SUMMARY: The FDA on June 12, 2025, approved Pembrolizumab (KEYTRUDA®) for adults with resectable locally advanced Head and Neck Squamous Cell Carcinoma (HNSCC) whose tumors express PD-L1 Combined Positive Score (CPS) of 1 or more, as determined by an FDA-approved test, as a single agent as neoadjuvant treatment, continued as adjuvant treatment in combination with Radiotherapy (RT) with or without Cisplatin after surgery, and then as a single agent.This is the first approval for HNSCC in 6 years and the first overall perioperative approval for locally advanced HNSCC.
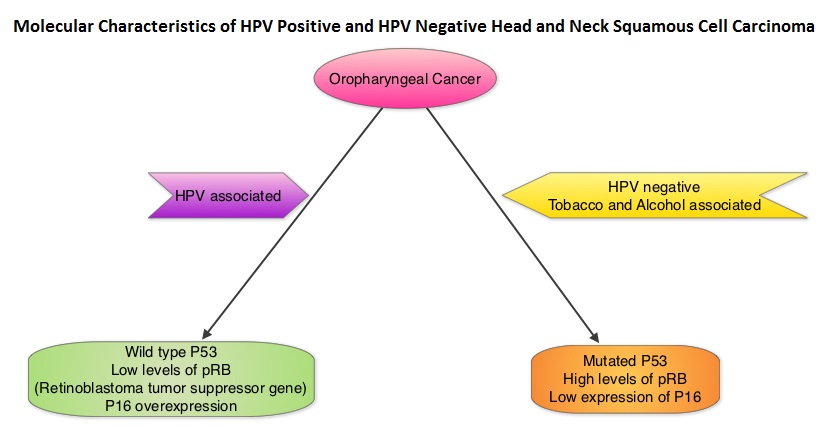
The American Cancer Society estimates that 59,660 new cases of cancer involving the oral cavity and pharynx will be diagnosed in the US in 2025 and 12,770 will die of the disease. The Head and Neck region includes the oral cavity, oropharynx, hypopharynx and larynx. Squamous Cell Carcinoma (SCC) of the Head and Neck accounts for about 3-5% of all cancers in the United States. Common risk factors include tobacco and alcohol use and Human PapillomaVirus (HPV) infection. Even though tobacco has long been associated with head and neck cancer development, cannabis has similar carcinogens.
The Standard of Care for patients with Stage III–IVA Head and Neck Squamous Cell Carcinoma (HNSCC) has remained largely static for nearly 2 decades: surgery followed by risk-adapted adjuvant radiotherapy, with or without concurrent chemotherapy. Despite refinements in technique and supportive care, relapse rates remain high, particularly among patients with adverse pathological features such as extranodal extension and positive margins.
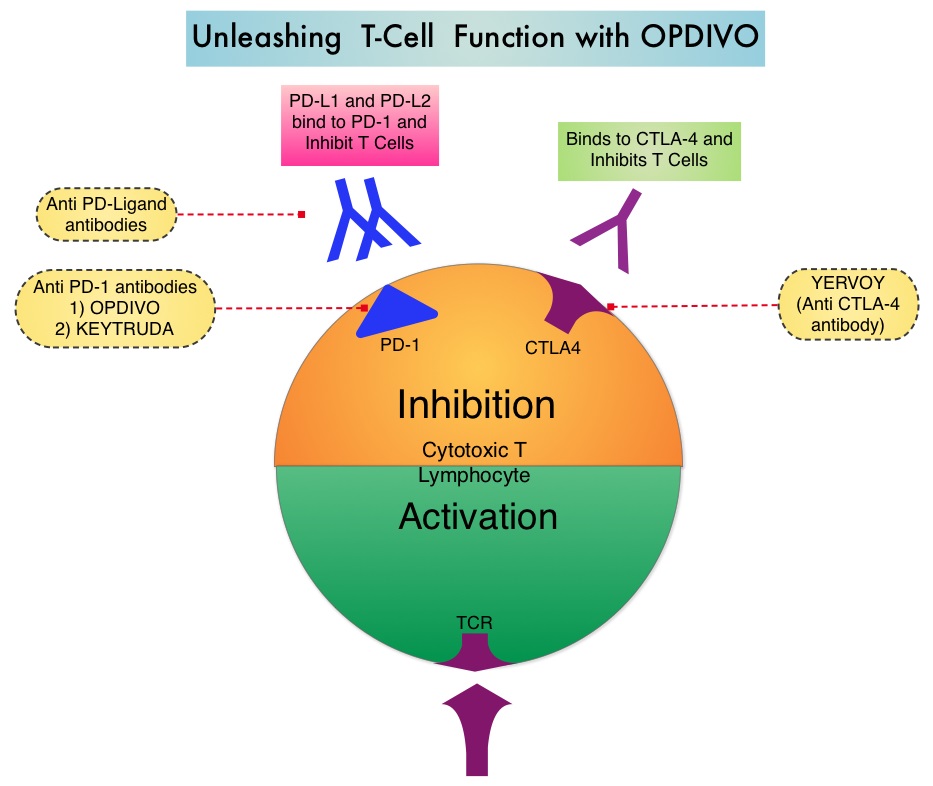
The treatment paradigm for Head and Neck cancer has been rapidly evolving with the recognition and better understanding of immune evasion and the role of immune checkpoints or gate keepers in suppressing antitumor immunity. Blocking the immune checkpoints unleashes the T cells, resulting in T cell proliferation, activation, and a therapeutic response. Checkpoint inhibitors administered in a neoadjuvant setting activates both the priming phase of immunity within tumor tissue, and the effector phase within the tumor microenvironment. It has been shown that neoadjuvant immunotherapy expands more T-cell clones than adjuvant treatment. Preclinical models have also demonstrated that both radiation therapy and Cisplatin chemotherapy increase the PD-L1 expression on the tumor, suggesting that combining radiotherapy with anti-PD-1 therapy could improve the outcomes.
Pembrolizumab (KEYTRUDA®) is a fully humanized, Immunoglobulin G4, monoclonal antibody and checkpoint inhibitor, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. Pembrolizumab has been shown to improve Overall Survival in patients with Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma
KEYNOTE-689, a landmark Phase 3 trial, has provided the most compelling evidence to date that perioperative immunotherapy, specifically Pembrolizumab, can significantly improve clinical outcomes for patients with resectable, locally advanced Head and Neck Squamous Cell Carcinoma (HNSCC). This international, randomized, placebo-controlled study enrolled 714 patients (N=714) with newly diagnosed, resectable, Stage III–IVA HNSCC of the oral cavity, oropharynx, larynx, or hypopharynx.
Patients were randomized 1:1 to receive:
- Investigational arm (N=356):
- 2 cycles of neoadjuvant Pembrolizumab (200 mg IV Q3W) starting about 3 weeks before surgery.
- Standard-of-care surgery.
- Up to 3 doses of Pembrolizumab administered concurrently with adjuvant chemoradiotherapy, with Cisplatin (depending on pathologic risk- positive margins <1 mm or extranodal extension present at surgery was considered high risk).
- 12 additional adjuvant doses of Pembrolizumab Q3W (total treatment duration: about 1 year).
- Control arm (N=358):
- Identical treatment structure, substituting placebo for Pembrolizumab.
PD-L1 expression was assessed via Combined Positive Score (CPS), and stratification included CPS ≥1 and CPS ≥10 subgroups, recognizing the prognostic and potentially predictive value of PD-L1 expression. The Primary endpoint was Event-Free Survival (EFS) by Blinded Independent Central Review, defined as time from randomization to disease progression, local/regional recurrence, distant metastasis, or death from any cause. Secondary endpoints included Overall Survival (OS) and Major Pathological Response.
The trial met its Primary endpoint of EFS. At median follow-up of 38.3 months, patients in the investigational arm had significantly improved EFS compared with the Standard of Care arm (median 51.8 months vs. 30.4 months; HR=0.73; P=0.0041). Patients who received Pembrolizumab who had a CPS score ≥10 derived the greatest benefit (median 59.7 months vs. 26.9 months; HR = 0.66; P=0.002) whereas the median EFS in the CPS ≥1 subgroup was 59.7 vs. 29.6 months (HR, 0.70; P = .0014).
Major pathological response defined as 90% or more tumor regression was also notably improved. Among all patients, the major pathological response rate was 9.4% with Pembrolizumab vs. 0% with Standard of Care (P < 0.00001). In the CPS ≥10 subgroup, the major pathological response rate reached 13.7%.
While the interim analysis did not demonstrate a statistically significant OS benefit, trends were favorable, particularly in the CPS ≥10 group (HR, 0.72; P =0.02). Further OS follow-up is ongoing.
Adverse events were consistent with known profiles of checkpoint inhibitors. Grade 3 or more Treatment-Related Adverse Events (TRAEs) occurred in 44.6% of the Pembrolizumab group and 42.9% in the Standard of Care group. Immune-mediated adverse events were observed in 43.2% of the Pembrolizumab arm, with hypothyroidism being the most common (24.7%). Mortality attributable to treatment was slightly higher with Pembrolizumab (1.1% vs. 0.3%).
The researchers concluded that perioperative Pembrolizumab is now emerging as a new standard of care in the treatment of resectable locally advanced HNSCC. The findings from this study underscore the importance of harnessing the immune system both before and after surgery. Neoadjuvant administration may prime the immune response when tumor antigen burden is highest, while adjuvant therapy may help eliminate residual microscopic disease.
Neoadjuvant and adjuvant pembrolizumab plus standard of care in resectable locally advanced head and neck squamous cell carcinoma: phase 3 KEYNOTE-689 study. Uppaluri R, et al. Abstract CT001. Presented at: American Association for Cancer Research Annual Meeting; April 25-30, 2025; Chicago.