
SUMMARY: The FDA on September 14, 2017, granted accelerated approval to ALIQOPA® (Copanlisib) for the treatment of adult patients with relapsed Follicular Lymphoma, who have received at least two prior systemic therapies. The American Cancer Society estimates that in 2017, about 72,240 people will be diagnosed with Non Hodgkin Lymphoma (NHL) in the United States and about 20,140 individuals will die of this disease. Indolent NHLs are mature B cell lymphoproliferative disorders and include Follicular Lymphoma, Nodal Marginal Zone Lymphoma (NMZL), Extranodal Marginal Zone Lymphoma (ENMZL) of Mucosa-Associated Lymphoid Tissue (MALT), Splenic Marginal Zone Lymphoma (SMZL), LymphoPlasmacytic Lymphoma (LPL) and Small Lymphocytic Lymphoma (SLL). Follicular Lymphoma is the most indolent form and second most common form of all NHLs and they are a heterogeneous group of lymphoproliferative malignancies. Approximately 20% of all NHLs are Follicular Lymphomas. Advanced stage indolent NHL is not curable and as such, prolonging Progression Free Survival (PFS) and Overall Survival (OS), while maintaining Quality of Life, have been the goals of treatment intervention. Asymptomatic patients with indolent NHL are generally considered candidates for “watch and wait” approach whereas those with B symptoms (fever, night sweats, and weight loss), painful lymphadenopathy/splenomegaly, organ compromise and cytopenias are generally considered candidates for therapy.. Follicular Lymphoma International Prognostic Index (FLIPI) is of prognostic value and is used to help with treatment choices. The Ann Arbor classification divides FL into four stages. Patients with stages I and II have localized disease and those with stages III and IV have advanced disease. The World Health Organization (WHO) further classified FL based on histology into low grade (grades 1 and 2) and high grade (grade 3a) FLs. Grade 3b FL which demonstrates diffuse areas of involvement is designated as Diffuse Large B-cell Lymphoma (DLBCL) and is treated as such. Patients with advanced stage symptomatic Follicular Lymphoma are often treated with induction chemoimmunotherapy followed by maintenance RITUXAN® (Rituximab). This can result in a median PFS of 6-8 yrs and a median Overall Survival of 12-15 yrs. However, approximately 30% of the patients will relapse in 3 years and treatment options are limited for patients with relapses, after multiple treatments.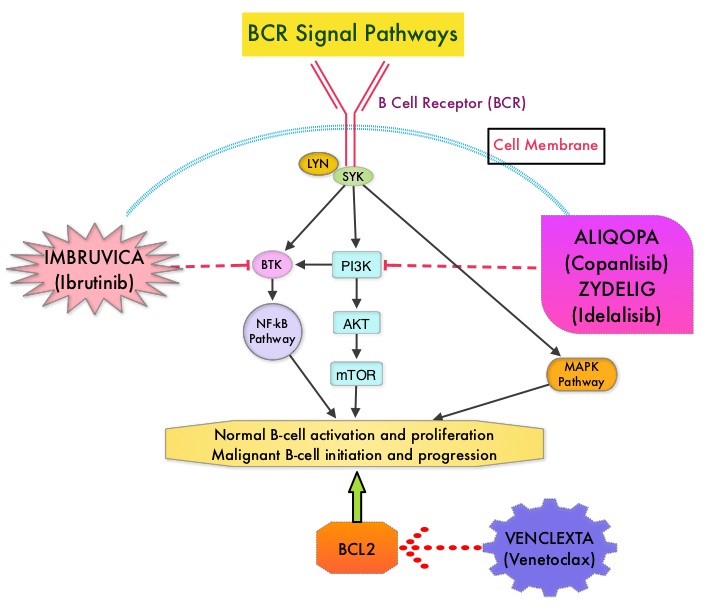
ALIQOPA® is a pan-class 1, PI3K inhibitor with inhibitory activity predominantly against PI3K-α and PI3K-δ Isoforms expressed in malignant B cells. The alpha isoform is broadly expressed and involved in insulin signaling and angiogenesis, as well as resistance mechanisms to lymphoma whereas the delta isoform is expressed by leukocytes and is involved in B-cell signaling, development, and survival. ALIQOPA® has been shown to induce tumor cell death by apoptosis and inhibition of proliferation of primary malignant B cell lines. ALIQOPA® also inhibits several key cell-signaling pathways, including B-cell receptor (BCR) signaling, CXCR12 (C-X-C chemokine receptor 12) mediated chemotaxis of malignant B cells, and NFÏ°B (Nuclear Factor Kappa B) signaling in lymphoma cell lines.
The approval of ALIQOPA® was based on data from the CHRONOS-1 trial, which is an open-label, single arm, multicenter, phase II study of patients with relapsed, Indolent or aggressive Non Hodgkin Lymphomas. This trial included patients with Follicular lymphoma (Grades 1-3a), Marginal Zone Lymphoma, Small Lymphocytic Lymphoma, and LymphoPlasmacytic Lymphoma /Waldenstrom Macroglobulinemia . Eligible patients had relapsed or refractory disease and had received at least two prior systemic therapies. The efficacy data leading to the FDA approval included 104 patients with Follicular B-cell Non Hodgkin Lymphoma. In this trial, patients received 0.8 mg/kg or 60 mg of ALIQOPA® by IV infusion on days 1, 8, and 15 of a 28-day treatment cycle, until disease progression or development of unacceptable toxicity. The median patient age was 63 yrs and all study patients had prior exposure to RITUXAN® and one or more alkylating agents, and 60% of the patients had disease that was refractory to the last regimen received. The Primary endpoint was Objective Response Rate after a minimum of 16 weeks of treatment. Secondary endpoints included Progression Free Survival, Duration of Response, Overall Survival, safety, and Quality of Life.
The Objective Response Rate was 58.7%, with an estimated median response duration of 12.2 months. The Complete Response rate was 14.4% and partial response rate was 44.3% and 33.7% has stable disease. The most common adverse reactions included nausea, hyperglycemia, diarrhea, fatigue, hypertension, cytopenias and lower respiratory tract infections. According to the authors, safety was manageable compared with the other PI3K inhibitor approved by the FDA, ZYDELIG® (Idelalisib), which targets only the δ-isoform and has warnings against fatal or severe colitis, intestinal perforation, hepatotoxicity, and pneumonitis The safety advantage with ALIQOPA® may be due to the dose scheduling or the IV mode of delivery.
It was concluded that ALIQOPA® has significant activity in patients with relapsed/refractory indolent B-cell lymphoma, and the safety was manageable, compared with other PI3K inhibitors. Two phase III trials are underway, using ALIQOPA® in combination with RITUXAN®. Dreyling M, Santoro A, Mollica L, et al. Copanlisib in patients with relapsed or refractory indolent B-cell lymphoma: Primary results of the pivotal CHRONOS-1 study. Presented at: 2017 AACR Annual Meeting; April 1-5, 2017; Washington, DC. Abstract CT149.
 Hyaluronan is a polysaccharide present in the extracellular matrix of the subcutaneous tissue and is depolymerized by the naturally occurring enzyme Hyaluronidase.
Hyaluronan is a polysaccharide present in the extracellular matrix of the subcutaneous tissue and is depolymerized by the naturally occurring enzyme Hyaluronidase. 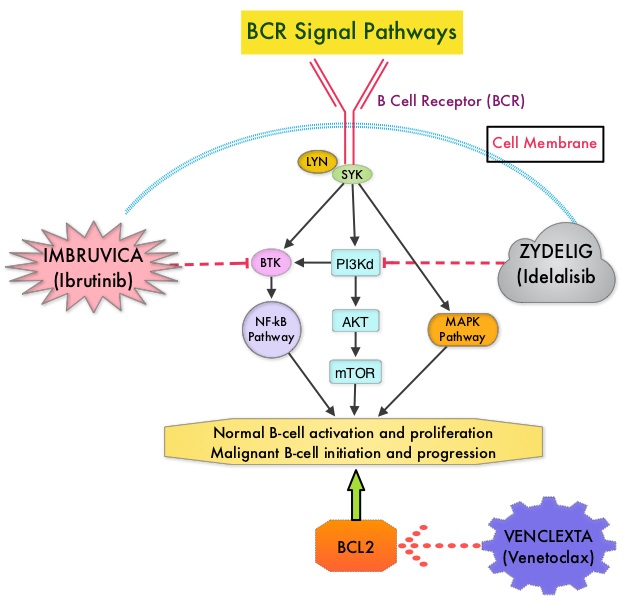

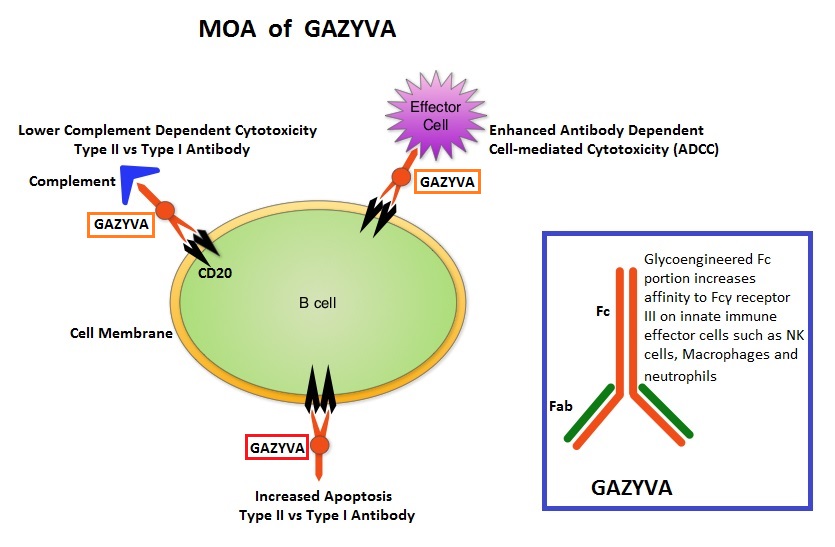

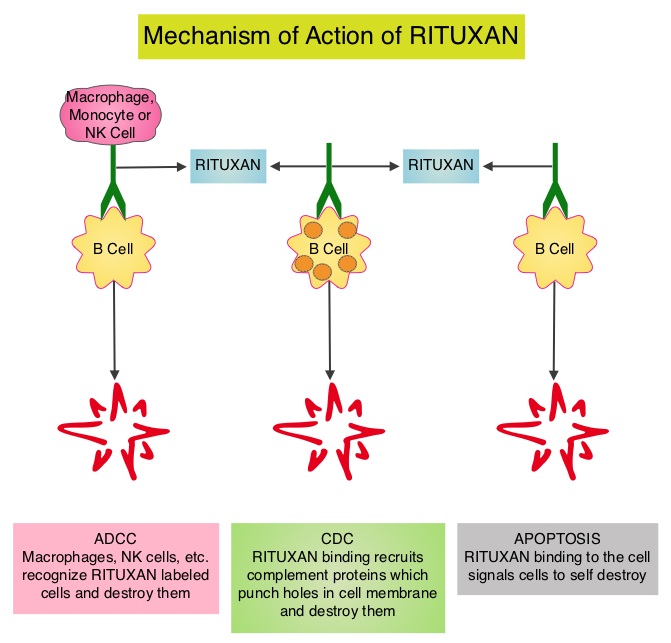
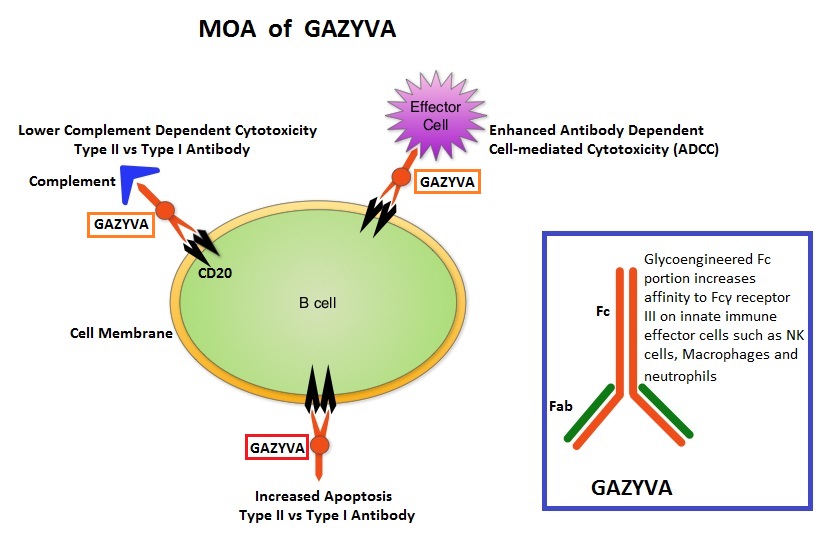 GAZYVA® (Obinutuzumab) is glycoengineered, fully humanized, third generation, type II anti-CD20 antibody (IgG1 monoclonal antibody) that selectivity binds to the extracellular domain of the CD20 antigen on malignant human B cells. By virtue of binding affinity of the glycoengineered Fc portion of GAZYVA® to Fcγ receptor III on innate immune effector cells such as natural killer cells, macrophages and neutrophils, Antibody-Dependent Cell-mediated Cytotoxicity (ADCC) and Antibody-Dependent Cellular phagocytosis is significantly enhanced, whereas it induces very little Complement-Dependent Cytotoxicity. This is in contrast to RITUXAN® (Rituximab), which is a first generation type I, chimeric anti-CD20 targeted monoclonal antibody that kills lymphoma cells primarily by Complement-Dependent Cytotoxicity and also ADCC.
GAZYVA® (Obinutuzumab) is glycoengineered, fully humanized, third generation, type II anti-CD20 antibody (IgG1 monoclonal antibody) that selectivity binds to the extracellular domain of the CD20 antigen on malignant human B cells. By virtue of binding affinity of the glycoengineered Fc portion of GAZYVA® to Fcγ receptor III on innate immune effector cells such as natural killer cells, macrophages and neutrophils, Antibody-Dependent Cell-mediated Cytotoxicity (ADCC) and Antibody-Dependent Cellular phagocytosis is significantly enhanced, whereas it induces very little Complement-Dependent Cytotoxicity. This is in contrast to RITUXAN® (Rituximab), which is a first generation type I, chimeric anti-CD20 targeted monoclonal antibody that kills lymphoma cells primarily by Complement-Dependent Cytotoxicity and also ADCC.