
The FDA on December 22, 2017 updated the product label for TASIGNA® to include information on TASIGNA® discontinuation, post-discontinuation monitoring criteria, and guidance for treatment re-initiation in patients taking TASIGNA® for Philadelphia chromosome positive (Ph+) Chronic Myeloid Leukemia (CML) who have achieved a sustained Molecular Response (MR 4.5). TASIGNA® is a product of Novartis Pharmaceuticals Corp.
Author: RR
SIKLOS® (Hydroxyurea)
The FDA on December 21, 2017 granted regular approval to SIKLOS® to reduce the frequency of painful crises and the need for blood transfusions in pediatric patients from 2 years of age and older with sickle cell anemia with recurrent moderate to severe painful crises. SIKLOS® is a product of Addmedica.
PERJETA® (Pertuzumab)
The FDA on December 20, 2017 granted regular approval to PERJETA® for use in combination with Trastuzumab and chemotherapy as adjuvant treatment of patients with HER2-positive early breast cancer at high risk of recurrence. PERJETA® is a product of Genentech, Inc.
OPDIVO® (Nivolumab)
The FDA on December 20, 2017 granted regular approval to the anti-PD1 monoclonal antibody OPDIVO® for the adjuvant treatment of patients with melanoma with involvement of lymph nodes or in patients with metastatic disease who have undergone complete resection. OPDIVO® was previously approved for the treatment of patients with unresectable or metastatic melanoma. OPDIVO® is a product of Bristol-Myers Squibb Company.
OGIVRI® (Trastuzumab-dkst)
The FDA on December 1, 2017 approved OGIVRI® as a Biosimilar to HERCEPTIN® (Trastuzumab, Genentech, Inc.) for the treatment of patients with HER2-overexpressing breast or metastatic stomach cancer (Gastric or GastroEsophageal junction adenocarcinoma). OGIVRI® is a product of Mylan N.V.
CABOMETYX® (Cabozantinib)
The FDA on December 19, 2017 granted regular approval to CABOMETYX® for treatment of patients with advanced Renal Cell Carcinoma (RCC). CABOMETYX® is a product of Exelixis, Inc.
BOSULIF® (Bosutinib)
The FDA on December 19, 2017 granted accelerated approval to BOSULIF® for treatment of patients with newly-diagnosed Chronic Phase (CP) Philadelphia chromosome positive (Ph+) Chronic Myelogenous Leukemia (CML). BOSULIF® is a product of Pfizer Inc.
Direct Oral Anticoagulant SAVAYSA® Noninferior to Subcutaneous FRAGMIN® for Cancer-Associated Venous Thromboembolism
SUMMARY: The Center for Disease Control and Prevention (CDC) estimates that approximately 1-2 per 1000 individuals develop Deep Vein Thrombosis/Pulmonary Embolism (PE) each year in the United States, resulting in 60,000-100,000 deaths. Venous ThromboEmbolism (VTE) is the third leading cause of cardiovascular mortality, after myocardial infarction and stroke.
Approximately 20% of cancer patients develop VTE and the current recommendations are treatment with parenteral Low Molecular Weight Heparin (LMWH) preparations, based on efficacy data. This however can be inconvenient and expensive, leading to premature discontinuation of treatment. Direct Oral Anticoagulant agents have been proven to be as effective as Warfarin, a Vitamin K antagonist, for the treatment of VTE, and are associated with less frequent and less severe bleeding and fewer drug interactions. However, the efficacy and safety of Direct Oral Anticoagulants for the treatment of cancer-associated VTE have not been established.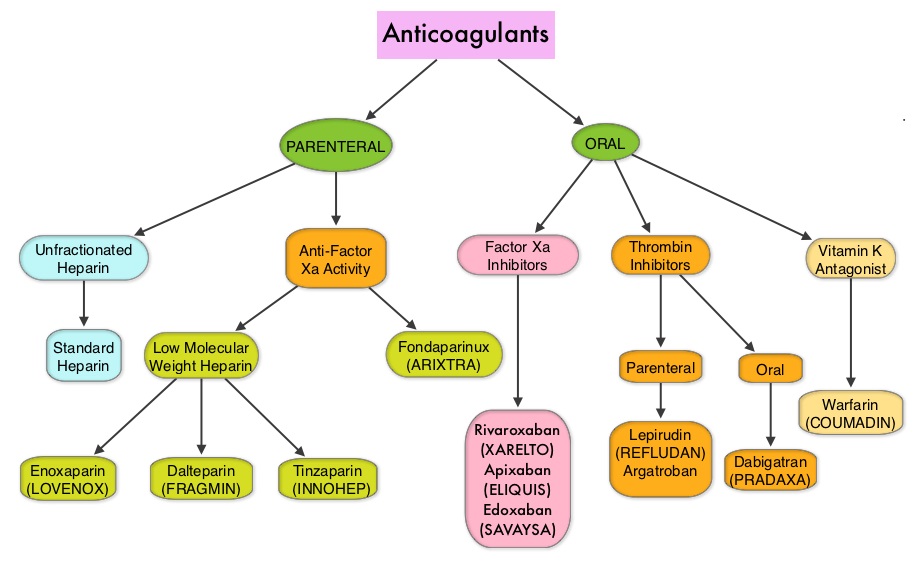
SAVAYSA® (Edoxaban) an oral Factor Xa inhibitor was compared with subcutaneous Low Molecular Weight Heparin FRAGMIN® (Dalteparin), for the treatment of patients with cancer-associated VTE in the Hokusai VTE Cancer trial. This open-label, noninferiority trial randomized 1050 patients in a 1:1 ratio to receive either SAVAYSA® or FRAGMIN®. SAVAYSA® was given after an initial course of physician’s choice of Low Molecular Weight Heparin, given subcutaneously in therapeutic doses, for at least 5 days. SAVAYSA® was administered orally at a fixed dose of 60 mg once daily. FRAGMIN® was given subcutaneously at a dose of 200 IU/kg once daily for 30 days and at a dose of 150 IU/kg once daily thereafter. This treatment was continued for up to 12 months. The median age was 64 years and 90% of the patients had solid tumors and were on various chemotherapy regimens. The primary endpoint was a composite of recurrent VTE or major bleeding during the 12 months after randomization, regardless of treatment duration.
It was noted that SAVAYSA® was noninferior to FRAGMIN® with regards to composite rates of recurrent VTE and bleeding, which occurred in 12.8% of those receiving SAVAYSA® and 13.5% of those receiving FRAGMIN®. The similarity between the two treatment groups met statistical criteria for demonstrating noninferiority for SAVAYSA® (P=0.006). The rate of recurrent VTE was numerically lower with SAVAYSA® compared with FRAGMIN® (7.9% vs 11.3%, HR=0.71; P=0.09). The rate of major bleeding was however significantly higher with SAVAYSA® compared with FRAGMIN® (6.9% vs 4.0%, HR=1.77; P=0.04). This difference was mainly due to higher rate of upper gastrointestinal bleeding with SAVAYSA® in patients with gastrointestinal cancers. The frequency of severe major bleeding (category 3 or 4) however was similar in both treatment groups.
It was concluded that Direct Oral Anticoagulant, SAVAYSA® was noninferior to subcutaneous Low Molecular Weight Heparin, FRAGMIN® with respect to the composite outcome of recurrent Venous ThromboEmbolism or major bleeding. The lower rate of recurrent VTE observed with SAVAYSA® was offset by a similar increase in the risk of major bleeding. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. Raskob GE, Van Es N, Verhamme P, et al. for the Hokusai VTE Cancer Investigators. December 12, 2017DOI: 10.1056/NEJMoa1711948
Consolidation with IMFINZI® after Chemoradiotherapy Improves Outcomes in Patients with Unresectable Stage III Non-Small Cell Lung Cancer
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2017 about 222,500 new cases of lung cancer will be diagnosed and over 155,000 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Approximately one third of all patients with NSCLC have stage III, locally advanced disease at the time of initial presentation. Worldwide, about 500,000 patients are diagnosed with unresectable, stage III NSCLC, each year. These patients include those with locally advanced primary tumors with tumor invading the vital mediastinal organs, as well as those with involvement of locoregional mediastinal lymph nodes. These patients are often treated with platinum-based doublet chemotherapy with concurrent radiation and have a median Progression Free Survival (PFS) of approximately 8 months and 5 year survival of only 15%. There is hence a significant unmet need for this patient group, with no major treatment advances thus far.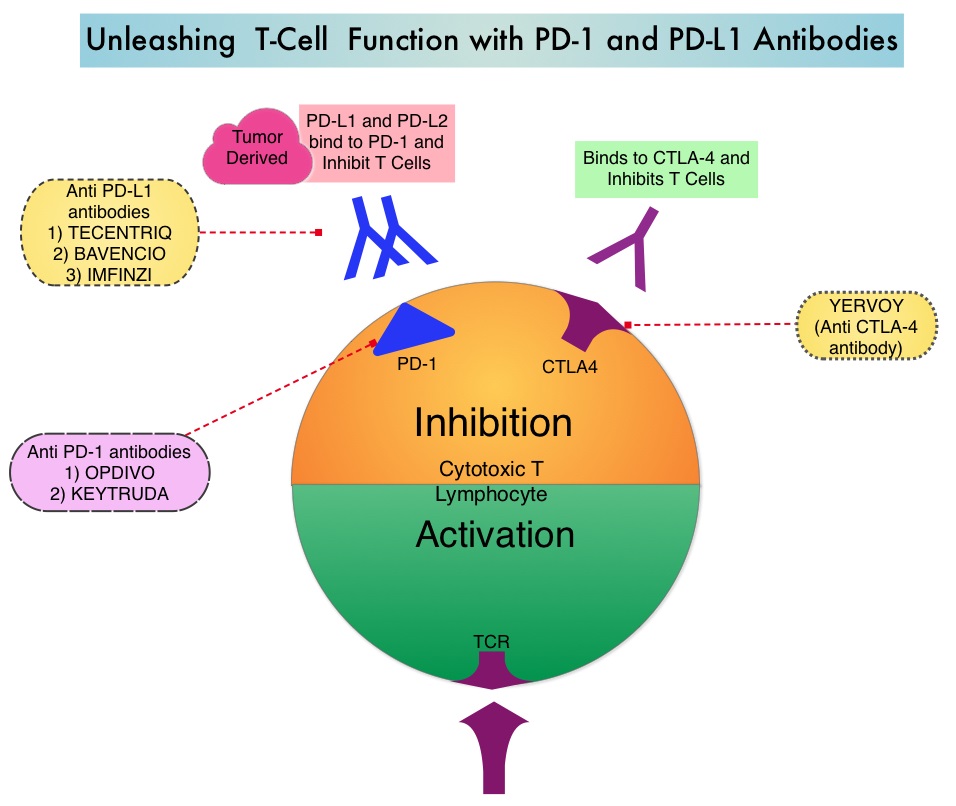
Preclinical evidence had suggested that chemotherapy and radiotherapy may upregulate PD-L1 expression in tumor cells. IMFINZI® (Durvalumab) is a selective, high-affinity, human IgG1 monoclonal antibody, that blocks the binding of Programmed Death Ligand 1 (PD-L1) to Programmed Death 1 (PD-1) and CD80, thereby unleashing the T cells to recognize and kill tumor cells. IMFINZI® showed encouraging antitumor activity in an early phase clinical study involving multiple advanced solid tumors, including stage IIIB or IV NSCLC. IMFINZI® was recently approved by the FDA for the treatment of patients with locally advanced or metastatic urothelial carcinoma, who had received prior platinum-based chemotherapy.
The authors in this publication evaluated the role of immune checkpoint blockade in locally advanced, unresectable, stage III NSCLC. PACIFIC trial is a randomized, double-blind, international, phase III study in which IMFINZI® as consolidation therapy was compared with placebo, in patients with stage III, locally advanced, unresectable NSCLC, that had not progressed following platinum-based chemoradiotherapy. Eligible patients received two or more cycles of platinum-based doublet chemotherapy concurrently with definitive radiation therapy (54-66 Gy). Following completion of concurrent chemoradiation treatment, 713 patients were randomized, of whom 709 patients in a 2:1 ratio received consolidation treatment, within 6 weeks after completion of chemoradiation with IMFINZI® 10 mg/kg every 2 weeks (N=473) or placebo (N=236), for up to 12 months. The median age was 64 years, and the majority of patients were men (70%) and 46% had a squamous histology. The coprimary end points were Progression Free Survival (PFS) and Overall Survival (OS). Secondary end points included 12-month and 18-month PFS rates, Objective Response Rate (ORR), Duration of Response, time to death or distant metastasis, and safety. The authors reported the results of a preplanned interim analysis after a median follow up of 14.5 months.
The median PFS from randomization to consolidation treatment was 16.8 months with IMFINZI® versus 5.6 months with placebo (HR=0.52; P<0.001). This meant a 48% decrease in the probability of disease progression with IMFINZI® and this improvement was consistent across all patient subgroups that were analyzed. The 12-month PFS was 55.9% vs 35.3%, and the 18-month PFS rate was 44.2% vs 27.0%, in favor of IMFINZI®. The ORR was higher with IMFINZI® compared to placebo (28.4% vs 16.0%; P<0.001), and the median Duration of Response was longer as well, with 73% of the patients in the IMFINZI® group having an ongoing response at 18 months versus 47% of the patients in the placebo group. Patients in the IMFINZI® group also had a lower incidence of new brain metastases. The median time to death or distant metastasis was longer with IMFINZI® compared with placebo (23.2 months vs 14.6 months; P<0.001). Adverse events of any grade occurred in 68% of patients in the IMFINZI® group compared to 53% in the placebo group and majority of the toxicities were grade 1 or 2, and grade 3 or higher toxicities were infrequent (less than10%), in both treatment groups. Treatment had to be discontinued due to pneumonitis in 6.3% of patients on IMFINZI® and 4.3% on placebo.
It was concluded that IMFINZI® significantly prolonged PFS in all prespecified groups of patients with locally advanced stage III NSCLC, and toxicity profile was acceptable. Biomarkers, such as mutational load or immunosignature, may be of value, as PD-L1 expression had little or no impact on outcomes. The National Comprehensive Cancer Network (NCCN) Guidelines have been updated to include one year of consolidation therapy with IMFINZI®, after curative-intent chemoradiation, for inoperable stage III lung cancer. Durvalumab after Chemoradiotherapy in Stage III Non-Small Cell Lung Cancer. Antonia SJ, Villegas A, Daniel D, et al. for the PACIFIC Investigators. N Engl J Med 2017; 377:1919-1929
FoundationOne CDx (F1CDx)
The FDA on November 30, 2017, granted marketing approval to the FoundationOne CDx, a Next Generation Sequencing (NGS) based in vitro diagnostic (IVD) to detect genetic mutations in 324 genes and two genomic signatures in any solid tumor type. The test can also identify which patients with Non-Small Cell Lung Cancer (NSCLC), melanoma, breast cancer, colorectal cancer, or ovarian cancer may benefit from 15 different FDA-approved targeted treatment options. This test is offered by Foundation Medicine, Inc.