SUMMARY: The American Cancer Society estimates that in the US, about 31,510 new cases of Gastric cancer will be diagnosed in 2026 and about 10,740 people will die of the disease. It is one of the leading causes of cancer-related deaths in the world. Several hereditary syndromes such as Hereditary Diffuse Gastric Cancer (HDGC), Lynch syndrome (Hereditary Nonpolyposis Colorectal Cancer) and Familial Adenomatous Polyposis (FAP) have been associated with a predisposition for stomach cancer. Additionally, one of the strongest risk factor for Gastric adenocarcinoma is infection with Helicobacter pylori (H.pylori), which is a gram-negative, spiral-shaped microaerophilic bacterium.
Persistent Unmet Need in HER2-Positive Disease
The Human Epidermal growth factor Receptor (HER) or erbB family of receptors, consist of HER1, HER2, HER3 and HER4. Approximately 20% of patients with GastroEsophageal Adenocarcinoma (GEA), encompassing gastric, gastroesophageal junction, and esophageal adenocarcinomas, harbor HER2-positive tumors. Despite the incorporation of HER2-directed therapy into first-line management more than a decade ago, long-term outcomes remain suboptimal. With Trastuzumab (HERCEPTIN®) plus chemotherapy, median Progression-Free Survival (PFS) has historically hovered around 10 months, and median Overall Survival (OS) around 20 months.
More recently, the addition of immune checkpoint inhibition has modestly improved outcomes in selected patients. Based on KEYNOTE-811, Pembrolizumab (KEYTRUDA®) plus Trastuzumab and chemotherapy is now standard for PD-L1–positive tumors. However, early relapse, often within the first year, remains common, underscoring the need for more effective HER2-targeted strategies.
Zanidatamab: A Next-Generation HER2-Targeted Approach
Preclinical and clinical data suggest greater antibody saturation on HER2-expressing tumor cells than with Trastuzumab or Pertuzumab (PERJETA®).
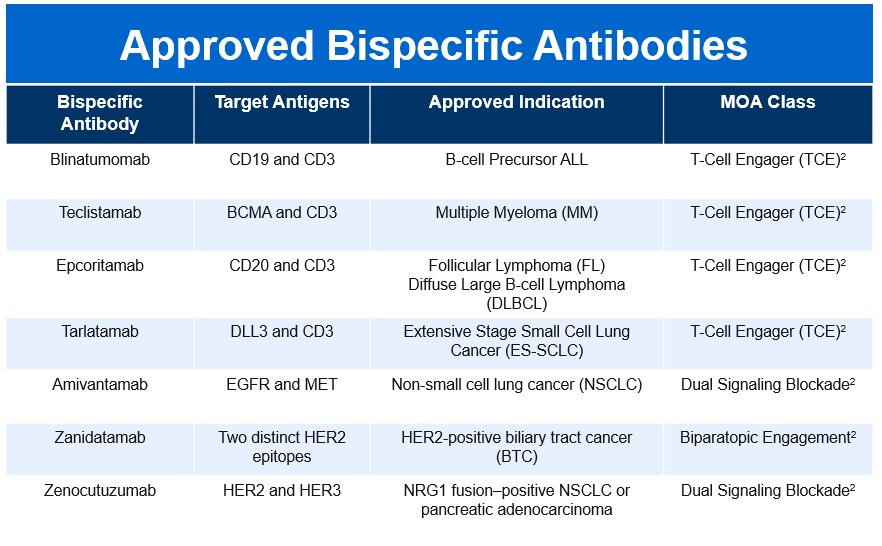
Zanidatamab (ZIIHERA®) is a novel, humanized IgG1 bispecific monoclonal antibody designed to bind two non-overlapping extracellular domains of HER2 (ECD2 and ECD4). This biparatopic binding leads to enhanced HER2 receptor clustering, internalization, and downregulation, resulting in more complete inhibition of HER2 signaling compared with single-epitope antibodies. Beyond direct signal blockade, Zanidatamab’s unique binding geometry promotes robust immune-mediated antitumor activity, including Complement-Dependent Cytotoxicity (CDC), Antibody-Dependent Cellular Cytotoxicity (ADCC), and Antibody-Dependent Cellular Phagocytosis (ADCP).
Zanidatamab’s clinical momentum was reinforced by its FDA accelerated approval in November 2024 for previously treated, unresectable or metastatic HER2-positive biliary tract cancer, highlighting the platform’s broader relevance across HER2-driven gastrointestinal malignancies.
Rationale for Combining HER2 Blockade and Immunotherapy
The HERIZON-GEA-01 trial also explored synergy between dual HER2 targeting and immune checkpoint inhibition. Tislelizumab (TEVIMBRA®), a humanized IgG4 anti-PD-1 monoclonal antibody, is engineered to minimize Fc-gamma receptor binding on macrophages, potentially reducing antibody-dependent clearance of activated T cells. Tislelizumab received FDA approval in March 2024 for previously treated metastatic esophageal Squamous Cell Carcinoma, supporting its activity in upper gastrointestinal cancers.
HERIZON-GEA-01: Trial Design and Patient Population
HERIZON-GEA-01 (NCT05152147) is a global, open-label, Phase III study evaluating Zanidatamab-based regimens versus standard Trastuzumab plus chemotherapy in the first-line setting for HER2-positive metastatic GEA (GastroEsophageal Adenocarcinoma).
A total of 914 patients with unresectable, locally advanced, recurrent, or metastatic disease were enrolled between December 2021 and February 2025. More than two-thirds had gastric primaries. Patients had received no prior systemic therapy, HER2-targeted therapy, or immunotherapy in this setting.
Participants were randomized 1:1:1 to:
- Arm A: Trastuzumab plus chemotherapy
- Arm B: Zanidatamab plus chemotherapy
- Arm C: Zanidatamab plus Tislelizumab plus chemotherapy
CAPOX was the chemotherapy backbone in approximately 90% of patients. Zanidatamab-based regimens in Arm B and Arm C were compared with standard Trastuzumab plus chemotherapy in Arm A. The dual Primary endpoints were PFS by Blinded Independent Review and OS.
Efficacy Results: Clinically Meaningful and Practice-Changing
At the interim analysis (data cutoff October 2025; median follow-up 26 months), there was a clear and consistent improvement in Progression-Free Survival with Zanidatamab-based therapy compared with Trastuzumab plus chemotherapy. Median PFS reached 12.4 months with Zanidatamab plus chemotherapy and 12.4 months with Zanidatamab plus Tislelizumab and chemotherapy, compared with 8.1–8.2 months in the Trastuzumab control arm. These gains translated into a 35–37% reduction in the risk of disease progression or death, with Hazard Ratios of 0.65 for Zanidatamab plus chemotherapy and 0.63 for the triplet regimen (both P <0.0001). Importantly, the separation of the PFS curves was maintained over time, highlighting the durability of benefit. The 1-year PFS was 38.0% with Zanidatamab plus chemotherapy and 43.9% with the triplet, versus 20.9% and 38.2% respectively with Trastuzumab-based therapy. The 2-year PFS was 31.5% and 20.9%, respectively, compared with 15.6% in the Trastuzumab group. These findings mark the first time a majority of patients receiving first-line HER2-targeted therapy remain progression-free at one year, a notable advance in a disease historically characterized by early relapse.
Median OS improved from 19.2 months with Trastuzumab plus chemotherapy to 24.4 months with Zanidatamab plus chemotherapy and 26.4 months with Zanidatamab plus Tislelizumab and chemotherapy. The addition of Tislelizumab yielded a statistically significant 28% reduction in the risk of death (HR 0.72; P =0.0043). While OS data for Zanidatamab plus chemotherapy alone were not yet statistically significant at this interim analysis (HR 0.80; P =0.0564), the observed survival extension of more than five months suggests meaningful clinical activity, with further analyses planned as follow-up matures. The 2-year OS was 50.3% with Zanidatamab plus chemotherapy and 54.3% with the triplet, versus 42.2% and 43.8% respectively with Trastuzumab-based therapy. The 30-month OS was 38.8% and 43.8%, respectively, compared with 30.0% in the Trastuzumab group.
Notably, the triplet regimen is the first HER2-directed first-line strategy to achieve median Overall Survival exceeding two years in a randomized phase III trial. Further, the benefits in both PFS and OS were consistent across key subgroups, including geographic region and PD-L1 status, an especially notable finding given that checkpoint inhibitor benefit has traditionally been restricted to PD-L1–positive tumors.
Depth and Durability of Response
Zanidatamab-based regimens also produced deeper and more durable responses. Confirmed Objective Response Rates approached 70% in both Zanidatamab arms, with Complete Response rates nearing 20% when Tislelizumab was added. Median duration of response was particularly striking, exceeding 20 months with the triplet regimen and substantially longer than the 8-month duration observed with Trastuzumab plus chemotherapy.
Safety and Tolerability
The safety profiles of Zanidatamab and Tislelizumab were consistent with their known toxicities. Grade ≥3 treatment-related adverse events occurred in approximately 59% of patients receiving Zanidatamab plus chemotherapy and 72% with the addition of Tislelizumab, compared with 60% in the Trastuzumab arm.
Diarrhea was the most common toxicity across all arms, typically occurring early and resolving within several weeks. Rates of HER2-targeted therapy discontinuation due to adverse events were higher with Zanidatamab-based regimens but remained manageable, with no new safety signals identified.
Clinical Implications and Future Directions
HERIZON-GEA-01 represents a landmark study in HER2-positive gastroesophageal adenocarcinoma. It is the first phase III trial to demonstrate superiority of a novel HER2-targeted agent over Trastuzumab in the first-line metastatic setting, and the first to achieve median PFS beyond one year and median OS beyond two years in this population.
While cross-trial comparisons should be interpreted cautiously, outcomes with Zanidatamab plus Tislelizumab and chemotherapy compare favorably with historical results from KEYNOTE-811. The observation of benefit irrespective of PD-L1 status further broadens the potential impact of this strategy.
As longer follow-up matures and guideline bodies evaluate these data, Zanidatamab, particularly in combination with immunotherapy appears poised to redefine the standard of care for HER2-positive metastatic gastroesophageal adenocarcinoma, offering patients a meaningful extension of disease control and survival.
Zanidatamab + chemotherapy ± tislelizumab for first-line HER2-positive locally advanced, unresectable, or metastatic gastroesophageal adenocarcinoma: Primary analysis from HERIZON-GEA-01. Elimova E, Rha SY, Shitara K, et al. 2026 ASCO Gastrointestinal Cancers Symposium. Abstract LBA285. Presented January 8, 2026.