
Approximately 35-40% of ovarian cancer patients express high levels of Folate Receptor alpha, and this expression correlates with advanced stages of disease and more malignant phenotypes. There is limited expression of Folate Receptor alpha in normal tissues and is limited to the choroid plexus, proximal renal tubules, placenta, and endometrium. Testing for Folate Receptor alpha can be performed on fresh or archived tissue and is considered positive if at least 75% of cells had 2+ staining intensity or greater, based on immunohistochemistry-based scoring. .
Tag: Ovarian Cancer
ELAHERE® (Mirvetuximab soravtansine-gynx)
The FDA on November 14, 2022, granted accelerated approval to ELAHERE® (Mirvetuximab soravtansine-gynx) for adult patients with Folate Receptor alpha (FRα) positive, platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer, who have received one to three prior systemic treatment regimens. ELAHERE® is a Folate Receptor alpha directed antibody and microtubule inhibitor conjugate. Patients are selected for therapy based on an FDA-approved test. ELAHERE® is a product of ImmunoGen, Inc.
FDA Approves Biomarker-Driven ELAHERE® for Platinum-Resistant Ovarian Cancer
SUMMARY: The FDA on November 14, 2022, granted accelerated approval to ELAHERE® (mirvetuximab soravtansine-gynx) for adult patients with Folate Receptor alpha (FR alpha) positive, platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer, who have received one to three prior systemic treatment regimens. The FDA also on the same day approved the VENTANA FOLR1 (FOLR-2.1) RxDx Assay (Ventana Medical Systems, Inc.), as a companion diagnostic device to select patients for the above indication.
It is estimated that in the United States, approximately 19,880 women will be diagnosed with ovarian cancer in 2022, and 12,810 women will die of the disease. Ovarian cancer ranks fifth in cancer deaths among women, and accounts for more deaths than any other cancer of the female reproductive system. Approximately 75% of the ovarian cancer patients are diagnosed with advanced disease. Approximately 85% of all ovarian cancers are epithelial in origin, and approximately 70% of all epithelial ovarian cancers are High-Grade Serous adenocarcinomas. Patients with newly diagnosed advanced ovarian cancer are often treated with platinum-based chemotherapy following primary surgical cytoreduction. Approximately 70% of these patients will relapse within the subsequent 3 years and are incurable, with a 5-year Overall Survival rate of about 20-30%. Treatment options for patients with platinum-resistant ovarian cancer are limited, and patients are often treated with single-agent chemotherapy, with an Overall Response Rate of between 4% and 13%, short duration of response, and significant toxicities.
Approximately 35-40% of ovarian cancer patients express high levels of Folate Receptor alpha, and this expression correlates with advanced stages of disease and more malignant phenotypes. There is limited expression of Folate Receptor alpha in normal tissues and is limited to the choroid plexus, proximal renal tubules, placenta, and endometrium. Testing for Folate Receptor alpha can be performed on fresh or archived tissue.
ELAHERE® (mirvetuximab soravtansine-gynx) is a first-in-class Antibody Drug Conjugate (ADC), directed against FR alpha, a cell-surface protein highly expressed in ovarian cancer. It is comprised of a Folate Receptor alpha-binding antibody, cleavable linker, and the maytansinoid payload DM4, which is a potent tubulin inhibitor, disrupting microtubule formation, and thereby designed to kill the targeted cancer cells. Microtubules are major components of the cytoskeleton that give shape and structure to cells. ELAHERE® is the first FDA approved ADC for platinum-resistant disease.
The FDA approval was based on the pivotal SORAYA trial, which is a single-arm study in 106 patients with platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer, whose tumors expressed high levels of Folate Receptor alpha, and who had been treated with 1-3 prior lines of systemic treatment regimens. All patients were required to have received prior treatment with AVASTIN® (Bevacizumab). Enrolled patient’s tumors were positive for FR alpha expression as determined by the above-mentioned FDA approved assay. Patients were eligible for the study if at least 75% of cells had 2+ staining intensity or greater, based on immunohistochemistry-based scoring. Patients were excluded if they had corneal disorders, ocular conditions requiring ongoing treatment, more than Grade 1 peripheral neuropathy, or noninfectious interstitial lung disease. Patients received ELAHERE® 6 mg/kg (based on adjusted ideal body weight) IV infusion every three weeks, until disease progression or unacceptable toxicity. Assessments were made for tumor response every six weeks for the first 36 weeks, and every 12 weeks thereafter. The Primary endpoint was investigator-assessed Overall Response Rate (ORR), and key Secondary endpoint was Duration of Response (DOR).
The confirmed ORR was 31.7% including five Complete Responses, and the median Duration of Response was 6.9 months. Response rates were consistently seen regardless of the number of prior therapies or the use of a prior PARP inhibitor. The most common adverse reactions including laboratory abnormalities, were vision impairment, keratopathy, fatigue, nausea, peripheral neuropathy, increase in ALT and AST and cytopenias. Product labeling includes a boxed warning for ocular toxicity. The authors reported that the ocular events were reversible and primarily included low-grade blurred vision and keratopathy, which were managed with protocol-defined dose modifications. Approximately 60% of patients with symptoms had resolution prior to their next cycle of treatment, and less than 1% of patients discontinued therapy due to an ocular event.
It was concluded that ELAHERE® had impressive anti-tumor activity, durability of response, and overall tolerability, and may be a new therapeutic option for patients with Folate Receptor alpha-positive platinum-resistant ovarian cancer.
Efficacy and safety of mirvetuximab soravtansine in patients with platinum-resistant ovarian cancer with high folate receptor alpha expression: Results from the SORAYA study. Matulonis UA, Lorusso D, Oaknin A, et al: 2022 SGO Annual Meeting on Women’s Cancer. Abstract 242. Presented March 19, 2022.
Late Breaking Abstract – ASCO 2022: RUBRACA® Monotherapy as Maintenance Treatment in Newly Diagnosed Ovarian Cancer
SUMMARY: It is estimated that in the United States, approximately 19,880 women will be diagnosed with ovarian cancer in 2022 and 12,810 women will die of the disease. Ovarian cancer ranks fifth in cancer deaths among women, and accounts for more deaths than any other cancer of the female reproductive system. Approximately 75% of the ovarian cancer patients are diagnosed with advanced disease. Approximately 85% of all ovarian cancers are epithelial in origin, and approximately 70% of all epithelial ovarian cancers are High-Grade Serous adenocarcinomas. Patients with newly diagnosed advanced ovarian cancer are often treated with platinum based chemotherapy following primary surgical cytoreduction. Approximately 70% of these patients will relapse within the subsequent 3 years and are incurable, with a 5 year Overall Survival rate of about 20-30%.
DNA damage is a common occurrence in daily life by UV light, ionizing radiation, replication errors, chemical agents, etc. This can result in single and double strand breaks in the DNA structure which must be repaired for cell survival. The two vital pathways for DNA repair in a normal cell are BRCA1/BRCA2 and PARP. BRCA1 and BRCA2 are tumor suppressor genes and they recognize and repair double strand DNA breaks via Homologous Recombination (HR) pathway. Homologous Recombination is a DNA repair pathway utilized by cells to accurately repair DNA double-stranded breaks during the S and G2 phases of the cell cycle, and thereby maintain genomic integrity.
Homologous Recombination Deficiency (HRD) is noted following mutation of genes involved in HR repair pathway. At least 15 genes are involved in the Homologous Recombination Repair (HRR) pathway including BRCA1 and BRCA2 genes. Mutations in BRCA1 and BRCA2 account for about 20-25% of hereditary breast cancers 15% of ovarian cancers, in addition to other cancers such as colon and prostate. BRCA mutations can either be inherited (Germline) and present in all individual cells or can be acquired and occur exclusively in the tumor cells (Somatic).
The PARP (Poly ADP Ribose Polymerase) family of enzymes includes PARP1 and PARP2, and is a related enzymatic pathway that repairs single strand breaks in DNA. In a BRCA mutant, the cancer cell relies solely on PARP pathway for DNA repair to survive. PARP inhibitors traps PARP onto DNA at sites of single-strand breaks, thereby preventing their repair and generate double-strand breaks. These breaks cannot be repaired accurately in tumors harboring defects in Homologous Recombination Repair pathway genes, such as BRCA1 or BRCA2 mutations, and this leads to cumulative DNA damage and tumor cell death.
RUBRACA® is an oral, small molecule PARP inhibitor, developed for treatment of ovarian cancer associated with Homologous Recombination DNA repair deficiency (HRD). With regards to ovarian cancer, RUBRACA® is presently approved by the FDA for the maintenance treatment of patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer, who are in a Complete or Partial Response to platinum-based chemotherapy.
ATHENA is an international, multicenter, randomized, double-blind, placebo-controlled, Phase III trial, which evaluated first-line maintenance treatment for patients with newly diagnosed advanced ovarian cancer. ATHENA was designed to evaluate RUBRACA® first-line maintenance treatment in a broad group of patients, including those without BRCA1 or BRCA2 (BRCA) mutations or other evidence of Homologous Recombination Deficiency (HRD), or high-risk clinical characteristics such as residual disease. ATHENA study has two separate and fully independently powered comparisons evaluating RUBRACA® monotherapy (ATHENA–MONO) and RUBRACA® plus Nivolumab (ATHENA–COMBO), as maintenance treatment in this patient population. The authors herein reported the efficacy and safety results from the ATHENA–MONO comparison of RUBRACA® maintenance treatment versus placebo.
In the ATHENA-MONO trial, patients with Stage III-IV high-grade ovarian cancer undergoing surgical cytoreduction (R0/complete resection permitted) and responding to 4-8 cycles of first-line platinum-doublet chemotherapy, were randomly assigned 4:1 to receive RUBRACA® 600 mg orally twice daily (N=427) or placebo. Treatment was continued for 24 months or until disease progression or unacceptable toxicity. Patients were stratified by HRD test status, residual disease after chemotherapy, and timing of surgery (primary surgery versus interval debulking). The median age was 61 years, majority of the patients (78%) did not have a BRCA mutation. Patients were stratified by HRD classification (BRCA wild-type/LOH (Loss of Heterozygosity) high-16% or more, BRCA wild-type/LOH low-less than 16%, and BRCA wild-type/LOH indeterminate). The Primary end point of investigator-assessed Progression Free Survival (PFS) was assessed in a step-down procedure, first in the HRD population (BRCA-mutant or BRCA wild-type/LOH high tumor), and then in the Intent-To-Treat (ITT) population. Secondary end points included Overall Survival (OS), investigator-assessed Objective Response Rate (ORR) in patients with measurable disease at baseline and Duration of Response (DOR) for patients with investigator-assessed confirmed radiographic Complete Response (CR) or Partial Response (PR). The median duration of follow was 26 months.
The median PFS in the HRD population was 28.7 months with RUBRACA® maintenance group compared to 11.3 months with placebo (HR=0.47; P=0.0004). In the Intent to Treat (ITT) population, the median PFS was 20.2 months in the RUBRACA® group versus 9.2 months in the placebo group (HR=0.52; P<0.0001). At 24 months, 45% of RUBRACA®-treated patients in the ITT population were progression-free compared with 25.4% with placebo. In the HRD negative population, the median PFS was 12.1 months in the RUBRACA® group versus 9.1 months in the placebo group (HR=0.65). Exploratory subgroup analyses of PFS in the ITT population showed that there was greater clinical benefit with RUBRACA® compared to placebo among all subgroups, including BRCA-mutant, BRCA wild-type/LOH high, and BRCA wild-type/LOH low (HRD-negative).
Among RUBRACA®-treated patients with measurable disease at baseline, the ORR, was 58.8% in the HRD population and 48.8% in the ITT population. Among the placebo-treated patients, the ORR was 20% in the HRD population and 9.1% in the ITT population. The median Duration of Response in the HRD and ITT populations for RUBRACA®-treated responders versus the placebo-treated responders respectively, was 16.7 months versus 5.5 months and 22.1 months versus 5.5 months. The Overall Survival results were immature at the time of the data cutoff. The most common Grade 3 or more adverse events in the RUBRACA® group were anemia (29%) and neutropenia 15%).
The authors concluded that in the ATHENA-MONO trial, RUBRACA® monotherapy is an effective first-line maintenance option that provides clinical benefit to a broad population of patients with newly diagnosed ovarian cancer, regardless of BRCA mutation and HRD status.
A Randomized, Phase III Trial to Evaluate Rucaparib Monotherapy as Maintenance Treatment in Patients With Newly Diagnosed Ovarian Cancer (ATHENA–MONO/GOG-3020/ENGOT-ov45). Monk BJ, Parkinson C, Lim MC, et al. DOI: 10.1200/JCO.2022.40.17_suppl.LBA5500 Journal of Clinical Oncology 40, no. 17_suppl (June 10, 2022) LBA5500-LBA5500. Published online June 08, 2022.
CYTALUX® (Pafolacianine)
The FDA on November 29, 2021, approved CYTALUX®, an optical imaging agent, for adult patients with ovarian cancer as an adjunct for interoperative identification of malignant lesions. CYTALUX® is a fluorescent drug that targets folate receptor which may be overexpressed in ovarian cancer. It is used with a Near-Infrared (NIR) fluorescence imaging system cleared by the FDA for specific use with CYTALUX®. CYTALUX® is a product of On Target Laboratories, LLC.
Early-Stage Multi-Cancer Detection Using an Extracellular Vesicle Protein-Based Blood Test
SUMMARY: The American Cancer Society’s estimates that in 2022, about 62,210 people will be diagnosed with pancreatic cancer and 49,830 people will die of the disease, 19,880 women will receive a new diagnosis of ovarian cancer and about 12,810 women will die of the disease, and about 81,800 new cases of bladder cancer will be diagnosed in 2022 and about 17,100 patients will die of the disease. These three cancer types are estimated to account for approximately 80,000 deaths in the US in 2022. Detecting cancer at early stages can significantly increase survival rates and outcomes.
Several multi-cancer early detection tests are being developed that involve blood-based circulating cell-free tumor DNA (cfDNA) in the plasma, to track hundreds of patient-specific mutations, to detect Minimal Residual Disease (MRD) , as well as detection of abnormal methylation patterns, followed by machine learning approaches, to differentiate between cancer and non-cancer, for detecting clinically significant, late-stage (III and IV) cancers. Early detection of cancer however is the key to improving survival. This is particularly relevant for certain cancer types. Pancreatic Ductal AdenoCarcinoma (PDAC) is one of the deadliest cancers, and a leading cause of all cancer-related deaths in the United States, and is typically detected when the disease is advanced. However, when detected at Stage I, survival rates can be as high as 80%. Ovarian cancer is often detected when the disease is advanced and the 5-year survival rates are less than 30%, but can be as high as 93% when detected early. The same holds true for metastatic bladder cancer, with 5-year survival rates of only 6%, whereas while detected when the tumor is still localized to the bladder wall inner layer results in a 5-year survival rate of 96%. Even though serum CA19-9 is intended as an aid in the management of patients with confirmed pancreatic cancer for serial monitoring of their response to therapy and disease progression, it is not recommended by the FDA for screening, as it may be elevated in several benign conditions. Similarly, serum CA-125 is FDA approved for use in monitoring patients with ovarian cancer for disease persistence and recurrence, but is not recommended to screen for ovarian cancer. Currently, there are few general screening strategies to detect asymptomatic, early-stage PDAC, ovarian, or bladder cancer and there is therefore a significant unmet need in this patient group.
Exosomes are 30-150 nm-sized Extracellular Vesicles (EVs) secreted by multiple different cell types and ejected by tumors into the bloodstream. They mediate intercellular signaling by transferring mRNAs and microRNAs between distant cells and tissues and therefore carry functional protein biomarkers representing the tumor proteome. Exosomes represent one potential approach for more sensitive detection of cancer-related biomarkers from blood.
The researchers in this study used an Alternating Current Electrokinetic (ACE)-based platform (Verita™ System) to efficiently isolate EVs from soluble contaminants such as cells, small proteins, or other vesicles from patient samples, and then measured the concentrations of associated protein biomarkers (“EV proteins”) present in the purified EV samples from our case-control study subjects. The researchers chose this platform over the current gold standard ultracentrifugation method, which the authors felt was inefficient and not suitable for point-of-care applications. Artificial Intelligence machine-learning algorithm developed by the researchers, enabled detection of early-stage pancreatic, ovarian, and bladder cancers.
In this case-control pilot study, 139 pathologically confirmed Stage I and II cancer cases representing pancreatic, ovarian, or bladder patients were compared with 184 control subjects, using the Verita™ System. The Extracellular Vesicles (EVs) isolated using this technology, were consistent with the presence of Exosomes, in accordance with the International Society for Extracellular Vesicles (ISEV) 2018 guidelines. The researchers selected a panel of 13 Extracellular Vesicle (EV) proteins along with age, a known cofactor in cancer. In order to simulate a real-world screening scenario, all cancer cases were treatment-naïve and to ensure that these were early-stage patients, the histopathologic staging was confirmed using the American Joint Commission on Cancer (AJCC) guidelines. The median age of the cancer cases was 60 years and 63.3% of the overall cancer cases were Stage I, with the remaining 36.7% at Stage II. The median age of the control group was 57 years and had no known history of cancer, autoimmune diseases, neurodegenerative disorders or diabetes mellitus.
When the overall cancer case cohort was compared with the control individuals using the EV protein biomarker test, the average sensitivity was 71.2%, at a specificity of 99.5%. When considered across all the three cancers studied, EV protein biomarker test using this technology demonstrated similar sensitivities of 70.5% and 72.5% for Stage I and II patients, respectively. This new technology detected 95.5% of Stage I pancreatic cancers, 73.1% of pathologic Stage IA lethally aggressive serous ovarian adenocarcinomas and 43.8% in bladder cancer, demonstrating the potential value of this platform for detection of early stage cancers. The lower sensitivity for detecting early stage bladder cancer may be due to high molecular and histologic heterogeneity of bladder tumors.
It was concluded from this study that blood-based EV protein detection test has potential clinical value for early cancer detection and the use of Verita™ platform resulted in the accurate detection of early stage pancreatic, ovarian, or bladder cancer. The authors added that mortality from pancreatic cancer which will soon become the second leading cause of cancer mortality in the U.S., can be greatly reduced if this study results are validated.
Early-stage multi-cancer detection using an extracellular vesicle protein-based blood test. Hinestrosa, J.P., Kurzrock, R., Lewis, J.M. et al. Commun Med 2, 29 (2022). https://doi.org/10.1038/s43856-022-00088-6.
Cytoreductive Surgery for Relapsed Ovarian Cancer Improves Overall Survival
SUMMARY: It is estimated that in the United States, approximately 19,880 women will be diagnosed with ovarian cancer in 2022 and 12,810 women will die of the disease. Ovarian cancer ranks fifth in cancer deaths among women, and accounts for more deaths than any other cancer of the female reproductive system. Approximately 75% of the ovarian cancer patients are diagnosed with advanced disease. Approximately 85% of all ovarian cancers are epithelial in origin, and approximately 70% of all epithelial ovarian cancers are High-Grade Serous adenocarcinomas. Patients with advanced ovarian cancer often receive primary cytoreductive surgery with the goal of resecting all macroscopic tumor, followed by chemotherapy with carboplatin and paclitaxel combination chemotherapy with or without Bevacizumab or a PARP inhibitor. This intervention has been associated with superior Progression Free Survival. However, approximately 70% of these patients will relapse within the subsequent 3 years and are incurable. Following a relapse, patients are treated with systemic therapy, and very few trials have shown evidence of a significant Overall Survival benefit in this setting. The role of a second cytoreductive surgery in relapsed ovarian cancer has not been well defined.
The researchers therefore conducted a prospectively randomized Phase III trial (DESKTOP III), that evaluated secondary cytoreductive surgery in platinum-sensitive, recurrent ovarian cancer. This study was designed based on previously published studies, showing the beneficial role of complete resection at first relapse, which superseded the effect of cytoreduction in upfront surgery, as well as the confirmed value of the AGO (ArbeitsgemeinschaftGynäkologischeOnkologie) score in predicting complete resectability of a tumor. A total of 407 patients with recurrent ovarian cancer, who had a first relapse after a platinum-free interval of 6 months or more, were randomly assigned 1:1 to secondary cytoreductive surgery and chemotherapy with a platinum-based regimen (N=206) or platinum-based chemotherapy alone (N=201). Eligible patients had relapsed histologically confirmed epithelial ovarian cancer (clinically defined as a lesion that is palpable or visible or that is visible on ultrasonographic imaging) or relapsed disease radiologically diagnosed at least 6 months after the last course of initial platinum-based chemotherapy (platinum-sensitive disease) and had a positive AGO score. A positive AGO score was defined as an ECOG Performance Status of 0, ascites of less than 500 ml, and complete resection at initial surgery, and this score was used to identify patients in whom a complete resection might be achieved. An elevated Cancer Antigen 125 level alone was not deemed to be an acceptable entry criterion. A complete macroscopic resection was achieved in 75.5% of the patients in the surgery group who underwent the procedure. The median duration of surgery was 3.7 hours, the median estimated blood loss was 250 ml, and was associated with low incidence of adverse events related to surgery. The Primary end point was Overall Survival (OS) and additionally Quality of Life and prognostic factors for survival were also assessed.
With a median follow up of 70 months, the median Overall Survival was significantly longer at 53.7 months in the surgery group and 46.0 months in the no-surgery group (HR for death= 0.75; P=0.02). Patients with a complete resection had the most favorable outcome, with a median Overall Survival of 61.9 months among patients in the surgery group who had complete resection, as compared with 27.7 months among patients who did not have complete resection. The median Progression Free Survival was also longer at 18.4 months in the surgery group and 14.0 months in the no-surgery group (HR for progression or death=0.66). A benefit from surgery was seen in all prognostic subgroups analyzed including age, Stage at initial diagnosis, histologic subtype, treatment history that included previous maintenance therapy, and platinum-free interval (6-12 months or more than 12 months). Quality of life measures were similar between the treatment groups at 6 months and 12 months and there was no perioperative mortality within 30 days after surgery. These findings underscore the importance of surgical skill needed to successfully perform secondary cytoreductive surgery, with resulting complete macroscopic resection.
It was concluded that in women with platinum-sensitive recurrent ovarian cancer, cytoreductive surgery performed before second line chemotherapy resulted in longer Overall Survival and Progression Free Survival, as compared to chemotherapy alone, without negatively impacting Quality of Life.
Randomized Trial of Cytoreductive Surgery for Relapsed Ovarian Cancer. Harter P, Sehouli J, Vergote I, et al., for the DESKTOP III Investigators. N Engl J Med 2021;385:2123-2131.
ASCO Guideline: PARP Inhibitors in the Management of Ovarian Cancer
SUMMARY: It is estimated that in the United States, approximately 21,750 women will be diagnosed with ovarian cancer in 2020 and 13,940 women will die of the disease. Ovarian cancer ranks fifth in cancer deaths among women, and accounts for more deaths than any other cancer of the female reproductive system. Approximately 75% of the ovarian cancer patients are diagnosed with advanced disease. Approximately 85% of all ovarian cancers are epithelial in origin, and approximately 70% of all epithelial ovarian cancers are High-Grade Serous adenocarcinomas. Patients with newly diagnosed advanced ovarian cancer are often treated with platinum based chemotherapy following primary surgical cytoreduction. Approximately 70% of these patients will relapse within the subsequent 3 years and are incurable, with a 5 year Overall Survival rate of about 20-30%.
Germline mutations in BRCA1 and BRCA2 genes account for about 17% of ovarian cancers (mutations present in all individual cells), whereas somatic mutations are found in an additional 7% (mutations present exclusively in tumor cells). BRCA1 and BRCA2 are tumor suppressor genes and they recognize and repair double strand DNA breaks via Homologous Recombination (HR) pathway. Homologous Recombination is a DNA repair pathway utilized by cells to accurately repair DNA double-stranded breaks during the S and G2 phases of the cell cycle, and thereby maintain genomic integrity. The PARP (Poly ADP Ribose Polymerase) family of enzymes include PARP1 and PARP2, and is a related enzymatic pathway that repairs single strand breaks in DNA. In a BRCA mutant, the cancer cell relies solely on PARP pathway for DNA repair to survive. PARP inhibitors traps PARP onto DNA at sites of single-strand breaks, thereby preventing their repair and generate double-strand breaks. These breaks cannot be repaired accurately in tumors harboring defects in Homologous Recombination Repair pathway genes, such as BRCA1 or BRCA2 mutations, and this leads to cumulative DNA damage and tumor cell death.
This systematic review-based guideline was developed by a multidisciplinary ASCO Expert Panel to provide clinicians and other health care practitioners, recommendations on the use of PARP inhibitors for management of Epithelial Ovarian, tubal, or Primary Peritoneal Cancer (herein referred to as EOC), based on best available evidence. The recommendations were developed following a systematic review of the literature which identified 17 randomized controlled trials published from 2011 through 2020, that included patients who have not previously received a PARP inhibitor.
ASCO Guideline Questions:
1) Should PARP inhibitor therapy for EOC be repeated over the course of treatment?
2) In which patients with newly diagnosed EOC are PARP inhibitors recommended?
a. What are the histologic types of EOC for which PARP inhibitors are recommended?
b. What are the biomarker subsets for which PARP inhibitors are recommended?
3) Is PARP inhibitor monotherapy recommended for recurrent EOC? If so,
a. In which settings (eg, second-line maintenance or treatment of recurrent disease)?
b. At what dose and duration?
4) Are there settings where PARP inhibitors in combination with chemotherapy or other targeted therapy are recommended?
5) How should clinicians manage the specific toxicities of the various PARP inhibitors?
Recommendations: The following recommendations pertain only to patients with EOC who have not previously received a PARP inhibitor.
Repeating PARP Inhibitor
Recommendation 1.0: Repeating therapy with a PARP inhibitor in the treatment of EOC is not recommended at this time. Consideration should be made as to the best time in the life cycle of an individual patient’s EOC in which to use PARP inhibitor. Clinical trial participation is encouraged.
Newly Diagnosed Ovarian Cancer
Recommendation 2.0: PARP inhibitors are not recommended for use in initial treatment of early stage (Stage I-II) EOC because there is insufficient evidence to support use in this population.
Recommendation 2.1: Women with newly diagnosed Stage III-IV EOC that is in Complete or Partial Response to first-line platinum-based chemotherapy should be offered PARP inhibitor maintenance therapy with Olaparib (for those with germline or somatic pathogenic or likely pathogenic variants in BRCA1 or BRCA2 genes) or Niraparib (all women) in High-Grade Serous or endometrioid ovarian cancer.
PARP inhibitor maintenance therapy should consist of Olaparib (300 mg orally every 12 hours for 2 years) or Niraparib (200-300 mg orally daily for 3 years). Longer duration could be considered in selected individuals.
Recommendation 2.2: The addition of Olaparib to Bevacizumab maintenance may be offered to patients who have Stage III-IV High-Grade Serous or endometrioid ovarian cancer and germline or somatic pathogenic or likely pathogenic variants in BRCA1 or BRCA2 genes and/or genomic instability, as determined by Myriad myChoice CDx, and who have had a Partial or Complete Response to chemotherapy plus Bevacizumab combination.
Recommendation 2.3: Inclusion of the PARP inhibitor Veliparib with combination chemotherapy followed by Veliparib maintenance therapy cannot be recommended at this time. There are no data that this approach is superior, equal, or less toxic than a switch maintenance.
Note: Veliparib is not commercially available at the time of these recommendations.
Recurrent Ovarian Cancer: Second-Line or Greater Maintenance and Treatment
Recommendation 3.0: PARP inhibitor monotherapy maintenance (second-line or more) may be offered to patients with EOC who have not already received a PARP inhibitor and who have responded to platinum-based therapy regardless of BRCA mutation status. Treatment is continued until disease progression or toxicity despite dose reductions and best supportive care. Options include Olaparib 300 mg every 12 hours, Rucaparib 600 mg every 12 hours or Niraparib 200-300 mg once daily.
Recommendation 3.1: Treatment with a PARP inhibitor should be offered to patients with recurrent EOC who have not already received a PARP inhibitor and have a germline or somatic pathogenic or likely pathogenic variants in BRCA1 or BRCA2 genes. Options include Olaparib 300 mg every 12 hours, Rucaparib 600 mg every 12 hours or Niraparib 200-300 mg once daily.
Recommendation 3.2: Treatment with a PARP inhibitor monotherapy should be offered to patients with recurrent EOC who have not already received a PARP inhibitor, and whose tumor demonstrates genomic instability, as determined by Myriad myChoice CDx, and has not recurred within 6 months of platinum-based therapy
Recommendation 3.3: PARP inhibitors are not recommended for treatment of BRCA wild-type or platinum-resistant recurrent EOC
PARP Inhibitors in Combination
Recommendation 4.0: PARP inhibitors are not recommended for use in combination with chemotherapy, other targeted agents, or immune-oncology agents in the recurrent setting outside the context of a clinical trial. Clinical trial participation is encouraged.
Management of Adverse Events
Recommendation 5.0 Anemia: Patients requiring a blood transfusion for symptom relief and/or hemoglobin level less than 8 g/dL should be monitored. PARP inhibitor dose should be reduced with evidence of repeated anemia to avoid multiple transfusions. Patients with progressive anemia may be offered growth factor per ASCO guidelines and physician and patient comfort.
Recommendation 5.1 Neutropenia: Growth factor is not indicated for use in patients receiving daily PARP inhibitor. Neutropenia (grade 4 lasting at least 5-7 days or associated with fever) should result in dose hold until recovery of infection and granulocyte count, followed by dose reduction. Growth factor support may be used in this setting to support patient safety during the drug hold period.
Recommendation 5.2 Platelets: Thrombocytopenia is most common with Niraparib. Niraparib dosing guidelines should be used to lower starting dose (200 mg) based on weight and platelet count. Discontinue PARP inhibitor for persistent thrombocytopenia or significant bleeding despite dose reduction.
Recommendation 5.3 Persistent cytopenia: Evaluation for treatment-related Myelodysplastic Syndrome/Acute Myeloid Leukemia should be initiated in patients with persistent cytopenia that occurs despite drug hold.
Recommendation 5.4 Nausea: Many patients will have tachyphylaxis of nausea symptoms over the first cycle of therapy. Persistent nausea requiring daily antiemetic intervention, causing a reduction in performance status, and/or resulting in more than 5% weight loss, should result in dose reduction.
PARP Inhibitors in the Management of Ovarian Cancer: ASCO Guideline. Tew WP, Lacchetti C, Ellis A, et al. J Clin Oncol 2020;38:3468-3493.
ASCO Guideline: PARP Inhibitors in the Management of Ovarian Cancer
SUMMARY: It is estimated that in the United States, approximately 21,750 women will be diagnosed with ovarian cancer in 2020 and 13,940 women will die of the disease. Ovarian cancer ranks fifth in cancer deaths among women, and accounts for more deaths than any other cancer of the female reproductive system. Approximately 75% of the ovarian cancer patients are diagnosed with advanced disease. Approximately 85% of all ovarian cancers are epithelial in origin, and approximately 70% of all epithelial ovarian cancers are High-Grade Serous adenocarcinomas. Patients with newly diagnosed advanced ovarian cancer are often treated with platinum based chemotherapy following primary surgical cytoreduction. Approximately 70% of these patients will relapse within the subsequent 3 years and are incurable, with a 5 year Overall Survival rate of about 20-30%.
Germline mutations in BRCA1 and BRCA2 genes account for about 17% of ovarian cancers (mutations present in all individual cells), whereas somatic mutations are found in an additional 7% (mutations present exclusively in tumor cells). BRCA1 and BRCA2 are tumor suppressor genes and they recognize and repair double strand DNA breaks via Homologous Recombination (HR) pathway. Homologous Recombination is a DNA repair pathway utilized by cells to accurately repair DNA double-stranded breaks during the S and G2 phases of the cell cycle, and thereby maintain genomic integrity. The PARP (Poly ADP Ribose Polymerase) family of enzymes include PARP1 and PARP2, and is a related enzymatic pathway that repairs single strand breaks in DNA. In a BRCA mutant, the cancer cell relies solely on PARP pathway for DNA repair to survive. PARP inhibitors traps PARP onto DNA at sites of single-strand breaks, thereby preventing their repair and generate double-strand breaks. These breaks cannot be repaired accurately in tumors harboring defects in Homologous Recombination Repair pathway genes, such as BRCA1 or BRCA2 mutations, and this leads to cumulative DNA damage and tumor cell death.
This systematic review-based guideline was developed by a multidisciplinary ASCO Expert Panel to provide clinicians and other health care practitioners, recommendations on the use of PARP inhibitors for management of Epithelial Ovarian, tubal, or Primary Peritoneal Cancer (herein referred to as EOC), based on best available evidence. The recommendations were developed following a systematic review of the literature which identified 17 randomized controlled trials published from 2011 through 2020, that included patients who have not previously received a PARP inhibitor.
ASCO Guideline Questions:
1) Should PARP inhibitor therapy for EOC be repeated over the course of treatment?
2) In which patients with newly diagnosed EOC are PARP inhibitors recommended?
a. What are the histologic types of EOC for which PARP inhibitors are recommended?
b. What are the biomarker subsets for which PARP inhibitors are recommended?
3) Is PARP inhibitor monotherapy recommended for recurrent EOC? If so,
a. In which settings (eg, second-line maintenance or treatment of recurrent disease)?
b. At what dose and duration?
4) Are there settings where PARP inhibitors in combination with chemotherapy or other targeted therapy are recommended?
5) How should clinicians manage the specific toxicities of the various PARP inhibitors?
Recommendations: The following recommendations pertain only to patients with EOC who have not previously received a PARP inhibitor.
Repeating PARP Inhibitor
Recommendation 1.0: Repeating therapy with a PARP inhibitor in the treatment of EOC is not recommended at this time. Consideration should be made as to the best time in the life cycle of an individual patient’s EOC in which to use PARP inhibitor. Clinical trial participation is encouraged.
Newly Diagnosed Ovarian Cancer
Recommendation 2.0: PARP inhibitors are not recommended for use in initial treatment of early stage (Stage I-II) EOC because there is insufficient evidence to support use in this population.
Recommendation 2.1: Women with newly diagnosed Stage III-IV EOC that is in Complete or Partial Response to first-line platinum-based chemotherapy should be offered PARP inhibitor maintenance therapy with Olaparib (for those with germline or somatic pathogenic or likely pathogenic variants in BRCA1 or BRCA2 genes) or Niraparib (all women) in High-Grade Serous or endometrioid ovarian cancer.
PARP inhibitor maintenance therapy should consist of Olaparib (300 mg orally every 12 hours for 2 years) or Niraparib (200-300 mg orally daily for 3 years). Longer duration could be considered in selected individuals.
Recommendation 2.2: The addition of Olaparib to Bevacizumab maintenance may be offered to patients who have Stage III-IV High-Grade Serous or endometrioid ovarian cancer and germline or somatic pathogenic or likely pathogenic variants in BRCA1 or BRCA2 genes and/or genomic instability, as determined by Myriad myChoice CDx, and who have had a Partial or Complete Response to chemotherapy plus Bevacizumab combination.
Recommendation 2.3: Inclusion of the PARP inhibitor Veliparib with combination chemotherapy followed by Veliparib maintenance therapy cannot be recommended at this time. There are no data that this approach is superior, equal, or less toxic than a switch maintenance.
Note: Veliparib is not commercially available at the time of these recommendations.
Recurrent Ovarian Cancer: Second-Line or Greater Maintenance and Treatment
Recommendation 3.0: PARP inhibitor monotherapy maintenance (second-line or more) may be offered to patients with EOC who have not already received a PARP inhibitor and who have responded to platinum-based therapy regardless of BRCA mutation status. Treatment is continued until disease progression or toxicity despite dose reductions and best supportive care. Options include Olaparib 300 mg every 12 hours, Rucaparib 600 mg every 12 hours or Niraparib 200-300 mg once daily.
Recommendation 3.1: Treatment with a PARP inhibitor should be offered to patients with recurrent EOC who have not already received a PARP inhibitor and have a germline or somatic pathogenic or likely pathogenic variants in BRCA1 or BRCA2 genes. Options include Olaparib 300 mg every 12 hours, Rucaparib 600 mg every 12 hours or Niraparib 200-300 mg once daily.
Recommendation 3.2: Treatment with a PARP inhibitor monotherapy should be offered to patients with recurrent EOC who have not already received a PARP inhibitor, and whose tumor demonstrates genomic instability, as determined by Myriad myChoice CDx, and has not recurred within 6 months of platinum-based therapy
Recommendation 3.3: PARP inhibitors are not recommended for treatment of BRCA wild-type or platinum-resistant recurrent EOC
PARP Inhibitors in Combination
Recommendation 4.0: PARP inhibitors are not recommended for use in combination with chemotherapy, other targeted agents, or immune-oncology agents in the recurrent setting outside the context of a clinical trial. Clinical trial participation is encouraged.
Management of Adverse Events
Recommendation 5.0 Anemia: Patients requiring a blood transfusion for symptom relief and/or hemoglobin level less than 8 g/dL should be monitored. PARP inhibitor dose should be reduced with evidence of repeated anemia to avoid multiple transfusions. Patients with progressive anemia may be offered growth factor per ASCO guidelines and physician and patient comfort.
Recommendation 5.1 Neutropenia: Growth factor is not indicated for use in patients receiving daily PARP inhibitor. Neutropenia (grade 4 lasting at least 5-7 days or associated with fever) should result in dose hold until recovery of infection and granulocyte count, followed by dose reduction. Growth factor support may be used in this setting to support patient safety during the drug hold period.
Recommendation 5.2 Platelets: Thrombocytopenia is most common with Niraparib. Niraparib dosing guidelines should be used to lower starting dose (200 mg) based on weight and platelet count. Discontinue PARP inhibitor for persistent thrombocytopenia or significant bleeding despite dose reduction.
Recommendation 5.3 Persistent cytopenia: Evaluation for treatment-related Myelodysplastic Syndrome/Acute Myeloid Leukemia should be initiated in patients with persistent cytopenia that occurs despite drug hold.
Recommendation 5.4 Nausea: Many patients will have tachyphylaxis of nausea symptoms over the first cycle of therapy. Persistent nausea requiring daily antiemetic intervention, causing a reduction in performance status, and/or resulting in more than 5% weight loss, should result in dose reduction.
PARP Inhibitors in the Management of Ovarian Cancer: ASCO Guideline. Tew WP, Lacchetti C, Ellis A, et al. J Clin Oncol 2020;38:3468-3493.
LYNPARZA® Superior to Chemotherapy in BRCA Mutated Platinum Sensitive Advanced Ovarian Cancer
SUMMARY: It is estimated that in the United States, approximately 21,750 women will be diagnosed with ovarian cancer in 2020 and 13,940 women will die of the disease. Ovarian cancer ranks fifth in cancer deaths among women, and accounts for more deaths than any other cancer of the female reproductive system. Approximately 75% of the ovarian cancer patients are diagnosed with advanced disease. Patients with newly diagnosed advanced ovarian cancer are often treated with platinum based chemotherapy following primary surgical cytoreduction. Approximately 70% of these patients will relapse within the subsequent 3 years and are incurable, with a 5 year Overall Survival rate of about 20-30%.
DNA damage is a common occurrence in daily life by UV light, ionizing radiation, replication errors, chemical agents, etc. This can result in single and double strand breaks in the DNA structure which must be repaired for cell survival. The two vital pathways for DNA repair in a normal cell are BRCA1/BRCA2 and PARP. BRCA1 and BRCA2 are tumor suppressor genes and they recognize and repair double strand DNA breaks via Homologous Recombination (HR) pathway. Homologous Recombination is a DNA repair pathway utilized by cells to accurately repair DNA double-stranded breaks during the S and G2 phases of the cell cycle, and thereby maintain genomic integrity.
Homologous Recombination Deficiency (HRD) is noted following mutation of genes involved in HR repair pathway. At least 15 genes are involved in the Homologous Recombination Repair (HRR) pathway including BRCA1 and BRCA2 genes. The BRCA1 gene is located on the long (q) arm of chromosome 17 whereas BRCA2 is located on the long arm of chromosome 13, and they regulate cell growth and prevent abnormal cell division and development of malignancy. Mutations in BRCA1 and BRCA2 account for about 20-25% of hereditary breast cancers 15% of ovarian cancers, in addition to other cancers such as Colon and Prostate. BRCA mutations can either be inherited (Germline) and present in all individual cells or can be acquired and occur exclusively in the tumor cells (Somatic).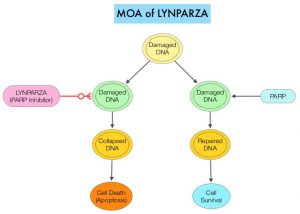
The PARP (Poly ADP Ribose Polymerase) family of enzymes include PARP1 and PARP2, and is a related enzymatic pathway that repairs single strand breaks in DNA. In a BRCA mutant, the cancer cell relies solely on PARP pathway for DNA repair to survive. LYNPARZA® is a PARP inhibitor that traps PARP onto DNA at sites of single-strand breaks, preventing their repair and generating double-strand breaks that cannot be repaired accurately in tumors harboring defects in Homologous Recombination Repair pathway genes, such as BRCA1 or BRCA2 mutations, leading to cumulative DNA damage and tumor cell death.
Previously published studies demonstrated a durable response to LYNPARZA® administered as treatment (rather than maintenance), in women with heavily pretreated relapsed ovarian cancer and a germline BRCA mutation, with an Objective Response Rate (ORR) of 42% in the subgroup of patients with platinum-sensitive disease, who had received at least 3 prior chemotherapy regimens. Single-agent nonplatinum chemotherapy is often used in heavily pretreated women with relapsed ovarian cancer. The authors conducted this study to evaluate whether LYNPARZA® monotherapy improves outcomes, compared with physician’s choice single-agent nonplatinum chemotherapy, in patients with platinum-sensitive relapsed ovarian cancer and a germline BRCA mutation, who have received at least 2 prior lines of platinum-based chemotherapy.
SOLO3 is an International, randomized, controlled, open label Phase III trial, that compared LYNPARZA® with non-platinum chemotherapy, in patients with platinum sensitive, relapsed ovarian cancer, and a germline BRCA1/2 mutation. This study included 266 patients who were randomly assigned 2:1 to LYNPARZA® 300 mg orally given twice a day (N=178) or physician’s choice of single-agent chemotherapy (N=88), which could be either Pegylated Liposomal Doxorubicin (PLD) 50 mg/m2 IV on day 1 every 4 weeks, Paclitaxel 80 mg/m2 IV on days 1, 8, 15, and 22 every 4 weeks, Gemcitabine 1000 mg/m2 IV on days 1, 8, and 15 every 4 weeks or Topotecan 4 mg/m2 IV on days 1, 8, and 15 every 4 weeks. Eligible patients had relapsed high-grade serous or high-grade endometrioid ovarian cancer, primary peritoneal cancer, and/or fallopian tube cancer, with at least 1 measurable and/or nonmeasurable lesion, that could be accurately assessed at baseline, by CT or MRI, and was suitable for repeated evaluation. Patients had received at least 2 prior lines of platinum-based chemotherapy for ovarian cancer and were platinum sensitive (progression more than 6 months after the end of the last platinum-based regimen). Treatment groups were well balanced and the median patient age was 59 years. The Primary end point was Objective Response Rate (ORR) in those with measurable disease, as assessed by Blinded Independent Central Review (BICR). The key Secondary end point was Progression Free Survival (PFS) assessed by BICR in the intent-to-treat population.
It was noted that ORR was significantly higher in the LYNPARZA® group than in the chemotherapy group (72.2% versus 51.4%; Odds Ratio=2.53; P=0.002), suggesting a 2.53 times higher likelihood of responding to LYNPARZA®, than to chemotherapy. In the subgroup who had received 2 prior lines of treatment, the ORR with LYNPARZA® was 84.6% and 61.5% with chemotherapy (Odds Ratio= 3.44), suggesting a 3.44 times higher likelihood of responding to LYNPARZA®, than to chemotherapy. The median time to onset of response was 2 months with LYNPARZA®, versus 3.5 months with chemotherapy, and the median Duration of Response was 9.4 months and 10.2 months respectively. The PFS also significantly favored LYNPARZA® versus chemotherapy (13.4 versus 9.2 months; HR=0.62; P=0.013). Adverse events were consistent with the established safety profiles of LYNPARZA® and chemotherapy. The most common Grade 3 or more adverse events were anemia in the LYNPARZA® group and PPE (Palmar-Plantar Erythrodysesthesia) and neutropenia in the chemotherapy group.
It was concluded that treatment with LYNPARZA® resulted in statistically significant and clinically relevant improvements in Objective Response Rate and Progression Free Survival, compared with nonplatinum chemotherapy, in patients with germline BRCA-mutated, platinum-sensitive, relapsed ovarian cancer, who had received at least 2 prior lines of platinum-based chemotherapy. This chemotherapy-free treatment option will be welcome news for patients with germline BRCA-mutated advanced ovarian cancer.
Olaparib Versus Nonplatinum Chemotherapy in Patients With Platinum-Sensitive Relapsed Ovarian Cancer and a Germline BRCA1/2 Mutation (SOLO3): A Randomized Phase III Trial. Penson RT, Valencia RV, Cibula D, et al. J Clin Oncol. 2020;38:1164-1174.