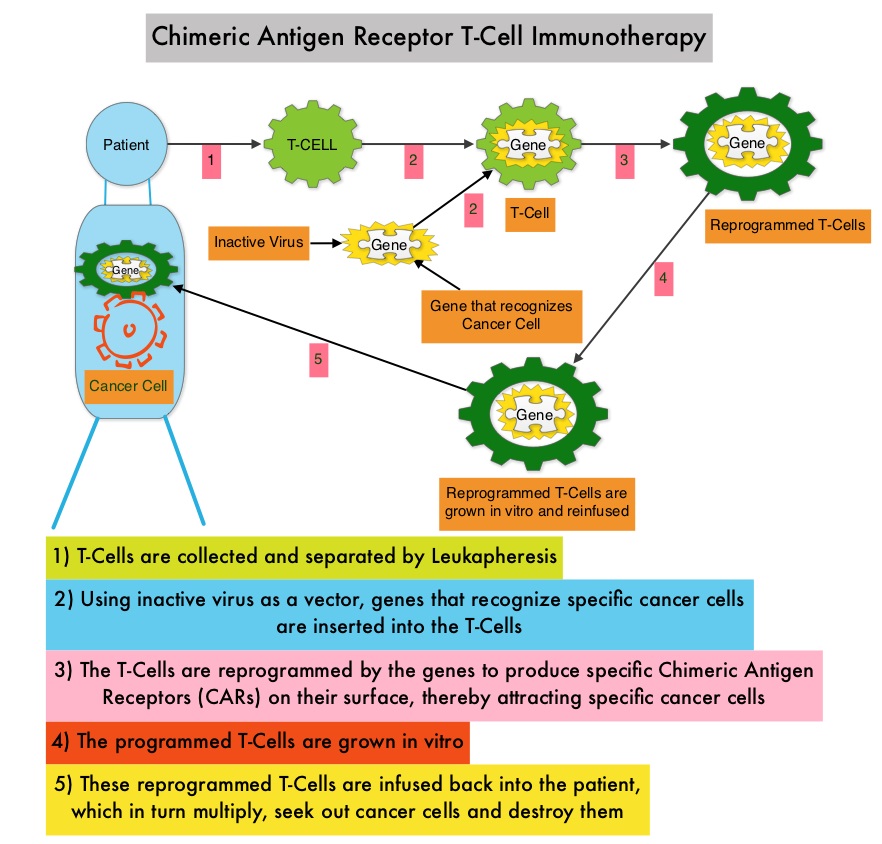
A total of 36 consecutive patients were enrolled in the study and underwent leukapheresis. Patients received bb2121 as a single infusion at increasing doses in the dose-escalation phase (50×106, 150×106, 450×106, or 800×106 CAR T-cells) followed by a dose expansion phase. The median number of previous treatment regimens was 7, and most of the enrolled patients had received previous Autologous Stem-Cell Transplantation. Further, all the patients had previously received both VELCADE® (Bortezomib) and REVLIMID® (Lenalidomide), and more than 75% of patients were exposed to VELCADE®, KYPROLIS® (Carfilzomib), REVLIMID®, POMALYST® (Pomalidomide) and DARZALEX® (Daratumumab). The median patient age was 60 years and the median time from diagnosis was 5 years. Approximately two thirds of the patients had Stage II or III disease, 27% had extramedullary disease, and 45% had a high-risk cytogenetic profile, defined by the presence of del(17p), t(4;14), or t(14;16). The Primary end point was Safety. The median duration of follow up after bb2121 infusion was 11.3 months.
Hematologic Grade 3 Adverse Events manifesting as cytopenias were the most common. Approximately 70% of patients had Grade 1 or 2 Cytokine Release Syndrome (CRS) and 6% had Grade 3 CRS. Approximately 40% of patients had Grade 1 or 2 neurotoxicity.
The Objective Response Rate was 85%, with 45% Complete Responses. The median time to first Partial Response or better was 30 days. The median Duration of Response was 10.9 months. Response rates were independent of tumor BCMA expression. All patients who had a Partial Response or better and who could be evaluated for Minimal Residual Disease (MRD) had MRD-negative status (10−4 or less nucleated cells). CAR T-cells persisted for up to 1 year after the infusion and CAR T-cell expansion was associated with responses. The median Progression Free Survival was 11.8 months.
It was concluded that, CAR T-cell therapy with bb2121 showed promising efficacy at dose levels of 150×106 or more CAR T-Cells, in a heavily pretreated population of patients with Multiple Myeloma. The authors added that non-hematologic toxicities were grade 2 or lower. Anti-BCMA CAR T-Cell Therapy bb2121 in Relapsed or Refractory Multiple Myeloma. Raje N, Berdeja J, Lin Y, et al. N Engl J Med 2019;380:1726-1737
