SUMMARY: The ASCO guideline for Antiemetics in oncology was updated by the ASCO Expert Panel following a systematic review of 41publications from November 2009 thru June 2016. The recommendations in this guideline are most definitive for adults who are treated with single-day IV chemotherapy. This topic has been divided into Part I and Part II for easy reading. Part II is continued in the second article of this e NewsLetter.
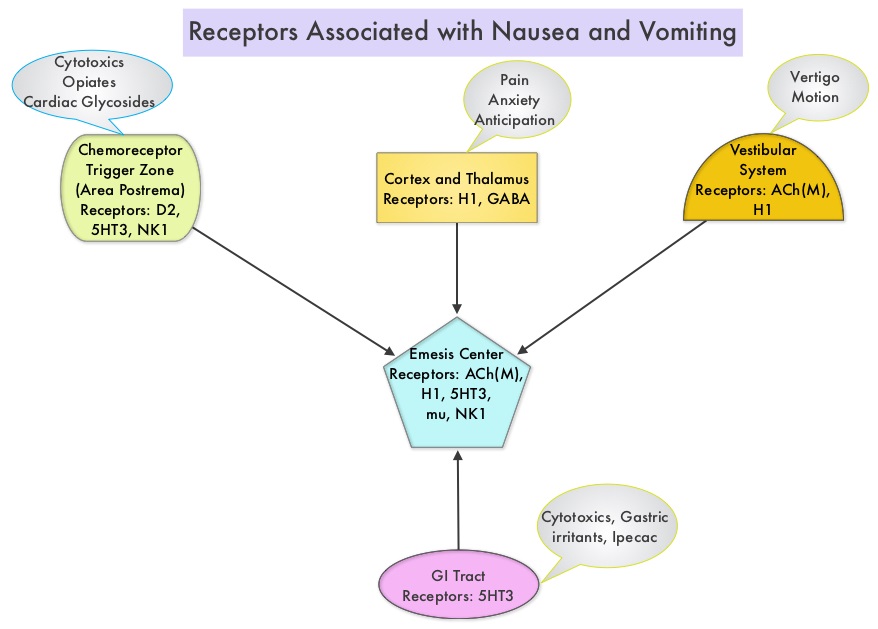
Guideline Question: What are the most effective strategies for preventing or managing nausea and vomiting due to antineoplastic agents or radiation therapy?
Target Population: Adults and children who receive antineoplastic agents and adults who undergo radiation therapy for cancer.
Target Audience: Medical and Radiation Oncologists, Oncology Nurses, Nurse Practitioners, Physician Assistants, Oncology Pharmacists, and Patients with cancer
KEY RECOMMENDATIONS – PART I
Adult Patients
High-emetic-risk antineoplastic agents
• (Updated) Adult patients who are treated with Cisplatin and other high-emetic-risk single agents should be offered a four-drug combination of a Neurokinin 1 (NK1) receptor antagonist, a Serotonin (5-HT3) receptor antagonist, Dexamethasone, and Olanzapine. Dexamethasone and Olanzapine should be continued on days 2 to 4.
• (Updated) Adult patients who are treated with an Anthracycline combined with Cyclophosphamide should be offered a four-drug combination of an NK1 receptor antagonist, a 5-HT3 receptor antagonist, Dexamethasone, and Olanzapine. Olanzapine should be continued on days 2 to 4.
Moderate-emetic-risk antineoplastic agents
• (Updated) Adult patients who are treated with Carboplatin AUC 4 or more should be offered a three-drug combination of an NK1 receptor antagonist, a 5-HT3 receptor antagonist, and Dexamethasone.
• (Updated) Adult patients who are treated with moderate-emetic-risk antineoplastic agents, excluding Carboplatin AUC 4 or more, should be offered a two-drug combination of a 5-HT3 receptor antagonist (day 1) and Dexamethasone (day 1).
• (Updated) Adult patients who are treated with Cyclophosphamide, Doxorubicin, Oxaliplatin, and other moderate-emetic-risk antineoplastic agents that are known to cause delayed nausea and vomiting may be offered Dexamethasone on days 2 to 3.
Low-emetic-risk antineoplastic agents
• (Updated) Adult patients who are treated with low-emetic-risk antineoplastic agents should be offered a single dose of a 5-HT3 receptor antagonist or a single 8-mg dose of Dexamethasone before antineoplastic treatment.
Minimal-emetic-risk antineoplastic agents
• (Reworded for clarity) Adult patients who are treated with minimal-emetic-risk antineoplastic agents should not be offered routine antiemetic prophylaxis.
Antineoplastic combinations
• (Reworded for clarity) Adult patients who are treated with antineoplastic combinations should be offered antiemetics that are appropriate for the component antineoplastic agent of greatest emetic risk.
Adjunctive drugs
• (Updated) Lorazepam is a useful adjunct to antiemetic drugs, but is not recommended as a single-agent antiemetic.
Cannabinoids
• (New) Evidence remains insufficient for a recommendation regarding treatment with medical marijuana for the prevention of nausea and vomiting in patients with cancer who receive chemotherapy or radiation therapy. Evidence is also insufficient for a recommendation regarding the use of medical marijuana in place of the tested and US FDA-approved cannabinoids, Dronabinol and Nabilone, for the treatment of nausea and vomiting caused by chemotherapy or radiation therapy.
Complementary and alternative therapies
• (Reworded for clarity) Evidence remains insufficient for a recommendation for or against the use of ginger, acupuncture/acupressure, and other complementary or alternative therapies for the prevention of nausea and vomiting in patients with cancer.
High-dose chemotherapy with stem cell or bone marrow transplantation
• (Updated) Adult patients who are treated with high-dose chemotherapy and stem cell or bone marrow transplantation should be offered a three-drug combination of an NK1 receptor antagonist, a 5-HT3 receptor antagonist, and Dexamethasone.
Multiday antineoplastic therapy
• (Reworded for clarity) Adult patients who are treated with multiday antineoplastic agents should be offered antiemetics before treatment that are appropriate for the emetic risk of the antineoplastic agent administered on each day of the antineoplastic treatment and for 2 days after the completion of the antineoplastic regimen.
• (Strengthened) Adult patients who are treated with 4- or 5-day Cisplatin regimens should be offered a three-drug combination of an NK1 receptor antagonist, a 5-HT3 receptor antagonist, and Dexamethasone.
Continued….. in Article 2 of this e NewsLetter
Antiemetics: American Society of Clinical Oncology Clinical Practice Guideline Update. Hesketh PJ, Kris MG, Basch E, et al. DOI: 10.1200/JCO.2017.74.4789 Journal of Clinical Oncology – published online before print July 31, 2017