
The FDA on May 15, 2020 approved QINLOCK® for adult patients with advanced GastroIntestinal Stromal Tumor (GIST), who have received prior treatment with 3 or more kinase inhibitors, including GLEEVEC® (Imatinib). QINLOCK® is a product of Deciphera Pharmaceuticals, LLC.
Tag: GI Stromal Tumor (GIST)
AYVAKIT® (Avapritinib)
The FDA on January 9, 2020 approved AYVAKIT® for adults with unresectable or metastatic GastroIntestinal Stromal Tumor (GIST) harboring a Platelet-Derived Growth Factor Receptor Alpha (PDGFRA) exon 18 mutation, including D842V mutations. AYVAKIT® is a product of Blueprint Medicines Corporation.
FDA Approves AYVAKIT®, a Precision Therapy, for Gastrointestinal Stromal Tumors
SUMMARY: The FDA on January 9, 2020, approved AYVAKIT® (Avapritinib) for adults with unresectable or metastatic GastroIntestinal Stromal Tumor (GIST) harboring a Platelet-Derived Growth Factor Receptor Alpha (PDGFRA) Exon 18 mutation, including D842V mutations. The American Cancer Society estimates that in the US, about 4000-5000 cases of GastroIntestinal Stromal Tumors (GISTs) are diagnosed each year. GI Stromal Tumor (GIST) is one of the most common types of Soft Tissue Sarcoma and can develop anywhere along the GI tract, but are primarily found in the stomach (60%) and small intestine (30%). GISTs originate from the interstitial cells of Cajal or related stem cells and are associated with activating mutations in KIT-CD117 (80%) or PDGFRA (5-10%). These two mutations are mutually exclusive and are important in the molecular pathogenesis of these tumors. PDGFRA-mutated GISTs are mostly of gastric origin and display epithelioid morphology or mixed epithelioid and spindle histology. Gain-of-function mutations lead to constitutive, ligand independent activation of PDGFRA and its downstream pathways, subsequently resulting in cell proliferation and apotosis inhibition. Primary PDGFRA mutations are found mainly in Exons 12 and 18 and rarely in Exon 14. The most frequent mutation results in an Exon 18 D842V substitution, detected in up to 75% of all PDGFRA-mutated tumors 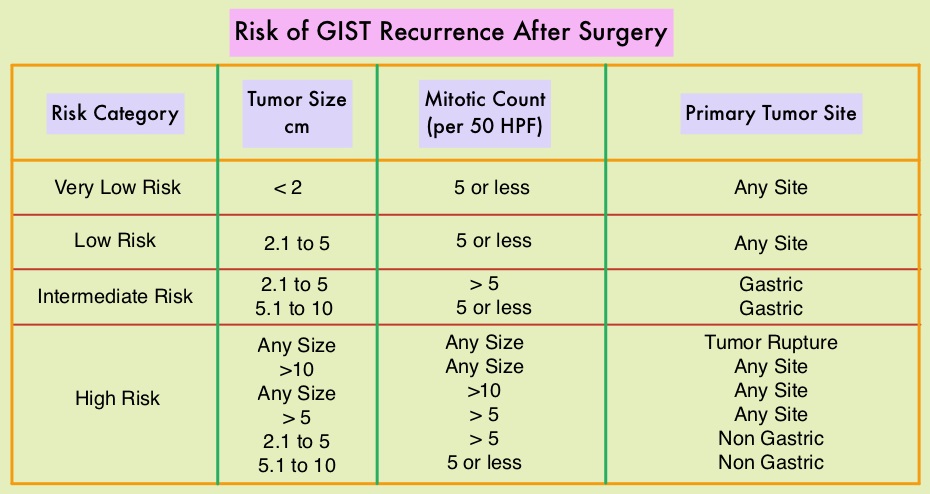
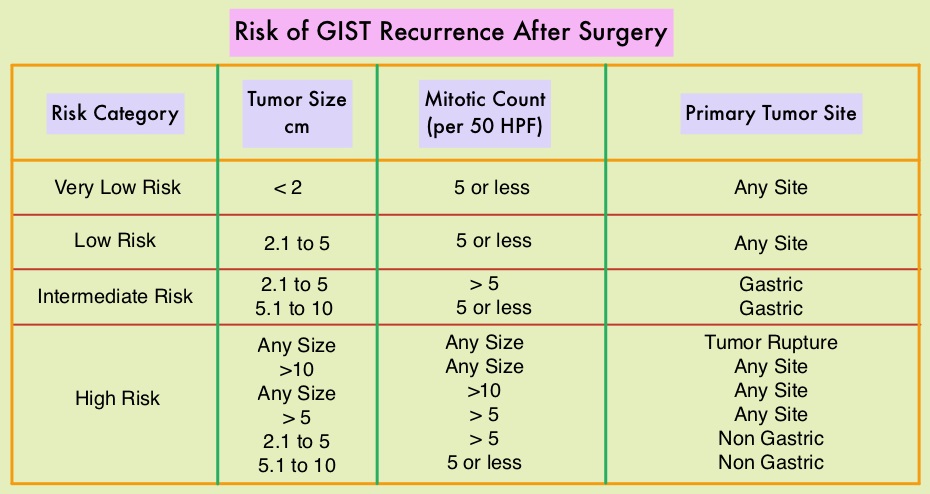
Most patients with GIST are diagnosed between 50 to 80 years of age, and patients may present with GI bleeding or as incidental findings during surgery or imaging, and occasionally with tumor rupture or bowel obstruction. Approximately two thirds of the patients with GISTs are cured with surgery but recurrences are frequent and this risk of relapse is dependent on the tumor size, mitotic rate and primary tumor site. The risk stratification of GISTs by Joensuu, unlike the NIH criteria, takes into account primary tumor site and tumor rupture as well, which can influence outcomes. Treatment of patients with advanced or metastatic GIST with Tyrosine Kinase Inhibitor GLEEVEC® (Imatinib) achieves high Objective Response and diseases stabilization rates. Patients with KIT Exon 9 mutation have a poor prognosis compared to those with KIT Exon 11 mutation (most common) and benefit from a higher dose of GLEEVEC® (800 mg daily). Following progression on GLEEVEC®, FDA approved therapies include SUTENT® (Sunitinib) and STIVARGA® (Regorafenib). Patients with PDGFRA D842V mutation are GLEEVEC® resistant.
AYVAKIT® is an oral, precision therapy, and is a potent and selective type 1 inhibitor of KIT and PDGFRA mutant kinases, and is also uniquely designed to selectively bind and inhibit D816V mutant KIT, the common driver of disease in approximately 95 percent of all Systemic Mastocytosis (SM) patients.
The present FDA approval was based on NAVIGATOR trial, designed to evaluate the safety, tolerability and clinical activity of AYVAKIT® in patients with unresectable or metastatic GIST. NAVIGATOR is a multicenter, single-arm, open-label trial, which enrolled 43 patients with GIST, harboring a PDGFRA Exon 18 mutation, including 38 patients with PDGFRA D842V mutations. Patients initially enrolled in this trial received AYVAKIT® at a starting dose of 400 mg orally once daily, which was later reduced to the recommended dose of 300 mg orally once daily due to toxicity. Treatment was continued until disease progression or unacceptable toxicity. The major efficacy endpoints were Overall Response Rate (ORR) and Duration of Response.
The ORR among patients harboring a PDGFRA Exon 18 mutation was 84%, with 7% Complete Responses and 77% Partial Responses. For the subgroup of patients with PDGFRA D842V mutations, the ORR was 89%, with 8% Complete Responses and 82% Partial Responses. The median Duration of Response was not reached with a median follow up for all patients of 10.6 months. Sixty one percent (61%) of the responding patients with Exon 18 mutations had a response lasting 6 months or longer. The most common Adverse Events across all grades included nausea, vomiting, decreased appetite, diarrhea, fatigue, anemia, cognitive effects, periorbital edema, increased lacrimation and peripheral edema.
It was concluded that AYVAKIT® shows unprecedented activity in D842V and other Exon 18 mutant PDGFRA GISTs, and is the first precision therapy approved to treat a genomically defined population of patients with GIST. Heinrich M, Jones RL, von Mehren M, et al. Clinical activity of avapritinib in ≥4th line (4L+) and PDGFRA exon 18 gastrointestinal stromal tumors (GIST). J Clin Oncol. 2019;37 (suppl; abstr 11022). DOI: 10.1200/JCO.2019.37.15_suppl.11022.
Late Breaking Abstract – ESMO 2019 Ripretinib Shows Dramatic Improvement in PFS in Heavily Pretreated GIST Patients
SUMMARY: The American Cancer Society estimates that in the US, about 4000-5000 cases of Gastro Intestinal Stromal Tumors (GISTs) are diagnosed each year. GI Stromal Tumor (GIST) is one of the most common types of Soft Tissue Sarcoma and can develop anywhere along the GI tract, but are primarily found in the stomach (60%) and small intestine (30%). GISTs originate from the interstitial cells of Cajal or related stem cells and are associated with activating mutations in KIT-CD117 (80%) or PDGFRA- Platelet-Derived Growth Factor Receptor-A (5-10%). These two mutations are mutually exclusive and are important in the molecular pathogenesis of these tumors. Approximately two thirds of the patients with GISTs are cured with surgery but recurrences are frequent and this risk of relapse is dependent on the tumor size, mitotic rate and primary tumor site. The risk stratification of GISTs by Joensuu, unlike the NIH criteria, takes into account primary tumor site and tumor rupture as well, which can influence outcomes.
 Treatment of patients with advanced or metastatic GIST with Tyrosine Kinase Inhibitor GLEEVEC® (Imatinib) achieves high Objective Response and diseases stabilization rates. Patients with KIT exon 9 mutation have a poor prognosis compared to those with KIT exon 11 mutation (most common) and benefit from a higher dose of GLEEVEC® (800 mg daily). The majority of PDGFRA mutations affect exon 18. It should also be noted that patients with PDGFRA D842V mutation are GLEEVEC® resistant. Following progression on GLEEVEC®, FDA approved therapies include SUTENT® (Sunitinib) and STIVARGA® (Regorafenib).
Treatment of patients with advanced or metastatic GIST with Tyrosine Kinase Inhibitor GLEEVEC® (Imatinib) achieves high Objective Response and diseases stabilization rates. Patients with KIT exon 9 mutation have a poor prognosis compared to those with KIT exon 11 mutation (most common) and benefit from a higher dose of GLEEVEC® (800 mg daily). The majority of PDGFRA mutations affect exon 18. It should also be noted that patients with PDGFRA D842V mutation are GLEEVEC® resistant. Following progression on GLEEVEC®, FDA approved therapies include SUTENT® (Sunitinib) and STIVARGA® (Regorafenib).
Ripretinib is an orally administered kinase switch-control inhibitor of KIT and PDGFRA at the JuxtaMembrane Domain (JMD), and the main activation loop switch. The agent restores the inhibitory JMD switch, which is often deactivated in GIST, and helps to stabilize the kinase in an inactive state. Ripretinib is a KIT and PDGFRA inhibitor that blocks initiating KIT mutations in exons 9, 11, 13, 14, 17, and 18, known to be present in GIST patients, and the D816V exon 17 mutation known to be present in patients with Advanced Systemic Mastocytosis. Ripretinib inhibits PDGFRA mutations in exon 18, including the D842V mutation that drives a subset of GIST. Ripretinib was specifically designed to improve the outcomes in GIST patients by inhibiting the full spectrum of known mutations in KIT and PDGFRA.
The INVICTUS trial is an international, multicenter, randomized, double-blind, placebo-controlled Phase III trial, in which the safety, efficacy and tolerability of Ripretinib was compared to placebo, among heavily pretreated patients with advanced GIST. In this study, 129 patients were randomized in a 2:1 ratio to receive Ripretinib at 150 mg orally daily (N=85) or placebo (N=44). Previous therapies for enrolled patients included at least GLEEVEC®, SUTENT® and STIVARGA®. Two-thirds of patients had received 3 prior therapies, and a third had received more than 4 lines of therapy. The median patient age was 60 years and the most common mutation was at KIT exon 11 (58%) followed by KIT exon 9 (16%). Patients with disease progression on placebo were allowed to cross over to receive Ripretinib. The Primary endpoint was Progression Free Survival.
It was noted that Ripretinib significantly reduced the risk of disease progression or death by 85% compared to placebo, with a median PFS of 6.3 months compared to 1.0 month in the placebo group (HR=0.15, P<0.0001). This PFS benefit was consistent across all assessed patient subgroups. Additionally, Ripretinib reduced the risk of death by 64% compared to placebo, with a median OS of 15.1 months compared to 6.6 months in the placebo group (HR=0.36; P=0.0004). According to the pre-specified hierarchical testing procedure of the endpoints for the study, statistical significance for OS could not be established. The most common Adverse Events with Ripretinib included alopecia, nausea, abdominal pain, constipation and myalgias.
It was concluded that Ripretinib significantly improves Progression Free Survival and very likely also improves Overall Survival in heavily pretreated patient population with Gastrointestinal Stromal Tumors. INVICTUS: A Phase 3, International, Double-Blind, Placebo-Controlled Study to Assess the Safety and Efficacy of Ripretinib as 4th Line Therapy or more in Patients with Advanced Gastrointestinal Stromal Tumors (GIST) Who Have Received Treatment with Prior Anticancer Therapies (NCT03353753). van Mehren M, Attia S, Bauer S, et al. Presented at 2019 ESMO Congress; September 27 to October 1, 2019; Barcelona, Spain. Abstract LBA87.
Adjuvant GLEEVEC® Improves Overall Survival in High Risk GI Stromal Tumors
SUMMARY: The American Cancer Society estimates that in the US, about 4000-5000 cases of Gastro Intestinal Stromal Tumors (GISTs) are diagnosed each year. GI Stromal Tumor (GIST) is one of the most common types of Soft Tissue Sarcoma and can develop anywhere along the GI tract, but are primarily found in the stomach. GISTs originate from the interstitial cells of Cajal or related stem cells and are associated with activating mutations in KIT or PDGFRA (Platelet-Derived Growth Factor Receptor-A). These two mutations are mutually exclusive and are important in the molecular pathogenesis of these tumors. Treatment of patients with advanced or metastatic GIST with Tyrosine Kinase Inhibitor GLEEVEC® (Imatinib) achieves high Objective Response and diseases stabilization rates. Patients with KIT exon 9 mutation have a poor prognosis compared to those with KIT exon 11 mutation and benefit from a higher dose of GLEEVEC® (800 mg daily). It should also be noted that patients with PDGFRA D842V mutation are GLEEVEC® resistant. Approximately two thirds of the patients with GISTs are cured with surgery but recurrences are frequent and this risk of relapse is dependent on the tumor size, mitotic rate and primary tumor site. The risk stratification of GISTs by Joensuu, unlike the NIH criteria, takes into account primary tumor site and tumor rupture as well, which can influence outcomes.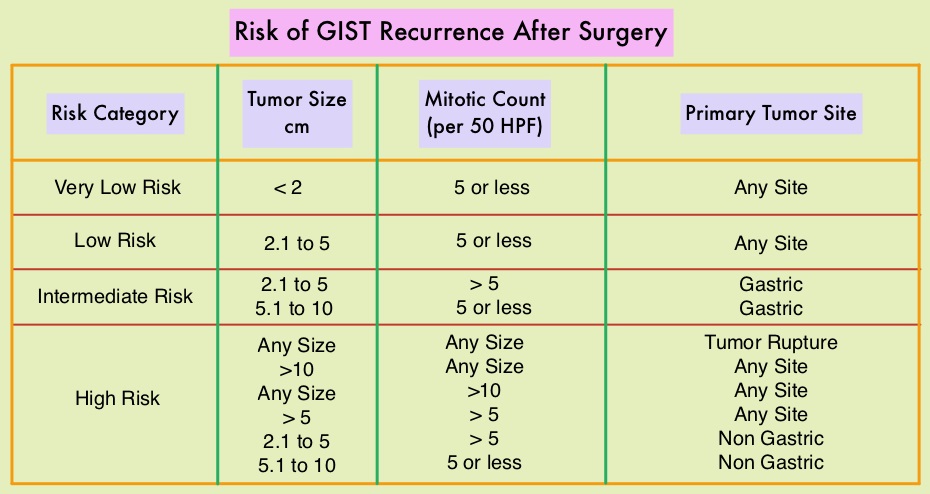
Adjuvant therapy with three years of GLEEVEC®, following curative surgery of high risk GISTs, is recommended and has been shown to improve Recurrence Free Survival (RFS). However, whether adjuvant GLEEVEC® improves overall survival has remained unclear. To address this further the authors in this publication performed a second planned analysis of the SSGXVIII/AIO trial after a longer follow up. In this open label study, 400 patients following surgery were randomly assigned to receive adjuvant GLEEVEC® for either 12 months (N=200) or for 36 months (N=200). Eligible patients had completely resected, KIT-positive GIST, with high risk features, per the modified National Institutes of Health criteria. The median age was 61 years and the primary objective was Recurrence Free Survival (RFS), and the secondary objectives included Overall Survival and Safety.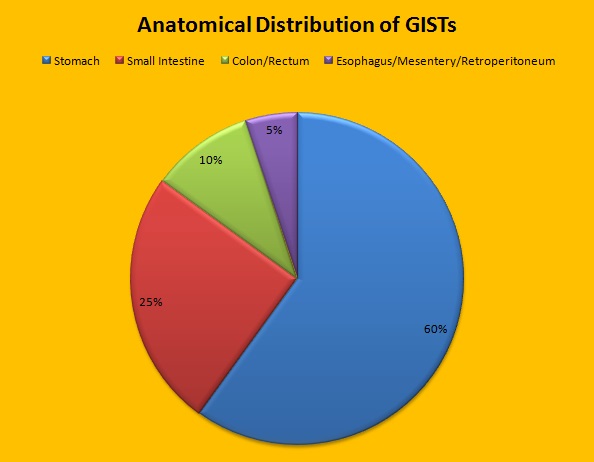
The second planned analysis was done 3 years after the first analysis of the trial and was intended to compare Overall Survival between the treatment groups, after additional follow up of these patients. The median follow up was 90 months. It was noted that the patients who were treated with 36 months of adjuvant GLEEVEC® had a longer RFS than those who were treated for 12 months (5-year RFS was 71.1% versus 52.3%, HR=0.60; P<0.001). The Overall Survival (OS) also favored the 36 month treatment group compared with the 12 month treatment group (5-year OS was 91.9% versus 85.3%, HR=0.60; P=0.036).
The authors concluded that 3 years of adjuvant GLEEVEC® therapy results in longer Overall Survival than 1 year of adjuvant GLEEVEC®, with a superior 5-year survival rate, in patients with high-risk GIST. Trials are underway evaluating the benefit of adjuvant GLEEVEC® for longer than 3 years. Adjuvant Imatinib for High-Risk GI Stromal Tumor: Analysis of a Randomized Trial. Joensuu H, Eriksson M, Hall KS, et al. J Clin Oncol 2016;34:244-250
KIT and PDGFRA Mutations and the Risk of GI Stromal Tumor Recurrence
SUMMARY: It is estimated that approximately 5000 new cases of GastroIntestinal Stromal Tumors (GISTs) will be diagnosed in the United States in 2015. Even though most of the GIST cases are sporadic, hereditary GIST has been well documented in individuals with von Recklinghausen’s neurofibromatosis as well as a familial syndrome in children and as a rare constellation of gastric GIST, pulmonary chondroma and extra adrenal paraganglioma (Carney’s Triad). Presently GLEEVEC® (Imatinib) is approved by the FDA for the adjuvant treatment of adult patients following resection of Kit (CD117) positive GIST and SUTENT® (Sunitinib) is approved in this setting if patients are intolerant to GLEEVEC®. GISTs are mesenchymal neoplasms and originate from Interstitial Cells of Cajal (ICC) or their precursors. These cells normally regulate GI motility ie. peristaltic wave and are considered pacemaker cells of the gut. They are located throughout the GI tract and transmit signals along the bowel.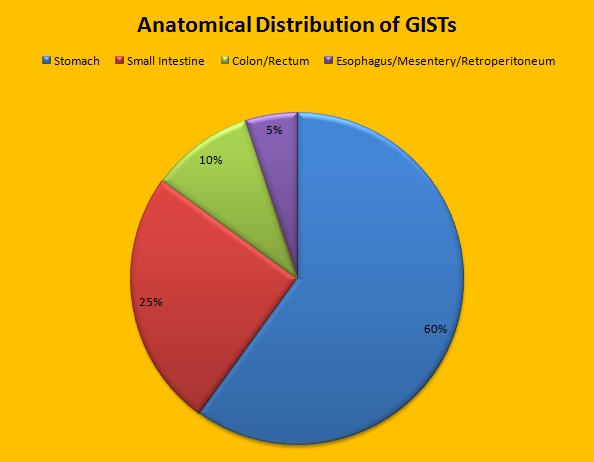 Approximately 60% of the primary GISTs originate in the stomach, 25% in the small intestine, 10% in the colon and rectum and the rest at other sites such as the esophagus, mesentery and retroperitoneum. GISTs were misclassified as leiomyomas or leiomyosarcomas until 1998, when the discovery of mutations in the c-KIT oncogene, lead to a better understanding of these tumors. C-KIT oncogene encodes the transmembrane KIT receptor tyrosine kinase. Approximately 85% of the GISTs have activating (gain of function) KIT mutations and are positive for the CD117 antigen, an epitope of KIT receptor tyrosine kinase. Positive CD117 by ImmunoHistoChemistry (IHC) is however not specific for GIST, as weak reactivity occurs with other mesenchymal tumors. IHC staining for protein kinase C theta and DOG1 are helpful in distinguishing GIST from other mesenchymal tumors, particularly those that are KIT-negative. DOG1 (Discovered On GIST 1) is a protein of unknown function that is expressed strongly in GISTs and is rarely expressed in other mesenchymal neoplasms. KIT mutations in GISTs occur in Exon 9 (10%), Exon 11 (67%), Exon 13 (1%) and Exon 17 (1%). About 5% of the GISTs have activating mutation in the Platelet-Derived Growth Factor Receptor alpha (PDGFRA) gene which encodes for another tyrosine kinase receptor. Approximately 10% to 20% of GISTs have no KIT or PDGFRA mutations and are referred as wild-type GISTs. Mutational status is important as they may predict response to GLEEVEC® and also have prognostic significance. Patients with KIT exon 11 mutations are most sensitive and have a much higher response to GLEEVEC® whereas those with KIT exon 9 mutation or wild-type c-KIT may require a higher dose of GLEEVEC® (800 mg daily dose). KIT exon 11 mutations affecting the codons 557 and 558 is an independent adverse prognostic factor and associated with higher incidence of metastases whereas GISTs with KIT exon 9 mutations usually arise in the small bowel and are associated with frequent recurrences. GISTs with PDGFRA mutations in general have low mitotic count and low malignant potential and those with PDGFRA exon 18 mutation have favorable survival outcomes and located in the stomach. They are however resistant to GLEEVEC®. Although mutated KIT and PDGFRA have been identified as important driver mutations for GIST oncogenesis, the clinical significance of their single mutations has been unclear. To address this, the authors in this study identified 3067 patients with GIST from databases who had macroscopically complete tumor excision and had no detectable metastases at the time of diagnosis. Information on mutation analysis was available on 1505 tumors. The researchers then analyzed associations between KIT and PDGFRA mutations and Recurrence Free Survival (RFS) in this patient population treated with surgery alone.
Approximately 60% of the primary GISTs originate in the stomach, 25% in the small intestine, 10% in the colon and rectum and the rest at other sites such as the esophagus, mesentery and retroperitoneum. GISTs were misclassified as leiomyomas or leiomyosarcomas until 1998, when the discovery of mutations in the c-KIT oncogene, lead to a better understanding of these tumors. C-KIT oncogene encodes the transmembrane KIT receptor tyrosine kinase. Approximately 85% of the GISTs have activating (gain of function) KIT mutations and are positive for the CD117 antigen, an epitope of KIT receptor tyrosine kinase. Positive CD117 by ImmunoHistoChemistry (IHC) is however not specific for GIST, as weak reactivity occurs with other mesenchymal tumors. IHC staining for protein kinase C theta and DOG1 are helpful in distinguishing GIST from other mesenchymal tumors, particularly those that are KIT-negative. DOG1 (Discovered On GIST 1) is a protein of unknown function that is expressed strongly in GISTs and is rarely expressed in other mesenchymal neoplasms. KIT mutations in GISTs occur in Exon 9 (10%), Exon 11 (67%), Exon 13 (1%) and Exon 17 (1%). About 5% of the GISTs have activating mutation in the Platelet-Derived Growth Factor Receptor alpha (PDGFRA) gene which encodes for another tyrosine kinase receptor. Approximately 10% to 20% of GISTs have no KIT or PDGFRA mutations and are referred as wild-type GISTs. Mutational status is important as they may predict response to GLEEVEC® and also have prognostic significance. Patients with KIT exon 11 mutations are most sensitive and have a much higher response to GLEEVEC® whereas those with KIT exon 9 mutation or wild-type c-KIT may require a higher dose of GLEEVEC® (800 mg daily dose). KIT exon 11 mutations affecting the codons 557 and 558 is an independent adverse prognostic factor and associated with higher incidence of metastases whereas GISTs with KIT exon 9 mutations usually arise in the small bowel and are associated with frequent recurrences. GISTs with PDGFRA mutations in general have low mitotic count and low malignant potential and those with PDGFRA exon 18 mutation have favorable survival outcomes and located in the stomach. They are however resistant to GLEEVEC®. Although mutated KIT and PDGFRA have been identified as important driver mutations for GIST oncogenesis, the clinical significance of their single mutations has been unclear. To address this, the authors in this study identified 3067 patients with GIST from databases who had macroscopically complete tumor excision and had no detectable metastases at the time of diagnosis. Information on mutation analysis was available on 1505 tumors. The researchers then analyzed associations between KIT and PDGFRA mutations and Recurrence Free Survival (RFS) in this patient population treated with surgery alone.
Taking into consideration the tumor size and mitotic rate in addition to mutational analysis data, they made several important observations. Patients with PDGFRA mutations had more favorable RFS than those with KIT mutations (HR=0.34; P =0 .004). They also pointed out that not all KIT Exon 11 mutations are equal and are associated with variable outcomes and clinical features. They concluded that mutation analysis in GISTs may provide clinically useful prognostic information in a patient groups treated with surgery alone, but the standard prognostic factors such as mitotic rate are generally stronger predictors for RFS even in subsets of patients with an identical KIT or PDGFRA mutation. Therefore tumor mutational status should be interpreted in the context of other standard prognostic factors. They did however note that majority of the patients with PDGFRA mutations and those with KIT exon 11 duplication mutation or deletion of one codon have favorable RFS with surgery alone and are usually not candidates for adjuvant therapy. Joensuu H, Rutkowski P, Nishida T, et al. J Clin Oncol 2015; 33:634-642
Efficacy and safety of regorafenib for advanced gastrointestinal stromal tumours after failure of imatinib and sunitinib (GRID) an international, multicentre, randomised, placebo-controlled, phase 3 trial
SUMMARY: STIVARGA® (Regorafenib) is an oral multikinase inhibitor. In this international trial, 199 patients with advanced GIST who had progressed on both GLEEVEC® (Imatinib) and SUTENT® (Sunitinib) were randomized in a 2:1 ratio to receive either STIVARGA® or placebo. The primary endpoint was progression-free survival (PFS). Patients in the STIVARGA® group had a statistically significant 3.9 month improvement in progression-free survival (PFS) compared to placebo (4.8 months vs 0.9 months; Hazard Ratio = 0.27; P<.0001). Following progression, 85% of the patients assigned to the placebo group crossed over to the STIVARGA® group. Treatment was well tolerated and the most common adverse events included hypertension, hand-foot syndrome and diarrhea. There is now a new treatment option for patients with GIST who progress on GLEEVEC® and SUTENT®. Demetri GD, Reichardt P, Kang Y, et al. The Lancet. 2013;381:295-302
STIVARGA® (Regorafenib)
The FDA on February 25, 2013 approved the use of STIVARGA® for the treatment of patients with advanced GastroIntestinal Stromal Tumors (GIST) that are unresectable or metastatic and are no longer responding to GLEEVEC® (Imatinib) and SUTENT® (Sunitinib). The FDA initially approved STIVARGA® in 2012 for the treatment of patients with metastatic colorectal cancer (mCRC) who have been previously treated with fluoropyrimidine, ELOXATIN® (Oxaliplatin), and CAMPTOSAR® (Irinotecan) based chemotherapy, an anti-VEGF therapy, and, if KRAS wild type, an anti-EGFR therapy. STIVARGA® is a product of Bayer HealthCare Pharmaceuticals, Inc.
STIVARGA® (Regorafenib) for advanced GIST
STIVARGA® is an oral multikinase inhibitor. In a study published in the January 2013 issue of THE LANCET, treatment with STIRVAGA® in patient population resistant or refractory to GLEEVEC® and SUTENT® resulted in significant improvement in progression free survival. This is the third agent approved by the FDA for advanced GIST. As patients with advanced GIST live longer, newer agents with unique mechanism of action will take center stage.
GLEEVEC® (Imatinib)
The FDA on January 31, 2012 granted regular approval for GLEEVEC® (Imatinib mesylate) for the adjuvant treatment of adult patients for a period of 36 months following complete gross resection of Kit (CD117) positive Gastrointestinal Stromal Tumors (GIST). GLEEVEC® is a product of Novartis Pharmaceuticals.