
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease. Majority of the breast cancer patients present with early stage disease without macroscopic metastatic disease. Several small proof of principle studies have shown that detection of circulating tumor DNA (ctDNA) in the peripheral blood may identify patients at risk of relapse following definitive therapy. ctDNA refers to DNA fragments that are shed into the bloodstream by cancer cells after apoptosis or necrosis. ctDNA can detect almost all molecular alterations present in cancer cells and the proportion of ctDNA that originates from a tumor depends on the anatomic location, tumor burden and cell turnover. ctDNA allows real-time monitoring for treatment response and resistance.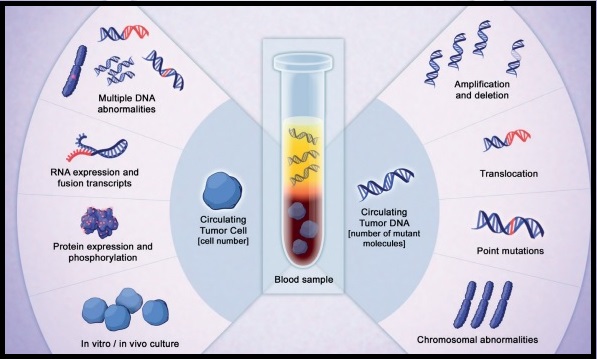
To assess the clinical validity of molecular relapse detection with circulating tumor DNA (ctDNA) analysis in early-stage breast cancer, the authors conducted a multicenter, prospective study in the UK over a 5 year period, and included patients, irrespective of their hormone receptor or HER2 status, who were receiving neoadjuvant chemotherapy followed by surgery or surgery before adjuvant chemotherapy. All patients had primary breast cancer without evidence of distant metastatic disease and patients scheduled to receive standard neoadjuvant chemotherapy followed by surgery consented for plasma sample collection before chemotherapy, and patients scheduled to receive adjuvant chemotherapy consented for plasma sample collection after surgery and before chemotherapy. This study enrolled 170 women, and somatic mutations were identified in 101 patients, and this formed the primary analysis cohort and secondary analyses were conducted on a combined cohort of 144 patients, including 43 patients previously analyzed in a proof of principle study (N=101+43). Tumor DNA extracted from the primary tumor was sequenced to identify somatic mutations to track in plasma, and personalized tumor-specific digital Polymerase Chain Reaction (dPCR) assays were designed to monitor these somatic mutations in serial plasma samples collected from patients every 3 months during the first year of follow up, and subsequently every 6 months for 5 years. ctDNA testing can identify genetic alterations unrelated to the lesion of interest (Clonal Hematopoiesis of Indeterminate Potential- CHIP). The authors analyzed buffy coat DNA to control for CHIP, which is common with increasing age and can potentially cause false-positive results in ctDNA analysis. The mean patient age was 54 years and the median follow up was 35.5 months. The Primary objective of the study was to assess whether patients with ctDNA detected in follow-up blood samples had worse Relapse Free Survival than patients without detectable ctDNA. Secondary end points included lead time between ctDNA detection and relapse, and association between detection of ctDNA in the diagnosis sample before neoadjuvant chemotherapy and relapse.
Results from the combined cohort of 144 patients showed that detection of ctDNA during follow up was associated with relapse (88.4% of patients who experienced relapse had antecedent ctDNA detection- P<0.001). Detection of ctDNA at diagnosis, before any treatment, was associated with larger tumor size and higher tumor grade, and patients with Triple Negative Breast Cancer (TNBC) had the highest level of ctDNA, likely due to high proliferative rates and cell turnover. This patient group was at a higher risk to relapse. Further, ctDNA detection had a median lead time of 10.7 months before clinical relapse and was associated with relapse in all breast cancer subtypes. Distant extracranial metastatic relapse was detected by ctDNA in 96% of patients. Brain-only metastasis however was less commonly detected by ctDNA, suggesting that cranial metastases are less readily detectable by ctDNA analysis.
It was concluded that detection of ctDNA during follow up of early-stage breast cancer is associated with a high risk of future relapse. A clinical trial is underway evaluating the benefit of treatment initiation at molecular relapse, before clinical development of metastatic disease. Assessment of Molecular Relapse Detection in Early-Stage Breast Cancer. Garcia-Murillas I, Chopra N, Comino-Méndez I, et al. JAMA Oncol.2019;5:1473-1478.
Bottom Ad

Advertisement