
The FDA on November 16, 2015 granted accelerated approval to DARZALEX®, administered as a single agent, for the treatment of patients with multiple myeloma who have received at least three prior lines of therapy, including a Proteasome Inhibitor (PI) and an immunomodulatory agent, or who are double-refractory to a PI and an immunomodulatory agent. DARZALEX® is a product of Janssen Biotech, Inc.
Tag: Multiple Myeloma
Continuous Therapy Significantly Improves Outcomes compared to Fixed Duration of Therapy in Patients with Newly Diagnosed Multiple Myeloma
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, close to 27,000 new cases will be diagnosed in 2015 and 11,240 will die of the disease. Maintenance or Continuous Treatment in patients with newly diagnosed multiple myeloma following induction and consolidation, can result in significantly longer Progression Free Survival (PFS) and Overall Survival (OS), compared to those patients who receive therapy for a fixed duration of time. Not all studies however, have shown Overall Survival benefit. It has been hypothesized that Continuous Treatment could result in resistance to therapy which in turn could reduce the duration of subsequent remission after first relapse and negatively impact overall survival.To address this controversy, the authors conducted a pooled analysis of the outcomes of three randomized phase III trials, coordinated by the same principal investigator, designed to compare Continuous Treatment to Fixed Duration Therapy, in patients with newly diagnosed multiple myeloma.
In trial RV-MM-209, patients were randomized to either induction with Lenolidomide (REVLIMID®), followed by consolidation and subsequent maintenance with REVLIMID® (Continuous Treatment) or Fixed Duration Therapy which entailed REVLIMID® based induction followed by consolidation but no maintenance therapy. In the GIMEMA0305 trial, the randomization was between Bortezomib (VELCADE®) based induction followed by maintenance treatment (Continuous Treatment) and VELCADE® induction, with no maintenance treatment (Fixed Duration Therapy). In the CC-5013-MM-015 study, the comparison was between REVLIMID® in combination with Melphalan and Prednisone followed by REVLIMID® maintenance until disease progression and placebo given along with Melphalan and Prednisone.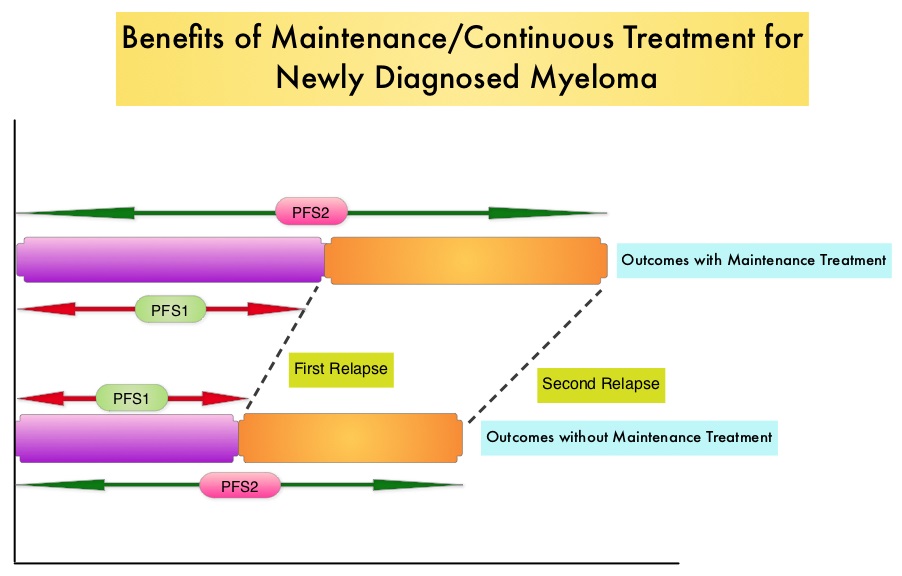
The trial investigators assessed PFS1 as the time from diagnosis to the occurrence of 1st relapse, PFS2 as time from diagnosis to the occurrence of 2nd relapse and Overall Survival as time from diagnosis to death , incorporating the duration of both 1st and 2nd remission. They then evaluated PFS1, PFS2 and OS, in newly diagnosed multiple myeloma patients who received Continuous Therapy or Fixed Duration Therapy. In this pooled analysis of three trials, 604 patients were randomized to Continuous Treatment and 614 patients were randomized to Fixed Duration Therapy. Four hundred and seventeen (N=417) in the Continuous Therapy group and 410 patients in the Fixed Duration Therapy group were eligible for comparative analysis. The median follow up was 52 months.
Patients receiving Continuous Treatment had significantly prolonged PFS1 (median 32 months versus 16 months; HR=0.47; P<0.001), PFS2 (median 55 months versus 40 months; HR=0.61; P=0.001) and OS (4 year OS 69% versus 60%; HR=0.69; P=0.003), when compared with Fixed Dose Therapy. The authors evaluated the PFS and OS from first relapse to second relapse and from first relapse to death respectively, and they noted that the outcomes were similar among patients who received Continuous Treatment or Fixed Dose Therapy following initial diagnosis.
The authors concluded that Continuous Treatment significantly improved PFS1, PFS2, and OS and findings from this pooled analysis suggested that the clinical benefit observed during first remission was not negated by a shorter second remission and Continuous Treatment did not induce tumor resistance. Continuous Treatment may be essential, as patients with multiple myeloma will always have some residual disease. It should be noted that certain institutions including the Mayo Clinic cap Continuous/Maintenance treatment at approximately 2 years, due to the lack of randomized comparative data, on the value of prolonged maintenance beyond 2 years. Continuous Therapy Versus Fixed Duration of Therapy in Patients With Newly Diagnosed Multiple Myeloma. Palumbo A, Gay F, Cavallo F, et al. J Clin Oncol 2015;33:3459-3466
FDA Approves First Oral Triplet Combination (NINLARO®, REVLIMID® and Dexamethasone) for Multiple Myeloma
SUMMARY: The FDA on November 20, 2015, approved NINLARO® (Ixazomib) in combination with REVLIMID® (Lenalidomide) and Dexamethasone for the treatment of patients with Multiple Myeloma who have received at least one prior therapy. Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, close to 27,000 new cases will be diagnosed in 2015 and 11,240 will die of the disease. Proteasomes are enzymes found in cells and they enable the breakdown of abnormal or mutant proteins. The amino acids from these proteins are recycled to make new proteins. Myeloma cells depend on the proteasomes to facilitate this metabolic function, to regulate their growth and survival. NINLARO® (Ixazomib) unlike VELCADE® (Bortezomib), is a second generation, oral, proteasome inhibitor, which disrupts protein metabolism in Myeloma cells, by inhibiting proteasomes and has an antiproliferative and pro-apoptotic effect.
The approval of NINLARO® was based a pivotal, multicenter, randomized, double-blind, placebo-controlled, phase III trial (TOURMALINE-MM1 study), in which 722 patients with Multiple Myeloma were randomized in a 1:1 ratio to receive either a combination of NINLARO®, REVLIMID® and Dexamethasone (N=360) or a combination of Placebo, REVLIMID® and Dexamethasone (n=362). NINLARO® was administered at 4 mg PO on days 1, 8, and 15 in combination with REVLIMID® 25 mg PO on days 1 thru 21 and Dexamethasone 40 mg PO on days 1, 8, 15, and 22 of a 28 day treatment cycle. Treatment was continued until disease progression or unacceptable toxicity. Enrolled patients had received 1 to 3 prior lines of therapy, which included VELCADE® (69%), THALOMID® (45%), and REVLIMID® (12%) and 77% of the patients had relapsed Multiple Myeloma. The median age of patients was 66 years. The primary end point of the study was Progression Free survival (PFS) and secondary endpoints included Objective Response Rate (ORR), safety, and Overall Survival.
At a prespecified interim analysis, the median PFS with the combination arm of NINLARO®, REVLIMID® and Dexamethasone was 20.6 months compared with 14.7 months for the combination group of Placebo, REVLIMID® and Dexamethasone (HR= 0.74, P=0.012).Secondary end points data was not mature at the time of this analysis. Patients in the NINLARO® group experienced more adverse events which included cytopenias, vomiting, diarrhea, peripheral neuropathy and skin rash.
The authors concluded that NINLARO® based oral triplet therapy significantly prolonged Progression Free Survival compared with REVLIMID® and Dexamethasone, with acceptable toxicities. Studies are underway, evaluating NINLARO® in newly diagnosed Myeloma patients as well as maintenance therapy in non-transplant patients. Ixazomib, an Investigational Oral Proteasome Inhibitor (PI), in Combination with Lenalidomide and Dexamethasone (IRd), Significantly Extends Progression-Free Survival (PFS) for Patients (Pts) with Relapsed and/or Refractory Multiple Myeloma (RRMM): The Phase 3 Tourmaline-MM1 Study (NCT01564537). Moreau P, Masszi T, Grzasko N, et al. 2015 ASH Annual Meeting; Orlando, FL; December 5-8, 2015. Abstract 727.
Targeting CD38 with Daratumumab Monotherapy in Multiple Myeloma
SUMMARY: The FDA recently assigned a priority review designation to Daratumumab, as a treatment for patients with double refractory Myeloma. Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, close to 27,000 new cases will be diagnosed in 2015 and 11,240 will die of the disease. The choice of first line therapy for patients with Myeloma may depend on transplant eligibility, comorbid conditions, cytogenetics and patient performance status. Following progression on first line therapy, single agent therapy with KYPROLIS® (Carfilzomib) has an Objective Response Rate of 24%, with a median duration of response of 7.4 months, in patient groups refractory to both VELCADE® (Bortezomib) and REVLIMID® (Lenalidomide). POMALYST® (Pomalidomide) in combination with Dexamethasone is superior to high dose Dexamethasone alone, with a significant improvement in the Progression Free Survival and Overall Survival, in patients with relapsed and refractory Multiple Myeloma. More recently, data became available for three triplet regimens in patients with relapsed Myeloma – 1) The addition of KYPROLIS® to REVLIMID® and Dexamethasone resulted in significant improvement in Progression Free Survival, when compared with REVLIMID® and Dexamethasone alone, in patients with relapsed Multiple Myeloma 2) A combination of FARYDAK® (Panobinostat), a histone deacetylase (HDAC) inhibitor, VELCADE® and Dexamethasone significantly improves Progression Free Survival in patients with relapsed and refractory Multiple Myeloma when compared to VELCADE® and Dexamethasone 3) Elotuzumab (HuLuc63), a monoclonal antibody that binds to the Signal Lymphocyte Activation Molecule – SLAMF7 protein (CS1, CD319), when added to REVLIMID® and Dexamethasone, reduced the risk of disease progression by 30% in patients with Relapsed/Refractory Multiple Myeloma, when compared with REVLIMID® and Dexamethasone.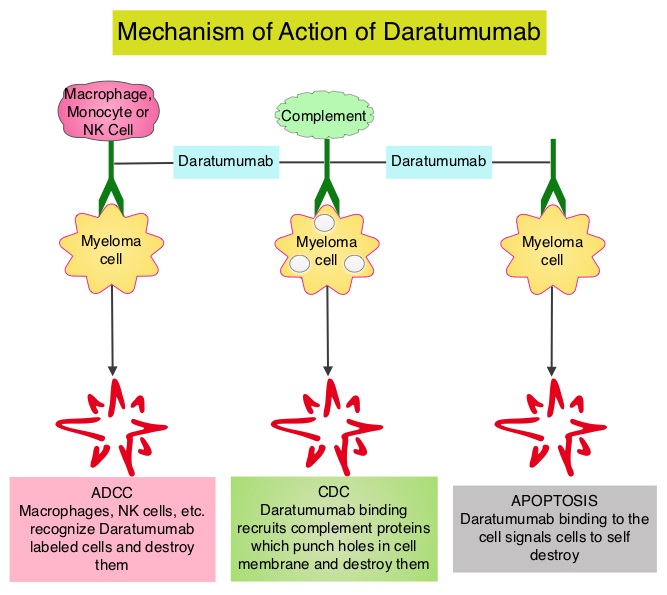
Daratumumab is a human IgG1 antibody that targets CD38, a transmembrane glycoprotein abundantly expressed on malignant plasma cells and with low levels of expression on normal lymphoid and myeloid cells. Daratumumab exerts its cytotoxic effect on myeloma cells by multiple mechanisms, including Antibody Dependent Cellular Cytotoxicity (ADCC), complement mediated cytotoxicity and direct apoptosis. Based on the anti-myeloma activity of Daratumumab in preclinical studies, a phase 1–2 clinical trial was conducted which involved patients with relapsed and refractory Myeloma, who were refractory to two or more prior lines of therapy. Patients in this study had received a median of four previous lines of therapy, 79% of the patients had disease that was refractory to their most recent therapy, including proteasome inhibitors and immunomodulators and 76% of the patients had also undergone autologous stem cell transplantation. This trial included a dose-expansion phase in which 30 patients received Daratumumab 8 mg/kg and 42 patients received 16 mg/kg, given once weekly for 8 doses, twice monthly for 8 doses, and monthly for up to 24 months. The primary end point was safety determined by frequency and severity of adverse events. Secondary end points included Objective Response Rate, duration of response, time to disease progression, Progression Free Survival, Overall Survival and pharmacokinetics.
It was noted that in the cohort that received Daratumumab 16 mg/kg, the overall response rate was 36% with a median Progression Free Survival of 5.6 months and 65% of the patients who had a response did not have disease progression at 12 months.
Infusion related reactions were mild and only 1% had grade 3 events. The other most common adverse events were pneumonia and thrombocytopenia. The authors concluded that Daratumumab has significant single agent activity in a very heavily pretreated and refractory Myeloma patient population, with a favorable safety profile. It remains to be seen if Daratumumab will be an important component of the induction, consolidation and maintenance phases, in the Myeloma treatment landscape. Targeting CD38 with Daratumumab Monotherapy in Multiple Myeloma. Lokhorst HM, Plesner T, Laubach JP, et al. N Engl J Med 2015; 373:1207-1219
KYPROLIS® (Carfilzomib)
The FDA on July 24, 2015 approved KYPROLIS® in combination with REVLIMID® (Lenalidomide) and Dexamethasone for the treatment of patients with relapsed multiple myeloma, who had received one to three prior lines of therapy. KYPROLIS® is a product of Onyx Pharmaceuticals, Inc., an Amgen subsidiary.
Monoclonal Antibody Combination Significantly Improves Progression Free Survival in Relapsed and Refractory Multiple Myeloma
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, close to 27,000 new cases will be diagnosed in 2015 and 11,240 will die of the disease. REVLIMID® (Lenalidomide) given along with weekly Dexamethasone, was associated with significantly improved Progression Free Survival (PFS) when administered until disease progression, in patients with newly diagnosed Multiple Myeloma. This combination of REVLIMID® and weekly Dexamethasone is considered a reference regimen (Control arm) for both newly diagnosed and relapsed Multiple Myeloma. Elotuzumab (HuLuc63) is a monoclonal antibody that binds to the Signal Lymphocyte Activation Molecule – SLAMF7 protein (CS1, CD319), which is highly expressed on Myeloma cells and also expressed on Natural Killer (NK) lymphocytes in the immune system. 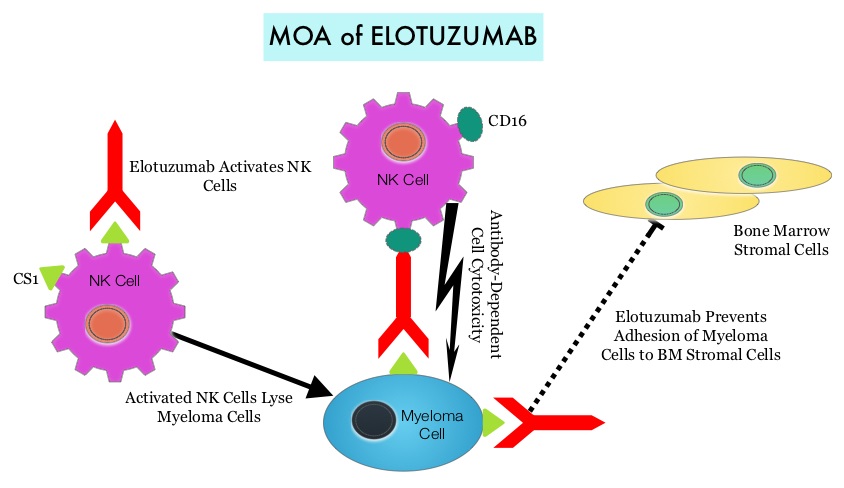 By virtue of its dual mechanism of action, it targets and destroys Myeloma cells and also enhances the activation of Natural Killer cells. Previously published phase Ib/II study, has shown encouraging activity, when Elotuzumab was combined with REVLIMID® and Dexamethasone, in patients with Relapsed/Refractory Multiple Myeloma (RRMM). ELOQUENT-2 is an open-label phase III trial in which 646 patients with Relapsed/Refractory Multiple Myeloma were randomized in a 1:1 ratio to receive Elotuzumab in combination with REVLIMID® and Dexamethasone (N=321) or REVLIMID® and Dexamethasone alone (N=325). Enrolled patients had 1–3 prior therapies and were not REVLIMID® refractory. Prior therapies included VELCADE® (Bortezomib), THALOMID® (Thalidomide) and REVLIMID®. Approximately 35% of the enrollees were refractory to the last therapy, 32% had del(17p) and 9% had t(4;14). The median age was 66 years. Elotuzumab was administered at 10 mg/kg IV weekly for the first two cycles and then once every 2 weeks thereafter. REVLIMID® was given at 25 mg orally on days 1 thru 21 of each cycle along with Dexamethasone 40 mg weekly. In the Elotuzumab group, Dexamethasone was dosed at 28 mg orally plus 8 mg IV on the weeks when Elotuzumab was administered. The cycle duration was 28 days. Treatment was administered until disease progression or unacceptable toxicity. Primary endpoints were Progression Free Survival (PFS) and Overall Response Rate (ORR). At a median follow up of 24 months, PFS in the Elotuzumab group was 19.4 months compared to 14.9 months in the REVLIMID®/Dexamethasone alone group (HR=0.70; P=0.0004). The 1-year PFS for the Elotuzumab versus control group was 68% vs 57% respectively and the 2-year PFS was 41% vs 27%. This benefit was seen across all subgroups including those with unfavorable cytogenetics. The ORR was 79% in the Elotuzumab group and 66% in the control group. (P = 0.0002). At the time of this interim analysis, more patients in the Elotuzumab group remained on therapy (35%) compared to the control group (21%) and treatment discontinuation was mainly for disease progression. Grade 3–4 toxicities occurred in 15% or more patients in the Elotuzumab group and included neutropenia and anemia. The authors concluded that Elotuzumab with its novel immunotherapeutic mechanism of action, when added to REVLIMID® and Dexamethasone, reduced the risk of disease progression by 30% in patients with Relapsed/Refractory MultipleMyeloma, and this was accomplished with manageable toxicities. Patients in this study are being followed up for long term outcomes including Overall Survival. Lonial S, Dimopoulos MA, Palumbo A, et al. ELOQUENT-2: A phase III, randomized, open-label study of lenalidomide (Len)/dexamethasone (dex) with/without elotuzumab (Elo) in patients (pts) with relapsed/refractory multiple myeloma (RRMM). J Clin Oncol. 2015;(suppl; abstr 8508).</s
By virtue of its dual mechanism of action, it targets and destroys Myeloma cells and also enhances the activation of Natural Killer cells. Previously published phase Ib/II study, has shown encouraging activity, when Elotuzumab was combined with REVLIMID® and Dexamethasone, in patients with Relapsed/Refractory Multiple Myeloma (RRMM). ELOQUENT-2 is an open-label phase III trial in which 646 patients with Relapsed/Refractory Multiple Myeloma were randomized in a 1:1 ratio to receive Elotuzumab in combination with REVLIMID® and Dexamethasone (N=321) or REVLIMID® and Dexamethasone alone (N=325). Enrolled patients had 1–3 prior therapies and were not REVLIMID® refractory. Prior therapies included VELCADE® (Bortezomib), THALOMID® (Thalidomide) and REVLIMID®. Approximately 35% of the enrollees were refractory to the last therapy, 32% had del(17p) and 9% had t(4;14). The median age was 66 years. Elotuzumab was administered at 10 mg/kg IV weekly for the first two cycles and then once every 2 weeks thereafter. REVLIMID® was given at 25 mg orally on days 1 thru 21 of each cycle along with Dexamethasone 40 mg weekly. In the Elotuzumab group, Dexamethasone was dosed at 28 mg orally plus 8 mg IV on the weeks when Elotuzumab was administered. The cycle duration was 28 days. Treatment was administered until disease progression or unacceptable toxicity. Primary endpoints were Progression Free Survival (PFS) and Overall Response Rate (ORR). At a median follow up of 24 months, PFS in the Elotuzumab group was 19.4 months compared to 14.9 months in the REVLIMID®/Dexamethasone alone group (HR=0.70; P=0.0004). The 1-year PFS for the Elotuzumab versus control group was 68% vs 57% respectively and the 2-year PFS was 41% vs 27%. This benefit was seen across all subgroups including those with unfavorable cytogenetics. The ORR was 79% in the Elotuzumab group and 66% in the control group. (P = 0.0002). At the time of this interim analysis, more patients in the Elotuzumab group remained on therapy (35%) compared to the control group (21%) and treatment discontinuation was mainly for disease progression. Grade 3–4 toxicities occurred in 15% or more patients in the Elotuzumab group and included neutropenia and anemia. The authors concluded that Elotuzumab with its novel immunotherapeutic mechanism of action, when added to REVLIMID® and Dexamethasone, reduced the risk of disease progression by 30% in patients with Relapsed/Refractory MultipleMyeloma, and this was accomplished with manageable toxicities. Patients in this study are being followed up for long term outcomes including Overall Survival. Lonial S, Dimopoulos MA, Palumbo A, et al. ELOQUENT-2: A phase III, randomized, open-label study of lenalidomide (Len)/dexamethasone (dex) with/without elotuzumab (Elo) in patients (pts) with relapsed/refractory multiple myeloma (RRMM). J Clin Oncol. 2015;(suppl; abstr 8508).</s
Efficacy and Safety Based on Duration of Treatment of Panobinostat Plus Bortezomib and Dexamethasone in Patients with Relapsed or Relapsed and Refractory Multiple Myeloma in the Phase 3 Panorama 1 Study
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, close to 27,000 new cases will be diagnosed in 2015 and 11,240 will die of the disease. The U.S. Food and Drug Administration (FDA) granted accelerated approval on February 23, 2015 to Panobinostat (FARYDAK®), in combination with VELCADE® (Bortezomib) and Dexamethasone, for the treatment of patients with Multiple Myeloma. The authors in the PANORAMA I trial evaluated the outcomes in previously treated advanced Multiple Myeloma patients, by taking advantage of the synergy between VELCADE®, a proteosome inhibitor and FARYDAK® (Panobinostat), a histone deacetylase (HDAC) inhibitor and treating these patients with a combination of these two agents. HDACs are a family of enzymes that play an important role in the regulation of gene expression.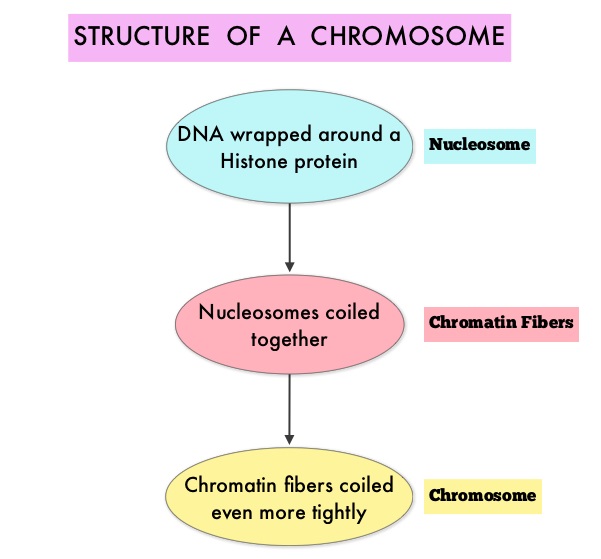 To briefly summarize the structure of a chromosome, individual loops of coiled double-helix DNA wrap around a histone protein to form a nucleosome. Nucleosomes are then coiled together to form chromatin fibers, which looks like beads on a string. The chromatin fibers are coiled even more tightly to form chromosomes. HDAC enzymes catalyze the removal of acetyl groups and regulate the level of acetylation of the histones and non-histone proteins and transcription of several genes. Hypoacetylation of histones has been associated with a condensed chromatin structure that results in the repression of gene transcription, whereas acetylated histones are associated with a more open chromatin structure and activation of gene transcription. HDACs are grouped into four major classes (Class I, II, III and IV) and regulate cell-cycle progression, cell survival, angiogenesis and immunity. The HDAC Class I enzymes are HDAC1, 2, 3 & 8 and are typically found in the nucleus where they are able to repress transcription. The HDAC Class II enzymes include HDAC4, 5, 6, 7, 9 and 10 and are able to move between the cytoplasm and nucleus and function in signal transduction. In Multiple Myeloma, the important enzyme to target is HDAC6.
To briefly summarize the structure of a chromosome, individual loops of coiled double-helix DNA wrap around a histone protein to form a nucleosome. Nucleosomes are then coiled together to form chromatin fibers, which looks like beads on a string. The chromatin fibers are coiled even more tightly to form chromosomes. HDAC enzymes catalyze the removal of acetyl groups and regulate the level of acetylation of the histones and non-histone proteins and transcription of several genes. Hypoacetylation of histones has been associated with a condensed chromatin structure that results in the repression of gene transcription, whereas acetylated histones are associated with a more open chromatin structure and activation of gene transcription. HDACs are grouped into four major classes (Class I, II, III and IV) and regulate cell-cycle progression, cell survival, angiogenesis and immunity. The HDAC Class I enzymes are HDAC1, 2, 3 & 8 and are typically found in the nucleus where they are able to repress transcription. The HDAC Class II enzymes include HDAC4, 5, 6, 7, 9 and 10 and are able to move between the cytoplasm and nucleus and function in signal transduction. In Multiple Myeloma, the important enzyme to target is HDAC6.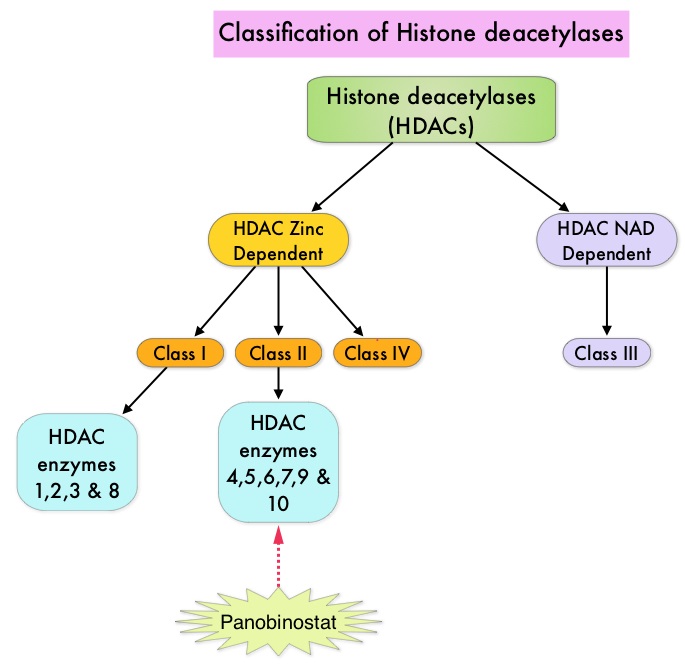 FARYDAK® is an oral, pan-histone deacetylase inhibitor which inhibits cell cycle progression and ultimately results in apoptosis. FARYDAK® inhibits the aggresome pathway of protein degradation which is upregulated when proteosome pathway is inhibited by VELCADE®. Based on preclinical data demonstrating synergy between VELCADE® and FARYDAK® in Myeloma, the PANORAMA 1 trial, enrolled patients with relapsed or refractory Multiple Myeloma who had received one to three prior lines of therapy and were not VELCADE® refractory. In this phase III trial, patients were randomly assigned to receive either FARYDAK® (N=387) or placebo (N=381), each along with IV VELCADE® and oral Dexamethasone. In this study, treatment was given in two 24 week phases. The first 24 week treatment phase was cycles 1 thru 8, where patients received placebo or FARYDAK® 20 mg orally QD 3 times a week for 2 weeks of a 3 week cycle; VELCADE® 1.3 mg/m2 IV twice weekly for 2 weeks of a 3 week cycle and Dexamethasone 20 mg PO on the day of and day after VELCADE®. Patients with clinical benefit (defined as complete response, partial response or stable disease, without significant toxicities) after the first eight cycles could proceed to the second phase of treatment in which FARYDAK® and Dexamethasone administration schedule remained the same but VELCADE® was administered once weekly for 2 weeks of the 3 week cycle. The median age was 63 years, 48% of patients had received at least two lines of therapy and 57% of patients had prior autologous stem cell transplantation and 43% had prior therapy with VELCADE®. The primary endpoint was Progression Free Survival (PFS) and secondary endpoints included Overall Survival (OS), Overall Response Rate (ORR), near Complete/Complete Response (nCR/CR) rate, Duration of Response (DOR), and safety. Among the patients enrolled in the FARYDAK® group (N = 387), 44% completed first phase of treatment and 26% completed the second phase of treatment. After a median follow up of 28 months, the primary end point of the study was met with a 37% decrease in the risk of disease progression in all the FARYDAK® group of patients compared to the placebo group (12 months vs 8.1 months, HR=0.63, P<0.0001). The median PFS was 14.65 months for those in the FARYDAK® group who completed the first phase of treatment and 17.64 months for those who completed the second phase of treatment. With regards to the secondary endpoints in the FARYDAK® vs placebo groups, the ORR was 60.7% vs 54.6% (P=0.87), nCR/CR rate was 27.6% vs 15.7% (P=0.00006), median duration of response was13.1months vs 10.9 months and median time to progression was 12.7 months vs 8.5 months respectively. It was noted that the nCR/CR rate was 52.9% for those patients who completed the second phase of treatment. The most common grade 3/4 adverse events in the FARYDAK® vs placebo arms included thrombocytopenia (67% vs 31%), neutropenia (35% vs 11%), and diarrhea (26% vs 8%) and these toxicities were manageable with dose reduction and supportive care. The authors concluded that a combination of FARYDAK®, VELCADE® and Dexamethasone significantly improves Progression Free Survival in patients with relapsed and refractory Multiple Myeloma, with manageable toxicities. Miguel JS, Hungria VTM , Yoon S, et al. 56th ASH Annual Meeting and Exposition, 2014. Abstract#4742
FARYDAK® is an oral, pan-histone deacetylase inhibitor which inhibits cell cycle progression and ultimately results in apoptosis. FARYDAK® inhibits the aggresome pathway of protein degradation which is upregulated when proteosome pathway is inhibited by VELCADE®. Based on preclinical data demonstrating synergy between VELCADE® and FARYDAK® in Myeloma, the PANORAMA 1 trial, enrolled patients with relapsed or refractory Multiple Myeloma who had received one to three prior lines of therapy and were not VELCADE® refractory. In this phase III trial, patients were randomly assigned to receive either FARYDAK® (N=387) or placebo (N=381), each along with IV VELCADE® and oral Dexamethasone. In this study, treatment was given in two 24 week phases. The first 24 week treatment phase was cycles 1 thru 8, where patients received placebo or FARYDAK® 20 mg orally QD 3 times a week for 2 weeks of a 3 week cycle; VELCADE® 1.3 mg/m2 IV twice weekly for 2 weeks of a 3 week cycle and Dexamethasone 20 mg PO on the day of and day after VELCADE®. Patients with clinical benefit (defined as complete response, partial response or stable disease, without significant toxicities) after the first eight cycles could proceed to the second phase of treatment in which FARYDAK® and Dexamethasone administration schedule remained the same but VELCADE® was administered once weekly for 2 weeks of the 3 week cycle. The median age was 63 years, 48% of patients had received at least two lines of therapy and 57% of patients had prior autologous stem cell transplantation and 43% had prior therapy with VELCADE®. The primary endpoint was Progression Free Survival (PFS) and secondary endpoints included Overall Survival (OS), Overall Response Rate (ORR), near Complete/Complete Response (nCR/CR) rate, Duration of Response (DOR), and safety. Among the patients enrolled in the FARYDAK® group (N = 387), 44% completed first phase of treatment and 26% completed the second phase of treatment. After a median follow up of 28 months, the primary end point of the study was met with a 37% decrease in the risk of disease progression in all the FARYDAK® group of patients compared to the placebo group (12 months vs 8.1 months, HR=0.63, P<0.0001). The median PFS was 14.65 months for those in the FARYDAK® group who completed the first phase of treatment and 17.64 months for those who completed the second phase of treatment. With regards to the secondary endpoints in the FARYDAK® vs placebo groups, the ORR was 60.7% vs 54.6% (P=0.87), nCR/CR rate was 27.6% vs 15.7% (P=0.00006), median duration of response was13.1months vs 10.9 months and median time to progression was 12.7 months vs 8.5 months respectively. It was noted that the nCR/CR rate was 52.9% for those patients who completed the second phase of treatment. The most common grade 3/4 adverse events in the FARYDAK® vs placebo arms included thrombocytopenia (67% vs 31%), neutropenia (35% vs 11%), and diarrhea (26% vs 8%) and these toxicities were manageable with dose reduction and supportive care. The authors concluded that a combination of FARYDAK®, VELCADE® and Dexamethasone significantly improves Progression Free Survival in patients with relapsed and refractory Multiple Myeloma, with manageable toxicities. Miguel JS, Hungria VTM , Yoon S, et al. 56th ASH Annual Meeting and Exposition, 2014. Abstract#4742
FARYDAK® (Panobinostat)
The FDA on February 23, 2015 granted accelerated approval to FARYDAK® for use in combination with VELCADE® (Bortezomib) and Dexamethasone for the treatment of patients with Multiple Myeloma who have received at least two prior regimens, including VELCADE® and an immunomodulatory agent. FARYDAK® capsules are a product of Novartis Pharmaceuticals.
IMBRUVICA® (Ibrutinib)
The FDA on January 29, 2015 approved IMBRUVICA® for the treatment of patients with Waldenstrom’s Macroglobulinemia (WM). IMBRUVICA® was initially approved in November 2013 for the treatment of patients with Mantle Cell Lymphoma (MCL) who have received at least one prior therapy. IMBRUVICA® also received approval in February 2014 for the treatment of Chronic Lymphocytic Leukemia (CLL) in patients who received at least one prior therapy and in July 2014 for the treatment of CLL with 17p deletion. IMBRUVICA® is an oral capsule and is a product of Pharmacyclics, Inc.
Carfilzomib, Lenalidomide, and Dexamethasone for Relapsed Multiple Myeloma
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, 24,050 new cases were diagnosed in 2014 and 11,090 died of the disease. KYPROLIS® (Carfilzomib) is a second generation selective, epoxyketone proteasome inhibitor and unlike VELCADE® (Bortezomib), proteasome inhibition with KYPROLIS® is irreversible. KYPROLIS® monotherapy is presently approved in the United States for use in patients with relapsed and refractory Multiple Myeloma following a phase 2b single arm study which showed a 24% overall response rate in this patient group. REVLIMID® (Lenalidomide) given along with weekly Dexamethasone, was associated with significantly improved Progression Free Survival (PFS) when administered until disease progression, in patients with newly diagnosed Multiple Myeloma. The combination of REVLIMID® and weekly Dexamethasone is considered a reference regimen for both newly diagnosed and relapsed multiple myeloma. VELCADE® in combination with REVLIMID® and Dexamethasone showed an overall response rate of 64% and a median PFS of 9.5 months in patients with relapsed and refractory Multiple Myeloma. Based on this background the authors conducted this randomized, open label, multicenter, phase III study in which the safety and efficacy of a combination of KYPROLIS® (Carfilzomib), REVLIMID® and weekly Dexamethasone (KYPROLIS® group) was compared with a combination of REVLIMID® and weekly Dexamethasone (control group), in patients with relapsed Multiple Myeloma. Seven hundred and ninety two (N=792) patients were randomly assigned in a 1:1 ratio to KYPROLIS® group (N=396) and control group (N=396). Eligible patients included those with Multiple Myeloma who had received one to three prior treatments which included VELCADE® or REVLIMID and Dexamethasone combination, provided that they did not have disease progression during treatment with these agents. The 28 day treatment cycle consisted of KYPROLIS® IV given on days 1, 2, 8, 9, 15, and 16 (starting dose, 20 mg/m2 on days 1 and 2 of cycle 1 with a target dose of 27 mg/m2 thereafter) during cycles 1 through 12 and on days 1, 2, 15, and 16 during cycles 13 through 18, following which KYPROLIS® was discontinued. REVLIMID® 25 mg PO was given on days 1 through 21 and Dexamethasone 40 mg PO was administered on days 1, 8, 15, and 22. Patients in both treatment groups received only REVLIMID® and Dexamethasone after cycle 18 until disease progression. Antiviral and antithrombotic prophylaxis was administered to patients in both treatment groups. The primary end point was Progression Free Survival and secondary end points included Overall Survival, the rate of overall response (partial response or better), response duration, health-related quality of life, and safety. The rate of clinical benefit (minimal response or better) was an exploratory end point. The study met its primary endpoint at the time of the pre-specified interim analysis with a significant improvement in the median Progression Free Survival for those patients in the KYPROLIS® group compared to the control group (26.3 months versus 17.6 months; HR=0.69; P=0.0001). This benefit in the PFS was demonstrated across all predefined subgroups. The median overall survival was not reached in either group and the 24 month overall survival rates were 73.3% and 65.0% in the KYPROLIS® and control groups, respectively (HR=0.79; P=0.04). The overall response rates (partial response or better) were 87.1% and 66.7% in the KYPROLIS® and control groups, respectively (P<0.001). Amongst the responders, 31.8% and 9.3% of patients in the respective groups had a complete response or better and 14.1% and 4.3% had a stringent complete response. Further, patients in the KYPROLIS® group reported superior health-related quality of life. Grade 3 or higher adverse events were reported in 83.7% and 80.7% of patients in the KYPROLIS® and control groups respectively. The authors concluded that the addition of KYPROLIS® to REVLIMID® and Dexamethasone resulted in significant improvement in PFS as compared with REVLIMID® and Dexamethasone alone, in patients with relapsed Multiple Myeloma. Additional benefits in the KYPROLIS® group included higher and deep response rates, improved health-related quality of life, a favorable risk–benefit profile and a trend towards improved Overall Survival. Stewart AK, Rajkumar SV, Dimopoulos MA, et al. N Engl J Med 2015; 372:142-152