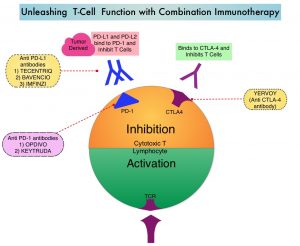
SUMMARY: The FDA on June 16, 2020 granted accelerated approval to KEYTRUDA® (Pembrolizumab) for the treatment of adult and pediatric patients with unresectable or metastatic Tumor Mutational Burden-High (10 or more mutations/megabase) solid tumors, as determined by an FDA-approved test, that have progressed following prior treatment, and who have no satisfactory alternative treatment options. The FDA on the same day also approved the FoundationOne® CDx assay (Foundation Medicine, Inc.) as a companion diagnostic for KEYTRUDA®. KEYTRUDA® is a fully humanized, Immunoglobulin G4, anti-PD-1 monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response, and unleashing the tumor-specific effector T cells.
Tumor Mutational Burden (TMB) is a measure of the somatic mutation rate within a tumor genome and is emerging as a quantitative indicator for predicting response to Immune Checkpoint Inhibitors such as KEYTRUDA®, across a wide range of malignancies. These non-synonymous somatic mutations in the tumor genome generate larger number of neo-antigens which are more immunogenic. Immune Checkpoint Inhibitors are able to unleash the immune system to detect these neoantigens and destroy the tumor. TMB can be measured using Next-Generation Sequencing (NGS) and is defined as the number of somatic, coding base substitutions and short insertions and deletions (indels), per megabase of genome examined. Several studies have incorporated Tumor Mutational Burden (TMB) as a biomarker, using the validated cutoff of TMB of 10 or more mutations/Megabase as High, and less than 10 mutations/Megabase, as Low. (A megabase is 1,000,000 DNA basepairs).
KEYNOTE-158 is a multicenter, non-randomized, open-label, Phase II basket trial investigating the antitumor activity and safety of KEYTRUDA® in multiple advanced solid tumors. The accelerated approval was based on data from a prospectively-planned, retrospective analysis of 10 cohorts of patients with various previously treated unresectable or metastatic solid tumors with TMB-H, who were enrolled in KEYNOTE-158 study. Patients received KEYTRUDA® 200 mg IV every 3 weeks until unacceptable toxicity or documented disease progression. In this study, 1,050 patients were included in the efficacy analysis and TMB was analyzed in the subset of 790 patients with sufficient tissue for testing. Of these 790 patients, 102 (13%) had tumors identified as TMB-H, defined as TMB 10 mutations /Megabase or more. The median age in this study population of 102 patients was 61 years, ECOG PS was 0-1, and 56% of patients had at least 2 prior lines of therapy. TMB status was assessed using the FoundationOne® CDx assay. Tumor response was assessed every 9 weeks for the first 12 months and every 12 weeks thereafter. The major efficacy outcome measures were Objective Response Rate (ORR) and Duration of Response (DOR) in the patients who received at least one dose of KEYTRUDA®. The key Secondary outcome measures included Progression Free Survival (PFS), Overall Survival (OS), and safety.
In the 102 patients whose tumors were TMB-H, KEYTRUDA® demonstrated an ORR of 29%, with a Complete Response rate of 4% and a Partial Response rate of 25%. After a median follow up time of 11.1 months, the median DOR had not been reached. Among the responding patients, 57% had ongoing responses of 12 months or longer, and 50% had ongoing responses of 24 months or longer. The median duration of exposure to KEYTRUDA® was 4.9 months. The most common adverse reactions for KEYTRUDA® were fatigue, decreased appetite, rash, pruritus, fever, nausea, diarrhea, cough, dyspnea, constipation, abdominal pain and musculoskeletal pain.
It was concluded that in patients with advanced solid tumors treated with KEYTRUDA® monotherapy, high TMB was associated with higher Objective Response Rates and median Duration of Response, with the Progression Free Survival favoring patients with high TMB. These data suggest that TMB may be predictive of the efficacy of KEYTRUDA® monotherapy in patients with a wide range of tumor types.
Association of tumour mutational burden with outcomes in patients with select advanced solid tumours treated with pembrolizumab in KEYNOTE-158. Marabelle A, Fakih MG, Lopez J, et al. Annals of Oncology (2019) 30 (suppl_5): v475-v532. 10.1093/annonc/mdz253.