⇚
 Advertisement
Advertisement Colon Cancer
Late Breaking Abstract - ASCO 2022: FOLFOXIRI Plus Bevacizumab in Unresectable Colorectal Cancer with Liver Metastases
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 151,030 new cases of CRC will be diagnosed in the United States in 2022 and about 52,580 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness. First line treatment of metastatic CRC include Oxaliplatin or Irinotecan, in combination with a Fluoropyrimidine and Leucovorin (FOLFOX or FOLFIRI), along with a VEGF targeting agent such as Bevacizumab. Patients with stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations. KRAS mutations are predictive of resistance to EGFR targeted therapy. Approximately 8-15% of all metastatic CRC tumors present with BRAF V600E mutations and BRAF V600E is recognized as a marker of poor prognosis in this patient group. These patients tend to have aggressive disease and do not respond as well to standard treatment intervention. Approximately 20% of the BRAF-mutated population in the metastatic setting has MSI-High tumors, but MSI-High status does not confer protection to this patient group. Colorectal cancer patients with unresectable liver-only metastases at the time of initial presentation may potentially be cured, after downsizing of metastases by neoadjuvant systemic therapy. However, the optimal neoadjuvant induction regimen has not been defined.
CAIRO5 is a prospective, randomized, multicentre, Phase III trial, conducted to investigate the optimal systemic induction therapy for patients with initially unresectable, liver-only colorectal cancer metastases. In this study, 294 patients were randomized to receive either FOLFOX or FOLFIRI plus Bevacizumab (N=148), or FOLFOXIRI plus Bevacizumab (N=146) for up to 12 cycles. Bevacizumab was given at a dose of 5 mg/kg IV. FOLFOX/FOLFIRI regimen consisted of either Oxaliplatin 85 mg/m2 IV or Irinotecan 180 mg/m2 IV, given along with Leucovorin 400 mg/m2 IV over 120 minutes, 5-Flourouracil (5-FU) 400 mg/m2 IV, followed by 5-FU 2400 mg/m2 given as an IV infusion over 46 hours. FOLFOXIRI regimen consisted of Oxaliplatin 85 mg/m2 IV, Irinotecan 165 mg/m2 IV, given along with Leucovorin 400 mg/m2 IV over 120 minutes, followed by 5-FU 3200 mg/m2 given as an IV infusion over 46 hours. Treatment was given every 2 weeks for a maximum of 12 cycles, followed by 5-FU, Leucovorin and Bevacizumab maintenance until disease progression. Enrolled patients had metastatic CRC with previously untreated liver-only metastases, (un)resectability status was prospectively assessed by a central panel consisting of radiologists and liver surgeons, according to predefined criteria, and patients were assessed for resectability every 2 months. Eligible patients had right-sided primary tumor and/or RAS or BRAF V600E mutated tumor. Both treatment groups were well balanced. The median age was 63 years, 41% had right-sided primary tumor, 86% of tumors had RAS mutation, 7% had BRAF V600E mutation, 5% had prior adjuvant chemotherapy, the median number of colorectal liver metastases was 12, and 87% had potentially resectable colorectal metastases. Patients were stratified by potentially resectable versus permanently unresectable colorectal liver metastases, BRAFV600E mutation, sidedness and choice of Irinotecan versus Oxaliplatin. The Primary endpoint was Progression Free Survival (PFS). Secondary endpoints included R0/1 resection, Overall Survival (OS), Overall Response Rate (ORR), toxicity, pathologic response and postoperative morbidity.
At a median follow up of 41 months, the median PFS was 9.0 months with doublet regimen FOLFOX/FOLFIRI plus Bevacizumab versus 10.6 months with the triplet regimen of FOLFOXIRI plus Bevacizumab. (HR=0.74; P=0.02). The ORR was 32% in the FOLFOX/FOLFIRI plus Bevacizumab group versus 52.1% in the FOLFOXIRI plus Bevacizumab group (P<0.001), R0/1 resection/ ablation rates were 37.4% versus 51.4% (P=0.02), and postoperative complications occurred in 38.2% versus 51.2% (P=0.14), respectively. Overall Survival data was immature at the time of data cutoff. Grade 3 or more adverse events, including neutropenia and diarrhea, were more common in the FOLFOXIRI plus Bevacizumab group.
It was concluded that in patients with initially unresectable colorectal cancer liver metastasis and right-sided and/or RAS or BRAF-mutated primary tumor, the triplet regimen of FOLFOXIRI plus Bevacizumab resulted in superior Progression Free Survival, a higher Objective Response Rate, and a greater chance for R0/R1 hepatic metastasectomy with or without ablation, compared to doublet chemotherapy with FOLFOX or FOLFIRI plus Bevacizumab. This benefit with the triplet regimen was achieved at the cost of increased toxicity, suggesting that careful patient selection should be made for the triplet regimen.
FOLFOXIRI + bevacizumab versus FOLFOX/FOLFIRI + bevacizumab in patients with initially unresectable colorectal liver metastases (CRLM) and right-sided and/or RAS/BRAFV600E-mutated primary tumor: Phase III CAIRO5 study of the Dutch Colorectal Cancer Group. Punt CJA, Bond MJG, Bolhuis K, et al. J Clin Oncol. 2022;40(suppl 17):LBA3506.
Late Breaking Abstract - ASCO 2022: Panitumumab Combined with mFOLFOX6 Improves Overall Survival in Left-Sided RAS Wild-Type Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 151,030 new cases of CRC will be diagnosed in the United States in 2022 and about 52,580 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness. First line treatment of metastatic CRC include Oxaliplatin or Irinotecan, in combination with a Fluoropyrimidine and Leucovorin (FOLFOX or FOLFIRI), along with a VEGF targeting agent such as Bevacizumab or EGFR targeting agents such as Cetuximab and Panitumumab. However numerous studies have failed to clearly establish that any of these combination regimens would be superior for any given patient based on clinical factors. Nonetheless, majority of patients with metastatic colorectal cancer receive FOLFOX-based first line treatment in the US.
A retrospective evaluation from the Phase III 80405 clinical trial which included data from 1,025 patients with KRAS wild-type disease, concluded that the biology of tumors originating in the right colon may be different from those originating in the left colon, with Cetuximab showing superiority over Bevacizumab, when combined with chemotherapy, in KRAS wild-type patients with left-sided colon cancer. (J Clin Oncol 34, 2016: suppl; abstr 3504).
Panitumumab (VECTIBIX®) is a human IgG2 kappa monoclonal antibody, that targets and antagonizes Epidermal Growth Factor Receptor (EGFR). The PARADIGM Trial is a multicenter, open-label, prospective, Phase III study conducted in Japan, to evaluate the efficacy and superiority of mFOLFOX6 plus Panitumumab compared to mFOLFOX6 plus Bevacizumab, in the first line treatment of chemotherapy-naïve patients with RAS wild type (KRAS/NRAS gene) metastatic colorectal cancer and left-sided primary tumors (descending colon, sigmoid colon, and rectum). In this first prospective randomized study, a total of 400 patients received Panitumumab and 402 received Bevacizumab. Both groups received mFOLFOX6. Most of the patients had left sided tumors (N=614) of whom 312 patients received Panitumumab with chemotherapy, whereas 292 patients received Bevacizumab with chemotherapy. The Primary endpoint of Overall Survival (OS) was hierarchically tested in patients with left-sided tumors, followed by evaluation in the entire study population. Key Secondary endpoints included Progression Free Survival (PFS), Objective Response Rate (ORR), and curative resection (R0) rate. Overall Survival in patients with left-sided tumors was analyzed after a median follow up of 61 months.
The study met its Primary endpoint and Panitumumab in combination with mFOLFOX6 significantly improved median Overall Survival, compared to Bevacizumab plus mFOLFOX6 in the left-sided tumor population, with a 18% lower risk of death (37.9 months versus 34.3 months; HR=0.82; P=0.031). When the data was subsequently analyzed for the entire study group, the OS benefit also significantly favored Panitumumab combination over Bevacizumab combination (median 36.2 months versus 31.3 months; HR=0.84; P=0.030). This difference however appears to be driven by the left-sided tumor population, as there was no significant OS improvement seen for patients with right-sided tumors in an exploratory analysis (median 20.2 months versus 23.2 months; HR=1.09).
There was no significant difference in the median PFS between treatment groups in the population with left-sided tumors and the median PFS was 13.7 months with Panitumumab combination and 13.2 months with Bevacizumab combination (HR=0.98). However, both Objective Response Rate and curative (R0) resection rate was higher in the Panitumumab group compared with Bevacizumab group, in the population with left-sided tumors. The Objective Response Rate was 80.2% versus 68.6%, the curative (R0) resection rate 18.3% versus 11.6% and the median duration of response was 13.1 versus 11.2 months respectively. Treatment with Panitumumab, resulted in more skin, mucosal and nail toxicities, commonly associated with EGFR inhibitors, and no new safety signal were observed.
It was concluded that in this first and largest randomized first line study comparing the efficacy of different targeted therapies in combination with standard doublet chemotherapy based on tumor sidedness, Panitumumab in combination with mFOLFOX6 significantly improved Overall Survival, resulted in a higher Objective Response Rate and a higher curative resection rate, in patients with RAS wild-type and left-sided metastatic colorectal cancer, compared with patients who received Bevacizumab plus mFOLFOX6. These findings emphasize the importance of comprehensive biomarker testing, as well as taking into consideration tumor location, in patients with metastatic colorectal cancer.
Panitumumab (PAN) plus mFOLFOX6 versus bevacizumab (BEV) plus mFOLFOX6 as first-line treatment in patients with RAS wild-type (WT) metastatic colorectal cancer (mCRC): Results from the phase 3 PARADIGM trial. Yoshino T, Watanabe J, Shitara K, et al. DOI:10.1200/JCO.2022.40.17_suppl.LBA1 Journal of Clinical Oncology 40, no. 17_suppl (June 10, 2022) LBA1.
Late Breaking Abstract – ASCO 2022: Circulating Tumor DNA in the Peripheral Blood Can Guide Adjuvant Therapy Decision in Stage II Colon Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 151,030 new cases of CRC will be diagnosed in the United States in 2022 and about 52,580 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Adjuvant chemotherapy for patients with resected, locally advanced, node-positive (Stage III) colon cancer has been the standard of care since the 1990s. Even though 80% of patients with Stage II colon cancer are cured with surgery alone, adjuvant chemotherapy is recommended for patients who have Stage II colon cancer with high-risk clinicopathological features, including tumor penetration of the serosa (T4 disease). However, the benefit of adjuvant chemotherapy for patients with Stage II disease remains unclear, with less than 5% of patients benefitting from adjuvant chemotherapy. There is therefore an unmet need for more precise markers to predict risk of recurrence after surgery for Stage II colon cancer, other than clinicopathological risk factors, and thus avoid exposure to unnecessary chemotherapy.
Circulating Tumor DNA (ctDNA) refers to DNA molecules that circulate in the bloodstream after cell apoptosis or necrosis, and can be detected in the cell-free component of peripheral blood samples (Liquid Biopsy) in almost all patients with advanced solid tumors including advanced colorectal cancer. ctDNA is a valuable biomarker and is directly evaluated for evidence of Minimal Residual Disease and allows early detection of relapse. Several studies have shown that detectable ctDNA following curative intent surgery for early stage cancers, including those with Stage II colon cancer, is associated with a very high risk of recurrence (more than 80%) without further adjuvant therapy. It has remained unclear whether adjuvant treatment is beneficial for these ctDNA-positive patients who are at high risk for recurrence.
The Circulating Tumor DNA Analysis Informing Adjuvant Chemotherapy in Stage II Colon Cancer (DYNAMIC) trial is a randomized trial designed to investigate whether a ctDNA-guided treatment approach could reduce the use of adjuvant treatment without compromising the risk of recurrence, as compared with a standard approach in patients with Stage II colon cancer. The researchers also evaluated outcomes among ctDNA-positive patients who received adjuvant chemotherapy, to assess the benefit of treating this high-risk group of patients, as well as outcomes among ctDNA-negative patients whose disease was managed by surveillance alone. In this Phase II, multicenter, randomized, controlled trial of biomarker-driven adjuvant therapy, 455 patients with resected, histologically confirmed, Stage II (T3 or T4, N0, M0) colon or rectal adenocarcinoma with negative resection margins, were randomly assigned in a 2:1 ratio to have their disease managed according to ctDNA results-ctDNA-guided management group (N=302) or managed by the treating clinician according to standard clinicopathological criteria-standard management group (N=153). Plasma specimens were obtained for ctDNA analysis from all patients at week 4 and week 7 after surgery. For patients assigned to ctDNA-guided management, week 4 and week 7 specimens were analyzed concurrently, and ctDNA results were made available to the treating clinician 8 to 10 weeks after surgery. Patients with a positive ctDNA result at either week 4 or week 7 received adjuvant single-agent fluoropyrimidine or Oxaliplatin-based chemotherapy, with the treatment regimen chosen at the treating physician’s discretion. Patients with negative ctDNA results at both week 4 and week 7 were not treated with adjuvant chemotherapy. In the standard management group, all treatment decisions were based on conventional clinicopathological criteria. This trial used a ctDNA assay specifically designed for detection of Minimal Residual Disease with very high sensitivity (a variant allele frequency limit of detection as low as 0.01%), as well as serial blood samples for ctDNA analysis to decrease the risk of a false negative result. In this study, ctDNA probes were personalized on the basis of specific mutations identified in tumor tissue.
Enrolled patients had an ECOG PS of 0-2 and had to be medically eligible to receive adjuvant Oxaliplatin-based or single-agent fluoropyrimidine chemotherapy. Patients were stratified according to tumor stage (T3 or T4) and patients with evidence of macroscopic metastatic disease on CT of the chest, abdomen, and pelvis performed within 8 weeks before enrollment, presence of synchronous primary colorectal cancer, or treatment with neoadjuvant chemoradiotherapy, were excluded. Patients were enrolled within 3 weeks following surgery, and an adequate resected tumor specimen had to be provided for mutation analysis by 4 weeks after surgery. The treatment groups were well balanced, the median age of the patients was 64 years, 85% of patients had T3 disease, 15% had T4 disease, and 5% had a lymph node yield of less than 12. Clinical high risk disease was defined as one or more of the following clinicopathological risk features: T4 lesion, poor tumor differentiation, lymph node yield less than 12, lymphovascular invasion, tumor perforation, or bowel obstruction, in association with a proficient mismatch-repair tumor, which was present in 40% of patients. The Primary efficacy end point was noninferiority of ctDNA-guided management to standard management with regards to 2-year Recurrence Free Survival (RFS). A key Secondary end point was to determine whether fewer patients would receive adjuvant chemotherapy with the ctDNA-guided approach.
At a median follow up of 37 months, the 2-year RFS was 93.5% with ctDNA-guided management and 92.4% with standard management, meeting the noninferiority criterion. Further, a lower percentage of patients in the ctDNA-guided group received adjuvant chemotherapy than in the standard-management group (15% versus 28%).
The authors concluded that a ctDNA-guided approach to the treatment of Stage II colon cancer reduced adjuvant chemotherapy use without compromising Recurrence Free Survival. Studies are underway assessing the role of escalated chemotherapy in ctDNA-positive patients and deescalation of chemotherapy in ctDNA-negative patients with Stage II colorectal cancer.
Circulating Tumor DNA Analysis Guiding Adjuvant Therapy in Stage II Colon Cancer. Tie J, Cohen JD, Lahouel K, et al. for the DYNAMIC Investigators. N Engl J Med 2022; 386:2261-2272
Lower Gastrointestinal Endoscopy before Age 50 Years Reduces Risk for Colorectal Cancer among Women
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 151,030 new cases of CRC will be diagnosed in the United States in 2022 and about 52,580 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Even though the incidence of Colorectal cancer (CRC) in the United States has been rapidly declining overall, primarily driven by screening, the incidence however has been increasing among adults younger than 50 years of age, according to data in the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) program. The increase in the incidence of CRC in young adults has been attributed to western style, high carbohydrate, high fat, low fiber diet, which can initiate inflammation and proliferation in the colonic mucosa within two weeks. Other lifestyle factors associated with CRC include obesity, high consumption of processed meat and alcohol, low levels of physical activity and cigarette smoking.
Based on benefits versus burden estimated by comparative modeling approaches using microsimulation models of CRC screening in a hypothetical cohort of 40-year-old US individuals, the American Cancer Society and the US Preventive Services Task Force within the past 4 years recommended lowering the age for screening initiation to 45 years for individuals at average risk. The recommended screening strategies include stool-based tests and endoscopic screening methods. Evidence from randomized clinical trials and prospective cohort studies has shown that endoscopic screening can reduce the incidence of and mortality from CRC, and endoscopic screening has the added advantage of CRC prevention by removal of precancerous lesions that could later become malignant, as well as detection of early-stage cancers that can be more effectively treated. There are however limited data with regards to the effectiveness of endoscopic screening in younger populations.
The authors conducted this prospective cohort study of lower gastrointestinal endoscopy (sigmoidoscopy or colonoscopy) among US female health professionals enrolled in the Nurses’ Health Study II between 1991 and 2017, to evaluate the association between endoscopy initiated at different ages and risk of CRC. The researchers also estimated the absolute risk reduction associated with endoscopy initiated at different ages through age 60 years. This analysis included 111,801 women, the median age was 36 years at the time of enrollment, and data analysis was performed from August 2020 to June 2021. The Primary end point of this study was overall CRC incidence. Secondary outcomes included incidence of younger-onset CRC (CRC diagnosed before 55 years of age) and CRC mortality.
The researchers noted that in the multivariable analysis after adjustment for age, family history, and lifestyle risk factors for CRC, compared with no endoscopy, women who underwent endoscopy had a significantly lower risk for incident colorectal cancer for age at initiation before 45 years (HR=0.37; 95% CI, 0.26-0.53), 45 to 49 years (HR=0.43; 95% CI, 0.29-0.62), 50 to 54 years (HR=0.47; 95% CI, 0.35-0.62), and 55 years or older (HR=0.46; 95% CI, 0.30-0.69).
The authors then estimated the multivariable-adjusted cumulative incidence of CRC and calculated the absolute risk reduction associated with each age group at endoscopy initiation. There was an absolute reduction in the estimated cumulative incidence of CRC through age 60 years, for women who initiated endoscopy between ages 45 to 49 years, compared with 50 to 54 years. Compared with no endoscopy, initiation of endoscopy before 50 years of age was also associated with a reduced risk of CRC diagnosed before 55 years of age (before age 45 years, HR=0.45; 95% CI, 0.29-0.70; 45-49 years, HR= 0.43, 95% CI, 0.24-0.76).
It was concluded that based on this analysis in a large, prospective cohort of women over a 26 year period, initiation of colorectal cancer screening before 50 years of age was associated with a reduced risk of CRC, and earlier initiation of endoscopy was associated with a greater absolute risk reduction of CRC, compared with initiation at later ages.
Age at Initiation of Lower Gastrointestinal Endoscopy and Colorectal Cancer Risk Among US Women. Ma W, MD, Wang M, Wang K, MD, et al. JAMA Oncol. Published online May 5, 2022. doi:10.1001/jamaoncol.2022.0883
Artificial Intelligence Can Determine Appropriate Chemotherapy Regimen in Advanced Colorectal Cancer
SUMMARY: Colorectal Cancer (CRC) is the third leading cause of cancer-related deaths in men and women in the United States. The American Cancer Society estimates that approximately 149,500 new cases of CRC will be diagnosed in the United States in 2021 and about 52,980 patients will die of the disease. The lifetime risk of developing CRC is about 1 in 23. Colorectal Cancer is a heterogeneous disease classified by its genetics, and even though the overall death rate has continued to drop, deaths from CRC among people younger than 55 years have increased 1% per year from 2008 to 2017, with 12% of CRC cases diagnosed in people under age 50. Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness.
First line treatment of metastatic CRC include Oxaliplatin or Irinotecan, in combination with a Fluoropyrimidine (FOLFOX or FOLFIRI), along with a VEGF targeting agent such as Bevacizumab or EGFR targeting agents such as Cetuximab and Panitumumab. However numerous studies have failed to clearly establish that any of these combination regimens would be superior for any given patient based on clinical factors. In the TRIBE2 Phase III study, upfront FOLFOXIRI plus Bevacizumab and reintroduction after progression resulted in significant improvement in median Overall Survival (OS), compared to mFOLFOX6 plus Bevacizumab followed by FOLFIRI plus Bevacizumab, in patients with metastatic CRC. Majority of patients with mCRC receive FOLFOX-based first-line treatment, even though neuropathy almost always limits its use beyond 4 months. Oxaliplatin has also become a first line treatment option as part of FOLFOXIRI in mCRC, as part of FOLFIRINOX in advanced Pancreatic cancer and as a part of FOLFOX for other cancers such as GE Junction and Gastric cancer. A biomarker predicting the relative efficacy of these regimens is presently lacking. However, the availability of large, combined clinical and molecular datasets has enabled the development of a machine-learning approach.
Artificial intelligence (AI) refers to the intelligence demonstrable by man-made machines and can automatically extract required information from massive amounts of data, using mathematical algorithms, and is able to mimic human cognitive abilities, thereby providing rapid solutions to difficult healthcare challenges.
The authors conducted this study to determine a patients’ likelihood of benefit from first-line treatment with FOLFOX followed by FOLFIRI versus FOLFIRI followed by FOLFOX, by taking advantage of an advanced machine-learning approach, to identify a molecular signature (FOLFOXai), predictive of treatment benefit from FOLFOX chemotherapy, by analyzing a combined dataset of comprehensive molecular profiling results and clinical outcomes data.
The researchers leveraged AI algorithms and comprehensive molecular profiling data to develop a machine-learning approach, and identified a 67-gene molecular signature (FOLFOXai), predictive of clinical benefit from FOLFOX chemotherapy, in previously untreated patients with mCRC. The molecular signature included genes involved in mediating WNT signaling (BCL9 and CDX2), epithelial-to-mesenchymal transition (EMT; INHBA, PRRX1, PBX1, and YWHAE), chromatin remodeling (EP300, ARID1A, SMARC4, and NSD3), DNA repair (WRN and BRIP1), NOTCH signaling (MAML2), and cell-cycle regulation (CNTRL and CCNE1). They then validated the putative molecular signature from a large Real World Evidence (RWE) database, a subset of cases from the randomized controlled Phase III TRIBE2 study, as well as RWE data from patients with advanced Esophageal/Gastro Esophageal Junction cancers (EC/GEJ cancers) or Pancreatic Ductal AdenoCarcinoma (PDAC) who received first-line treatments with Oxaliplatin-containing regimens.
The researchers utilized Real World Evidence (RWE) outcomes dataset from the Caris Life Sciences Precision Oncology Alliance registry, and insurance claims data from more than 10,000 physicians. The training cohort or dataset included patients who had a diagnosis of mCRC, received treatment with FOLFOX-based combination therapy, completed at least one full cycle of therapy, and completed Next-Generation DNA analysis of at least one colorectal cancer sample using a 592-gene panel. Patients were excluded if they had prior chemotherapy, including adjuvant therapy.
Two separate RWE validation cohorts were also generated, and patients in these cohorts had a diagnosis of mCRC, received first-line treatment with FOLFOX/Bevacizumab (FOLFOX/Bevacizumab cohort) or FOLFIRI-based treatment (FOLFIRI cohort), completed at least one full cycle of therapy, completed Next-Generation DNA analysis of at least one CRC sample using a 592-gene panel, and switched to an Irinotecan-containing regimen (FOLFOX/bevacizumab cohort) or to FOLFOX (FOLFIRI cohort).
For algorithm training, a TTNT (Time To Next Treatment) of 270 days was chosen to define whether a patient benefitted from receiving first-line FOLFOX. Patients with TTNT of less than 270 days were referred to as having decreased benefit to FOLFOX and others were referred to as having increased benefit. Validation studies used Time To Next Treatment (TTNT), Progression Free Survival (PFS), and Overall Survival (OS) as the Primary endpoints.
A total of 105 patients with mCRC from the RWE dataset who had received first-line FOLFOX-based treatment and who had been profiled by Caris Life Sciences, were included in the training cohort. The first validation cohort included 412 patients (with RWE data on treatments and death dates) treated with FOLFOX/Bevacizumab and 55 patients who had received FOLFIRI as first-line treatments. Additional RWE datasets included 333 patients with advanced PDAC and EC/GEJC treated in first line with Oxaliplatin-containing regimens, and blinded retrospective-prospective analysis of samples from patients enrolled in the Phase III TRIBE2 study, with completed Next Generation Sequencing (NGS) analysis.
The researchers noted that
1) A 67-gene signature was cross-validated in a training cohort (N=105) which demonstrated the ability of FOLFOXai to distinguish FOLFOX-treated patients with mCRC with increased benefit from those with decreased benefit.
2) The gene signature was predictive of TTNT and OS in an independent RWE dataset of 412 patients who had received FOLFOX/bevacizumab in first line and inversely predictive of survival in RWE data from 55 patients who had received first-line FOLFIRI.
3) Blinded analysis of TRIBE2 samples confirmed that FOLFOXai was predictive of overall survival in both Oxaliplatin-containing arms (FOLFOX HR=0.629; P=0.04 and FOLFOXIRI HR=0.483; P=0.02).
4) FOLFOXai was also predictive of benefit from Oxaliplatin-containing regimens in advanced Esophageal/Gastro Esophageal Junction cancers, as well as Pancreatic Ductal AdenoCarcinoma.
It was concluded from this analysis that application of FOLFOXai molecular signature could lead to improvements of treatment outcomes for patients with mCRC and other cancers, because patients predicted to have less benefit from Oxaliplatin-containing regimens might benefit from alternative regimens, thus providing critical guidance for the choice of first line therapy. The authors added that this is the first clinically validated, machine-learning powered molecular predictor of chemotherapy efficacy in these diseases, with immediate relevance for the initial therapeutic decision-making process.
Clinical Validation of a Machine-learning–derived Signature Predictive of Outcomes from First-line Oxaliplatin-based Chemotherapy in Advanced Colorectal Cancer. Abraham JP, Magee D, Cremolini C, et al. Clin Cancer Res 2021;27:1174-1183.
Association between Antibiotic Use and Colorectal Cancer
SUMMARY: Colorectal Cancer (CRC) is the third leading cause of cancer-related deaths in men and women in the United States. The American Cancer Society estimates that approximately 149,500 new cases of CRC will be diagnosed in the United States in 2021 and about 52,980 patients will die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Colorectal Cancer is a heterogeneous disease classified by its genetics, and even though the overall death rate has continued to drop, deaths from CRC among people younger than 55 years have increased 1% per year from 2008 to 2017, with 12% of CRC cases diagnosed in people under age 50. The proportion of the total number of patients diagnosed with CRC under the age of 50 yrs rose from 10% in 2004 to 12.2% in 2015 (P<0.0001). Younger adults presented with more advanced stage of disease (Stage III/IV) than those 50 yrs or older (51.6% versus 40.0% respectively). Based on these findings, the American Cancer Society in 2018 updated its guidelines to include a “qualified recommendation” to begin CRC screening at the age of 45 yrs. The increase in the incidence of CRC in young adults has been attributed to western style, high carbohydrate, high fat, low fiber diet, which can initiate inflammation and proliferation in the colonic mucosa within two weeks. Other lifestyle factors associated with CRC include obesity, high consumption of processed meat and alcohol, low levels of physical activity and cigarette smoking.
Preclinical studies have suggested that there is a very complex interplay of the immune system with the host’s microbiome and there may be a relationship between gut bacteria and immune response to cancer. The crosstalk between microbiota in the gut and the immune system allows for the tolerance of commensal bacteria (normal microflora) and oral food antigens and at the same time enables the immune system to recognize and attack opportunistic bacteria. Immune Checkpoint Inhibitors strongly rely on the influence of the host’s microbiome, and the gut microbial diversity enhances mucosal immunity, dendritic cell function, and antigen presentation.
There has been a significant increase in the global antibiotic consumption and colorectal cancer (CRC) rates in individuals aged less than 50 years since the late 1980s. Broad-spectrum antibiotics can potentially alter the bacterial composition and diversity of our gut microbiota, by killing the good bacteria. It has been postulated that this may influence CRC genesis in older patients and negate the benefits of immunotherapy and influence treatment outcomes. Quinolones and Sulfonamides/Trimethoprim antibiotics used to treat a wide range of infections have been associated with these right side colon cancers. It has been postulated that gut flora with more abundant Fusobacteria and Bacteroidetes may contribute to CRC development. The limited effect of Quinolones and Sulfonamides on anaerobic bacteria would therefore favor anaerobic bacteria such as Fusobacteria species and Bacteroidetes species, which may play a role in CRC development. The purpose of this analysis was to investigate antibiotics use in relation to subsequent CRC risk.
The authors conducted a matched case-control study using data from Swedish population from July 2005 to December 2016. Swedish personal Identity numbers enabled multiregister linkage and matching. The CRC cases identified using the Swedish Colorectal Cancer Register, were matched with controls from the Total Population Register. Data on antibiotics use were extracted from the Swedish Prescribed Drug Register, and other variables of interest were taken from the Swedish Inpatient Register and the Longitudinal Integration Database for Health Insurance and Labor Market Studies. All primary CRC cases were classified as proximal colon cancer (cecum, ascending colon, hepatic flexure, transverse colon, splenic flexure), distal colon cancer (descending, sigmoid colon), or rectal cancer (rectosigmoidal junction, rectum). Stages of CRC were categorized as early stage (Stage I-II) and late stage (Stage III-IV) based on TNM Classification. This nationwide, population-based study with a matched case-control design included 40,545 newly diagnosed CRC cases (67% in the colon and 33% in the rectum) and 202720 controls (for each CRC case, 5 controls were selected from the Total Population Register). Approximately 53% were men and 47% were women. Prespecified subgroup analyses (sex, age, and anatomical tumor site) were performed, and those with antibiotic use, within 2 years of CRC diagnosis were excluded. Antibiotics use reported as defined daily doses, was categorized as no use (no reported use of antibiotics during the study period), low (1-10 days), moderate (11-60 days), high (61-180 days), and very high (more than 180 days) use.
It was noted in this analysis that there was a positive dose-response association between antibiotics use and colon cancer. The CRC risk was mostly confined to proximal colon cancer for moderate use and for very high use, versus no use (P<0.001). The association between antibiotics use and risk of proximal colon cancer was more obvious among patients 50 years and older at the time of diagnosis, compared with patients younger than 50 years. There was an inverse association between antibiotics use and rectal cancer, probably reflecting differences in the bacterial flora at those two sites. When stratified by tumor stage, the positive association between antibiotics use and risk of proximal colon cancer was more pronounced in Stage I-II cancer compared with Stage III-IV cancer. In contrast, the inverse association in rectal cancer was limited to Stage III-IV. Quinolones and Sulfonamides and/or Trimethoprims were associated with increased risk of proximal colon cancer whereas Nitrofurantoins, Macrolides and/or Lincosamides, and notably, Metronidazoles and/or Tinidazoles (which exclusively inhibit anaerobic bacteria) were inversely associated with rectal cancer. Antibiotics across all classes generally had an inverse association for rectal cancer in women. There was no association noted between Methenamine hippurate, a urinary tract antiseptic not affecting the gut microbiota, and CRC risk.
It was concluded from this analysis that there was a consistent association between antibiotics use and higher subsequent risk of proximal colon cancer and an inverse association for rectal cancer in women. The authors added that these findings strengthen the evidence from previous investigations and provide new insights into site-specific carcinogenesis, as well as indirect support for the role of gut microbiota. This study provides further reasons to reduce, where possible, frequent and unnecessary antibiotic prescribing.
Antibiotics use and subsequent risk of colorectal cancer: A Swedish nationwide population-based study. Lu SSM, Mohammed Z, Haggstrom C, et al. JNCI: Journal of the National Cancer Institute, djab125, https://doi.org/10.1093/jnci/djab125
Circulating Tumor DNA as a Biomarker in Advanced Colorectal Cancer
SUMMARY: Colorectal Cancer (CRC) is the third leading cause of cancer-related deaths in men and women in the United States. The American Cancer Society estimates that approximately 149,500 new cases of CRC will be diagnosed in the United States in 2021 and about 52,980 patients will die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Cell-free DNA (cfDNA) refers to DNA molecules that circulate in the bloodstream after cell apoptosis or necrosis. A specific portion of cfDNA that originates from tumor cells is referred to as circulating tumor DNA (ctDNA), which can be detected in the cell-free component of peripheral blood samples in almost all patients with advanced solid tumors, including advanced colorectal cancer. ctDNA is a valuable biomarker and allows early detection of relapse.
Patients with metastatic colorectal cancer are often treated with chemotherapy and sometimes surgical intervention. Treatment decisions are based on clinical and pathological characteristics such as tumor size and number of metastatic lesions, which is an arbitrary method of treatment stratification. ctDNA can be a potential biomarker of tumor biology and disease trajectory, and can be an important clinical decision tool. The present study was conducted to systematically review ctDNA in Stage IV colorectal cancer, and assess its potential role as a prospective biomarker, to guide treatment decisions.
This meta-analysis included 2823 patients from 28 studies. ctDNA was detectable in 80-90% of patients with metastatic CRC prior to treatment. This analysis found a strong correlation between detectable ctDNA after treatment with surgery or chemotherapy and Overall Survival (HR=2.2; P<0.00001), as well as Progression Free Survival (HR= 3.15; P<0.00001). Further, ctDNA as an early biomarker was able to consistently predict long term prognosis in patients with unresectable disease, with changes after one cycle of systemic therapy demonstrating prognostic value. In patients with surgically resectable disease treated with curative intent, detection of ctDNA offered a lead time of 10 months, over radiological recurrence.
The authors concluded from this analysis that ctDNA is detectable in the majority of resectable and unresectable patients with metastatic colorectal cancer, and the presence of ctDNA is clearly associated with shorter Overall Survival. ctDNA may serve as an early biomarker and dynamic assessment of ctDNA may predict treatment efficacy.
Circulating tumour DNA as a biomarker in resectable and irresectable stage IV colorectal cancer; a systematic review and meta-analysis. Jones RP, Pugh SA, Graham J, et al. Eur J Cancer. 2021 Feb;144:368-381. doi: 10.1016/j.ejca.2020.11.025. Epub 2021 Jan 7.
Antibiotic Use and Early Onset Colon Cancer in Younger Individuals
SUMMARY: Colorectal Cancer (CRC) is the third leading cause of cancer-related deaths in men and women in the United States. The American Cancer Society estimates that approximately 149,500 new cases of CRC will be diagnosed in the United States in 2021 and about 52,980 patients will die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Colorectal Cancer is a heterogeneous disease classified by its genetics, and even though the overall death rate has continued to drop, deaths from CRC among people younger than 55 years have increased 1% per year from 2008 to 2017, with 12% of CRC cases diagnosed in people under age 50. The proportion of the total number of patients diagnosed with CRC under the age of 50 yrs rose from 10% in 2004 to 12.2% in 2015 (P<0.0001). Younger adults presented with more advanced stage of disease (Stage III/IV) than those 50 yrs or older (51.6% versus 40.0% respectively). Based on these findings, the American Cancer Society in 2018 updated its guidelines to include a “qualified recommendation” to begin CRC screening at the age of 45 yrs. The increase in the incidence of CRC in young adults has been attributed to western style, high carbohydrate, high fat, low fiber diet, which can initiate inflammation and proliferation in the colonic mucosa within two weeks. Other lifestyle factors associated with CRC include obesity, high consumption of processed meat and alcohol, low levels of physical activity and cigarette smoking.
Preclinical studies have suggested that there is a very complex interplay of the immune system with the host’s microbiome and there may be a relationship between gut bacteria and immune response to cancer. The crosstalk between microbiota in the gut and the immune system allows for the tolerance of commensal bacteria (normal microflora) and oral food antigens and at the same time enables the immune system to recognize and attack opportunistic bacteria. Immune Checkpoint Inhibitors strongly rely on the influence of the host’s microbiome, and the gut microbial diversity enhances mucosal immunity, dendritic cell function, and antigen presentation.
There has been a significant increase in the global antibiotic consumption and colorectal cancer (CRC) rates in individuals aged less than 50 years since the late 1980s. Broad-spectrum antibiotics can potentially alter the bacterial composition and diversity of our gut microbiota, by killing the good bacteria. It has been postulated that this may influence CRC genesis in older patients and negate the benefits of immunotherapy and influence treatment outcomes.
The present study was conducted to investigate the association between exposure to antibiotics and risk of early onset CRC, and also evaluate antibiotic usage in older adults with CRC for comparison. In this case-control study, the authors using a large Scottish primary care database identified 7,903 cases of CRC (5,281 colon, 2,622 rectal) diagnosed between 1999 and 2011, along with 30,418 healthy controls. Analyses were conducted separately for those 50 years or older, diagnosed with early onset CRC. Prescriptions for oral antibiotics (by drug class and by anaerobic/non-anaerobic effect) were extracted and total antibiotic exposure period determined for each matched set. Total exposure time in days was then categorized. The researchers then investigated the associations between each exposure with antibiotics and CRC by tumor location, adjusting for comorbidities.
Antibiotic use was associated with increased risk of colon cancer in both age groups, but the risk was increased by nearly 50% in patients under age 50, compared to 9% in those older than 50 years. Antibiotic use was associated with a significantly increased risk of proximal colon cancer (right colon) among the under those under age 50, but not among the older age group. Quinolones and sulfonamides/trimethoprim antibiotics used to treat a wide range of infections were associated with these right side colon cancers. The researchers noted that this study doesn't prove that antibiotics cause these cancers, only that there appears to a link.
It was concluded from the findings of this study that antibiotics may play a role in the development of colon cancer, particularly in the proximal colon, in individuals under age 50. The authors added that this is the first study to investigate antibiotic usage in early onset Colorectal Cancer and provides further reasons to reduce, where possible, frequent and unnecessary antibiotic prescribing.
Global rise in early-onset colorectal cancer: An association with antibiotic consumption? Perrott S, McDowell R, Murchie P, et al. DOI:https://doi.org/10.1016/j.annonc.2021.05.049.
AI Derived Molecular Signature Predicts First-line Oxaliplatin-Based Chemotherapy Benefit in Advanced CRC
SUMMARY: Colorectal Cancer (CRC) is the third leading cause of cancer-related deaths in men and women in the United States. The American Cancer Society estimates that approximately 149,500 new cases of CRC will be diagnosed in the United States in 2021 and about 52,980 patients will die of the disease. The lifetime risk of developing CRC is about 1 in 23. Colorectal Cancer is a heterogeneous disease classified by its genetics, and even though the overall death rate has continued to drop, deaths from CRC among people younger than 55 years have increased 1% per year from 2008 to 2017, with 12% of CRC cases diagnosed in people under age 50. Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness.
First line treatment of metastatic CRC include Oxaliplatin or Irinotecan, in combination with a Fluoropyrimidine ( FOLFOX or FOLFIRI), along with a VEGF targeting agent such as Bevacizumab or EGFR targeting agents such as Cetuximab and Panitumumab. However numerous studies have failed to clearly establish that any of these combination regimens would be superior for any given patient based on clinical factors. In the TRIBE2 Phase III study, upfront FOLFOXIRI plus Bevacizumab and reintroduction after progression resulted in significant improvement in median Overall Survival (OS), compared to mFOLFOX6 plus Bevacizumab followed by FOLFIRI plus Bevacizumab, in patients with metastatic CRC. Majority of patients with mCRC receive FOLFOX-based first-line treatment, even though neuropathy almost always limits its use beyond 4 months. Oxaliplatin has also become a first line treatment option as part of FOLFOXIRI in mCRC, as part of FOLFIRINOX in advanced Pancreatic cancer and as a part of FOLFOX for other cancers such as GE Junction and Gastric cancer. A biomarker predicting the relative efficacy of these regimens is presently lacking. However, the availability of large, combined clinical and molecular datasets has enabled the development of a machine-learning approach.
The authors conducted this study to determine a patients’ likelihood of benefit from first-line treatment with FOLFOX followed by FOLFIRI versus FOLFIRI followed by FOLFOX, by taking advantage of an advanced machine-learning approach, to identify a molecular signature (FOLFOXai), predictive of treatment benefit from FOLFOX chemotherapy, by analyzing a combined dataset of comprehensive molecular profiling results and clinical outcomes data.
The researchers leveraged AI algorithms and comprehensive molecular profiling data to develop a machine-learning approach, and identified a 67-gene molecular signature (FOLFOXai), predictive of clinical benefit from FOLFOX chemotherapy, in previously untreated patients with mCRC. The molecular signature included genes involved in mediating WNT signaling (BCL9 and CDX2), epithelial-to-mesenchymal transition (EMT; INHBA, PRRX1, PBX1, and YWHAE), chromatin remodeling (EP300, ARID1A, SMARC4, and NSD3), DNA repair (WRN and BRIP1), NOTCH signaling (MAML2), and cell-cycle regulation (CNTRL and CCNE1). They then validated the putative molecular signature from a large Real World Evidence (RWE) database, a subset of cases from the randomized controlled Phase III TRIBE2 study, as well as RWE data from patients with advanced Esophageal/Gastro Esophageal Junction cancers (EC/GEJ cancers) or Pancreatic Ductal AdenoCarcinoma (PDAC) who received first-line treatments with Oxaliplatin-containing regimens.
The researchers utilized Real World Evidence (RWE) outcomes dataset from the Caris Life Sciences Precision Oncology Alliance registry, and insurance claims data from more than 10,000 physicians. The training cohort or dataset included patients who had a diagnosis of mCRC, received treatment with FOLFOX-based combination therapy, completed at least one full cycle of therapy, and completed Next-Generation DNA analysis of at least one colorectal cancer sample using a 592-gene panel. Patients were excluded if they had prior chemotherapy, including adjuvant therapy.
Two separate RWE validation cohorts were also generated, and patients in these cohorts had a diagnosis of mCRC, received first-line treatment with FOLFOX/Bevacizumab (FOLFOX/Bevacizumab cohort) or FOLFIRI-based treatment (FOLFIRI cohort), completed at least one full cycle of therapy, completed Next-Generation DNA analysis of at least one CRC sample using a 592-gene panel, and switched to an Irinotecan-containing regimen (FOLFOX/bevacizumab cohort) or to FOLFOX (FOLFIRI cohort).
For algorithm training, a TTNT (Time To Next Treatment) of 270 days was chosen to define whether a patient benefitted from receiving first-line FOLFOX. Patients with TTNT of less than 270 days were referred to as having decreased benefit to FOLFOX and others were referred to as having increased benefit. Validation studies used Time To Next Treatment (TTNT), Progression Free Survival (PFS), and Overall Survival (OS) as the primary endpoints.
A total of 105 patients with mCRC from the RWE dataset who had received first-line FOLFOX-based treatment and who had been profiled by Caris Life Sciences, were included in the training cohort. The first validation cohort included 412 patients (with RWE data on treatments and death dates) treated with FOLFOX/Bevacizumab and 55 patients who had received FOLFIRI as first-line treatments. Additional RWE datasets included 333 patients with advanced PDAC and EC/GEJC treated in first line with Oxaliplatin-containing regimens, and blinded retrospective-prospective analysis of samples from patients enrolled in the Phase III TRIBE2 study, with completed Next Generation Sequencing (NGS) analysis.
The researchers noted that
1) A 67-gene signature was cross-validated in a training cohort (N=105) which demonstrated the ability of FOLFOXai to distinguish FOLFOX-treated patients with mCRC with increased benefit from those with decreased benefit.
2) The gene signature was predictive of TTNT and OS in an independent RWE dataset of 412 patients who had received FOLFOX/bevacizumab in first line and inversely predictive of survival in RWE data from 55 patients who had received first-line FOLFIRI.
3) Blinded analysis of TRIBE2 samples confirmed that FOLFOXai was predictive of overall survival in both Oxaliplatin-containing arms (FOLFOX HR=0.629; P=0.04 and FOLFOXIRI HR=0.483; P=0.02).
4) FOLFOXai was also predictive of benefit from Oxaliplatin-containing regimens in advanced Esophageal/Gastro Esophageal Junction cancers, as well as Pancreatic Ductal AdenoCarcinoma.
It was concluded from this analysis that application of FOLFOXai molecular signature could lead to improvements of treatment outcomes for patients with mCRC and other cancers, because patients predicted to have less benefit from Oxaliplatin-containing regimens might benefit from alternative regimens, thus providing critical guidance for the choice of first line therapy. The authors added that this is the first clinically validated, machine-learning powered molecular predictor of chemotherapy efficacy in these diseases, with immediate relevance for the initial therapeutic decision-making process.
Clinical Validation of a Machine-learning–derived Signature Predictive of Outcomes from First-line Oxaliplatin-based Chemotherapy in Advanced Colorectal Cancer. Abraham JP, Magee D, Cremolini C, et al. Clin Cancer Res 2021;27:1174-1183.
FDA Approves Bispecific Antibody RYBREVANT® for Metastatic Non Small Cell Lung Cancer
SUMMARY: The FDA on May 21, 2021, granted accelerated approval to RYBREVANT® (Amivantamab-vmjw), a bispecific antibody directed against Epidermal Growth Factor (EGF) and MET receptors, for adult patients with locally advanced or metastatic Non Small Cell Lung Cancer (NSCLC) with Epidermal Growth Factor Receptor (EGFR) exon 20 insertion mutations, as detected by an FDA-approved test, whose disease has progressed on or after Platinum-based chemotherapy. FDA also approved the Guardant360® CDx (Guardant Health, Inc.) as a companion diagnostic for RYBREVANT®.
The American Cancer Society estimates that for 2021, about 235,760 new cases of lung cancer will be diagnosed and 131,880 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer.
Approximately 10-15% of Caucasian patients and 35-50% of Asian patients with Adenocarcinomas, harbor activating EGFR mutations and 90% of these mutations are either exon 19 deletions or L858R substitution mutation in exon 21. EGFR exon 20 insertion mutations are the third most common after L858R and exon 19 deletions, and occur in about 2-3% patients with NSCLC and are insensitive to EGFR Tyrosine Kinase Inhibitors (TKIs) due to an altered conformation of the kinase active site. Next-Generation sequencing provides an alternative to Polymerase Chain Reaction (PCR)-based tests, which fail to identify 50% or more of exon 20 insertion mutations. Patients with EGFR exon 20 insertion mutations have a 5 year Overall Survival (OS) of 8% in the frontline setting, compared to an OS of 19% for patients with EGFR exon 19 deletions or L858R mutations. There is therefore a clinically unmet need for this patient group, as there are no approved targeted therapies available and platinum-doublet chemotherapy remains the standard of care for these patients.
Epidermal Growth Factor Receptor (EGFR) plays an important role in regulating cell proliferation, survival and differentiation, and is overexpressed in a variety of epithelial malignancies. EGFR targeted Tyrosine Kinase Inhibitors (TKIs) such as Gefitinib, Erlotinib, Afatinib, Dacomitinib and Osimertinib target the EGFR signaling cascade. However, patients eventually will develop drug resistance due to new EGFR mutations. Another important cause of drug resistance to TKIs is due to the activation of parallel RTK (Receptor Tyrosine Kinase) pathways such as Hepatocyte Growth Factor/Mesenchymal-Epithelial Transition factor (HGF/MET) pathway, thereby bypassing EGFR TKI inhibitors.
RYBREVANT® is a fully-human bispecific antibody directed against EGFR and MET receptors. RYBREVANT® binds extracellularly and simultaneously blocks ligand-induced phosphorylation of EGFR and c-MET, inhibiting tumor growth and promoting tumor cell death. Further, RYBREVANT® downregulates receptor expression on tumor cells thus preventing drug resistance mediated by new emerging mutations of EGFR or c-MET. By binding to the extracellular domain of the receptor protein, RYBREVANT® can bypass primary and secondary TKI resistance at the active site.
The present FDA approval was based on CHRYSALIS, an ongoing multicenter, non-randomized, open label, multicohort, Phase I clinical trial (NCT02609776) which included patients with locally advanced or metastatic NSCLC with EGFR exon 20 insertion mutations. The purpose of study is to evaluate the safety, pharmacokinetics, and preliminary efficacy of RYBREVANT® as a monotherapy and in combination with Lazertinib, and to determine the recommended Phase 2 dose (RP2D) (monotherapy), recommended Phase 2 combination dose (RP2CD) (combination therapy), and to determine recommended Phase 2 Dose (RP2q3W) with combination chemotherapy (RYBREVANT® in combination with standard of care Carboplatin and Pemetrexed) in 21 day treatment cycle for participants with advanced NSCLC.
In this analysis of the Phase 1 CHRYSALIS study, researchers assessed the efficacy and safety of RYBREVANT® in patients with NSCLC and EGFR exon 20 insertion mutations, who had progressed on prior Platinum-based chemotherapy, and were treated at the recommended Phase II dose of RYBREVANT® 1050 mg (1400 mg for patients weighting 80 kg or more). The median patient age was 61 years, 51% were female, and median prior lines of therapy was one. The Primary endpoint was Overall Response Rate (ORR). Secondary endpoints included Duration of Response (DOR), Clinical Benefit Rate, Progression Free Survival (PFS) and Overall Survival (OS).
It was noted that among this post-platinum cohort of patients (N=81), at a median follow up of 9.7 months, the ORR was 40%, with 4% Complete Reponses and 36% achieving Partial Responses (PR). Responses were durable with median Duration of Response of 11.1 months, with 63 % having responses of at least six months or greater duration. The median PFS was 8.3 months and median OS was 22.8 months. The Clinical Benefit Rate (PR or more, or Stable Disease of 11 weeks or more) was 74%. The most common adverse reactions (20% or more) were rash, infusion-related reactions, paronychia, fatigue, musculoskeletal pain, stomatitis, nausea, vomiting, constipation, edema, cough and dyspnea.
The authors concluded that RYBREVANT® demonstrated robust and durable antitumor activity in patients with EGFR exon 20 insertion mutations, with a manageable safety profile.
Amivantamab in Post-platinum EGFR Exon 20 Insertion Mutant Non-small Cell Lung Cancer. Sabari JK, Shu CA, Park K, et al. Presented at: IASLC 2020 World Conference on Lung Cancer Singapore. January 28-31, 2021. Abstract OA04.04
Role of Aspirin in Colorectal Cancer Prevention and Mortality
SUMMARY: Colorectal Cancer (CRC) is the third leading cause of cancer-related deaths in men and women in the United States. The American Cancer Society estimates that approximately 149,500 new cases of CRC will be diagnosed in the United States in 2021 and about 52,980 patients will die of the disease. The lifetime risk of developing CRC is about 1 in 23. The majority of CRC cases (about 75 %) are sporadic whereas the remaining 25 % of the patients have family histories of the disease. Only 5-6 % of patients with CRC with a family history background are due to inherited mutations in major CRC genes, while the rest are the result of accumulation of both genetic mutations and epigenetic modifications of several genes. Colorectal Cancer is a heterogeneous disease classified by its genetics, and even though the overall death rate has continued to drop, deaths from CRC among people younger than 55 years have increased 1% per year from 2008 to 2017, with 12% of CRC cases diagnosed in people under age 50.
Aspirin (AcetylSalicylic Acid) has been studied as a chemopreventive agent for several decades and the temporal relationship between systemic inflammation and cancer has been a topic of ongoing investigation. The US Preventive Services Task Force (USPSTF) found adequate evidence that Aspirin use reduces the incidence of CRC in adults after 5-10 years of use, and recommends initiating low-dose Aspirin use for the primary prevention of CardioVascular Disease (CVD) and CRC, in adults aged 50-69 years, who have a 10% or greater 10-year CVD risk, are not at increased risk for bleeding, have a life expectancy of at least 10 years, and are willing to take low-dose Aspirin daily for at least 10 years.
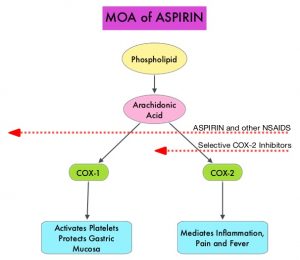
The molecular mechanisms underlying Aspirin’s chemoprevention effects as well as the dose, duration, and timing of Aspirin chemoprevention have remained unclear. More recent data suggests that platelets may play a role in tumorigenesis as well, through the release of angiogenic and growth factors due to overexpression of COX-2. Daily low dose Aspirin inhibits COX-1 and COX-2. It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties.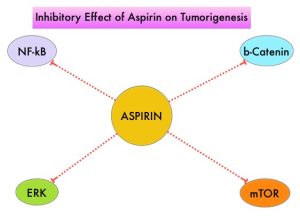
Two recently published studies have provided new information on the association between regular aspirin use, and CRC incidence.
In the first study by Zhang and colleagues, the authors addressed the use of aspirin for the primary prevention of CRC and explored the dosing, timing and duration of Aspirin intake, to reduce the incidence of CRC. The authors derived data from two large US cohort studies, The Nurses’ Health Study (January 1980-June 2014) and the Health Professionals Follow-up Study (January 1986-January 2014). These two studies provided data on the use of Aspirin by more than 94,500 participants over a period of 35 years, providing a unique opportunity to evaluate the chemopreventive benefit of Aspirin on CRC. Colorectal cancer incidence was approximately 10% lower amongst individuals reporting regular Aspirin use immediate 10 years or more earlier before follow up started, with the lowest average dose studied (23-70 mg/day) appearing as effective as higher doses. However, when the period of Aspirin use was between 5 and 10 years earlier, a smaller reduction in CRC incidence was noted amongst those taking aspirin, but the greatest reduction was noted among those taking the highest dose. This study suggested that the benefit necessitates at least 6-10 years and most clearly after approximately 10 years since initiation of Aspirin. Both remote use and use within the previous 10 years contributed independently to decreased risk, though a lower dose may be required for a benefit with longer term use.
Figueiredo and colleagues studied whether the use of Aspirin prior to or after a diagnosis of CRC, affects subsequent cancer-related mortality. They utilized data from men and women enrolled in the American Cancer Society’s Cancer Prevention Study-II (CPS-II) Nutrition Cohort who were cancer-free at the baseline (year 1992/1993), and diagnosed with CRC during follow up through 2015. They compared CRC-specific mortality amongst long-term regular Aspirin users (defined as 15 or more times per month) and non-users prior to and after diagnosis. Long-term regular use of Aspirin before diagnosis was associated with lower CRC mortality. Regular use of Aspirin following diagnosis was not statistically significantly associated with risk of CRC-specific mortality overall, although participants who began regular Aspirin use, only after their diagnosis, were at lower risk, than participants who did not use Aspirin at both the pre-and post-diagnosis periods. Further, long-term Aspirin use before diagnosis was also associated with lower risk of distant metastases. This study suggested that long-term Aspirin use before a diagnosis of non-metastatic CRC may be associated with lower CRC-specific mortality after diagnosis, implying possible inhibition of micro-metastases before diagnosis.
Taken together, the study by Zhang et al. suggested that even a relatively small dose of Aspirin taken regularly for 2-5 years during the middle years of life might reduce the risk of colorectal cancer 10 years or so later, whereas the study by Figueiredo and colleagues suggested that Aspirin, taken prior to (or started after) a diagnosis of colorectal cancer, reduced subsequent metastatic spread and cancer related mortality. Even though these two new studies support the anti-cancer effect of Aspirin, additional consistent information may be required before widespread role of Aspirin for primary prevention of cancer is embraced.
Timing of aspirin use in colorectal cancer chemoprevention: a prospective cohort study. Zhang Y, Chan AT, Meyerhardt JA, et al. J Natl Cancer Inst 2021; https://doi.org/10.1093/jnci/djab009
Associations of aspirin and non-aspirin non-steroidal anti-inflammatory drugs with colorectal cancer mortality after diagnosis. Figueiredo JC, Jacobs EJ, Newton CC, et al. J Natl Cancer Inst 2021; https://doi.org/10.1093/jnci/djab008
First Line KEYTRUDA® Superior to Chemotherapy in Metastatic MSI-H/dMMR Colorectal Cancer
SUMMARY: Colorectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 147,950 new cases of CRC were diagnosed in the United States in 2020 and about 53,200 patients died of the disease. The lifetime risk of developing CRC is about 1 in 23. The majority of CRC cases (about 75 %) are sporadic whereas the remaining 25 % of the patients have family histories of the disease. Only 5-6 % of patients with CRC with a family history background are due to inherited mutations in major CRC genes, while the rest are the result of accumulation of both genetic mutations and epigenetic modifications of several genes. Colorectal Cancer is a heterogeneous disease classified by its genetics, and even though the diagnosis of Colorectal Cancer in the US is dropping among people 65 years and older, the incidence has been rising in the younger age groups, with 12% of Colorectal Cancer cases diagnosed in people under age 50.
The DNA MisMatchRepair (MMR) system is responsible for molecular surveillance and works as an editing tool that identifies errors within the microsatellite regions of DNA and removes them. Defective MMR system leads to MSI (Micro Satellite Instability) and hypermutation, with the expression of tumor-specific neoantigens at the surface of cancer cells, triggering an enhanced antitumor immune response. MSI is therefore a hallmark of defective/deficient DNA MisMatchRepair (dMMR) system and occurs in 15% of all colorectal cancers. Defective MMR can be a sporadic or heritable event. Approximately 65% of the MSI high colon tumors are sporadic and when sporadic, the DNA MMR gene is MLH1. Defective MMR can manifest as a germline mutation occurring in MMR genes including MLH1, MSH2, MSH6 and PMS2. This produces Lynch Syndrome often called Hereditary Nonpolyposis Colorectal Carcinoma – HNPCC, an Autosomal Dominant disorder that is often associated with a high risk for Colorectal and Endometrial carcinoma, as well as several other malignancies including Ovary, Stomach, Small bowel, Hepatobiliary tract, Brain and Skin. MSI is a hallmark of Lynch Syndrome-associated cancers. MSI high tumors tend to have better outcomes and this has been attributed to the abundance of tumor infiltrating lymphocytes in these tumors from increase immunogenicity. These tumors therefore are susceptible to blockade with immune checkpoint inhibitors.
MSI testing is performed using a PCR or NGS based assay and MSI-High refers to instability at 2 or more of the 5 mononucleotide repeat markers and MSI-Low refers to instability at 1 of the 5 markers. Patients are considered Micro Satellite Stable (MSS) if no instability occurs. MSI-L and MSS are grouped together because MSI-L tumors are uncommon and behave similar to MSS tumors. Tumors considered MSI-H have deficiency of one or more of the DNA MMR genes. MMR gene deficiency can be detected by ImmunoHistoChemistry (IHC). NCCN Guidelines recommend MMR or MSI testing for all patients with a history of Colon or Rectal cancer. Unlike Colorectal and Endometrial cancer, where MSI-H/dMMR testing is routinely undertaken, the characterization of Lynch Syndrome across heterogeneous MSI-H/dMMR tumors is unknown.
KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. The FDA in 2017 granted accelerated approval to KEYTRUDA® for patients with advanced MSI-High or dMMR solid tumors, that have progressed following prior treatment, and who have no satisfactory alternative treatment options. This has led to routine MSI-H/dMMR testing in advanced solid tumors.
KEYNOTE-177 is an International, multicenter, randomized open-label, Phase III trial conducted, to evaluate the efficacy and safety of KEYTRUDA® versus Standard-of-Care (SOC) chemotherapy, as first-line therapy for dMMR or MSI-H metastatic ColoRectal Cancer (mCRC). In this study, a total of 307 patients with MSI-H/dMMR mCRC as determined locally, and with ECOG PS of 0 or 1 were randomly assigned 1:1 to first-line treatment with KEYTRUDA® 200 mg IV every 3 weeks for up to 2 years (N=153) or investigator’s choice of mFOLFOX-6 or FOLFIRI every 2 weeks, with or without Bevacizumab or Cetuximab (N=154). Chemotherapy regimens were chosen prior to randomization. Treatment was continued until disease progression, unacceptable toxicity or completion of 35 cycles (for KEYTRUDA® only). The median patient age was 63 years and both treatment groups were well balanced. The co-Primary endpoints of the study were Progression Free Survival (PFS) and Overall Survival (OS). Key Secondary endpoints included Overall Response Rate (ORR) and Safety. Patients with confirmed disease progression on chemotherapy were given the option to crossover, to receive treatment with KEYTRUDA®.
At the second interim analysis, after a median follow up of 32.4 months, it was noted that KEYTRUDA® was superior to chemotherapy with a median PFS of 16.5 months versus 8.2 months for chemotherapy (HR=0.60; P=0.00002). The estimated restricted mean survival time after 24 months of follow up was 13.7 months in the KEYTRUDA® group as compared with 10.8 months in the chemotherapy group. Progression Free Survival was consistently longer with KEYTRUDA® than with chemotherapy across prespecified subgroups. The confirmed ORR was 43.8% with KEYTRUDA® versus 33.1% with chemotherapy, with Complete Responses in 11% and 4%, respectively. Among patients with an Overall Response, 83% in the KEYTRUDA® group had ongoing responses, as compared with 35% in the chemotherapy group at 24 months. The median Duration of Response was not reached in the KEYTRUDA® group and was 10.6 months in the chemotherapy group. Following disease progression, 36% of patients assigned to the chemotherapy group crossed over to the KEYTRUDA® group. This study is being continued to evaluate OS. Grade 3-5 treatment related Adverse Event rates were 22% in the KEYTRUDA® arm and 66% in the chemotherapy group.
The authors concluded that when compared to chemotherapy, first-line therapy with KEYTRUDA® provided a clinically meaningful and statistically significant improvement in Progression Free Survival, among patients with MSI-H/dMMR metastatic colorectal cancer, with fewer treatment-related Adverse Events. The authors added that KEYTRUDA® should be the new standard of care for this patient group.
Pembrolizumab in Microsatellite-Instability–High Advanced Colorectal Cancer. Andre T, Shiu K-K, Kim TW, et al. for the KEYNOTE-177 Investigators. N Engl J Med 2020;383:2207-2218.
First Line FOLFOXIRI Plus Bevacizumab May Be a Preferable Strategy for Metastatic Colorectal Cancer
SUMMARY: Colorectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 147,950 new cases of CRC will be diagnosed in the United States in 2020 and about 53,200 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23. Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness. Patients with metastatic CRC, whose disease has progressed after treatment with standard therapies, have limited therapeutic options available, to treat their disease.
In the TRIBE trial, the triplet combination FOLFOXIRI (Fluorouracil, Leucovorin, Oxaliplatin, and Irinotecan) plus Bevacizumab significantly improved Progression Free Survival compared with the doublet combination FOLFIRI (Fluorouracil, Leucovorin and Irinotecan) plus Bevacizumab in patients with metastatic colorectal cancer. However, the actual benefit of first line treatment with three cytotoxic drugs compared with a preplanned sequential strategy of using doublet therapy, as well as the feasibility or efficacy of these therapies after disease progression has remained unclear. The authors in this study aimed to compare a preplanned strategy of upfront FOLFOXIRI followed by the reintroduction of the same regimen after disease progression versus a sequence of mFOLFOX6 and FOLFIRI doublets, in combination with Bevacizumab. It should be noted that FOLFOXIRI regimen is not FOLFIRINOX. FOLFOXIRI regimen does not require a bolus infusion of Fluorouracil, involves a different infusional dose and schedule, and includes Irinotecan and Leucovorin at lower doses than does FOLFIRINOX.
TRIBE2 is an open-label, randomized, multicenter, Phase III study in which first line FOLFOXIRI followed by reintroduction of the same regimen after disease progression, was compared with a sequence of mFOLFOX6 (Fluorouracil, Leucovorin, and Oxaliplatin) and FOLFIRI (Fluorouracil, Leucovorin, and Irinotecan) doublets, in combination with Bevacizumab, in patients with unresectable, previously untreated metastatic colorectal cancer. A total of 679 patients were randomly assigned 1:1 to the control group (N=340) or experimental group (N=339). Patients in the control group received first-line mFOLFOX6 (Oxaliplatin 85 mg/m2 IV along with Leucovorin 200 mg/m2 IV over 120 min, Fluorouracil 400 mg/m2 IV bolus, followed by Fluorouracil 2400 mg/m2 continuous infusion over 48 hours) plus Bevacizumab 5 mg/kg IV over 30 min starting on day 1. Patients in the experimental group received FOLFOXIRI (Irinotecan 165 mg/m2 IV over 60 min, Oxaliplatin 85 mg/m2 IV along with Leucovorin 200 mg/m2 IV over 120 min, Fluorouracil 3200 mg/m2 continuous infusion over 48 hours) plus Bevacizumab 5 mg/kg IV over 30 min starting on day 1. Treatment was repeated every 14 days for up to 8 cycles. Patients then received maintenance treatment with Fluorouracil and Leucovorin along with Bevacizumab every 14 days until disease progression. After disease progression on maintenance treatment, patients in the control group received FOLFIRI (Irinotecan 180 mg/m2 IV along with Leucovorin 200 mg/m2 IV over 120 min, Fluorouracil 400 mg/m2 IV bolus, followed by Fluorouracil 2400 mg/m2 continuous infusion over 48 hours) plus Bevacizumab 5 mg/kg IV over 30 min starting on day 1 every 2 weeks for 8 cycles. This was followed by Fluorouracil and Leucovorin along with Bevacizumab maintenance. After disease progression on maintenance treatment in the experimental group, FOLFOXIRI was reintroduced for up to 8 cycles, followed by Fluorouracil and Leucovorin along with Bevacizumab maintenance. Patient demographics, clinical and molecular baseline characteristics, were well balanced in both treatment groups. The Primary endpoint was Progression Free Survival 2 (PFS2), defined as the time from randomization to disease progression on any treatment given after first disease progression.
At a median follow up of 35.9 months, the median PFS2 19.2 months in the experimental group versus 16.4 months in the control group (HR=0.74; P=0.0005). The median PFS1 was 12 months versus 9.8 months respectively (HR=0.74, P=0.0002). The Objective Response Rate (ORR) to first line treatment was 62% in the experimental group versus 50% in the control group (P=0.0023). The median Overall Survival was 27.4 months in the experimental group versus 22.5 months in the control group (HR=0.82; P=0.032). The most common Grade 3 or 4 adverse events during first-line treatment in the experimental group were diarrhea and neutropenia. Serious adverse events occurred in 25% of patients in the experimental group versus 17% of patients in the control group. After first disease progression, there were no significant differences in frequency of Grade 3 or 4 adverse events between the control and experimental groups, except for a higher incidence of neurotoxicity in the experimental group (5% versus 0%).
It was concluded that first line treatment with FOLFOXIRI plus Bevacizumab followed by the reintroduction of the same regimen after disease progression is the best first-line treatment option for select group of patients with metastatic colorectal cancer, compared to sequential administration of chemotherapy doublets, in combination with Bevacizumab.
Upfront FOLFOXIRI plus bevacizumab and reintroduction after progression versus mFOLFOX6 plus bevacizumab followed by FOLFIRI plus bevacizumab in the treatment of patients with metastatic colorectal cancer (TRIBE2): a multicentre, open-label, phase 3, randomised, controlled trial. Cremolini C, Antoniotti C, Rossini D, et al. Lancet Oncol 2020;21:497-505
Late Breaking Abstract - ASCO 2020: First Line KEYTRUDA® Superior to Chemotherapy in Metastatic MSI-H/dMMR Colorectal Cancer
SUMMARY: Colorectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 147,950 new cases of CRC will be diagnosed in the United States in 2020 and about 53,200 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23. The majority of CRC cases (about 75 %) are sporadic whereas the remaining 25 % of the patients have family histories of the disease. Only 5-6 % of patients with CRC with a family history background are due to inherited mutations in major CRC genes, while the rest are the result of accumulation of both genetic mutations and epigenetic modifications of several genes.
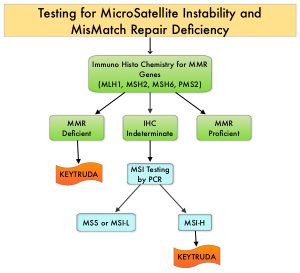
The DNA MisMatchRepair (MMR) system is responsible for molecular surveillance and works as an editing tool that identifies errors within the microsatellite regions of DNA and removes them. Defective MMR system leads to MSI (Micro Satellite Instability) and hypermutation, triggering an enhanced antitumor immune response. MSI is therefore a hallmark of defective/deficient DNA MisMatchRepair (dMMR) system and occurs in 15% of all colorectal cancers. Defective MMR can be a sporadic or heritable event. Approximately 65% of the MSI colon tumors are sporadic and when sporadic, the DNA MMR gene is MLH1. Defective MMR can manifest as a germline mutation occurring in MMR genes including MLH1, MSH2, MSH6 and PMS2. This produces Lynch Syndrome often called Hereditary Nonpolyposis Colorectal Carcinoma – HNPCC, an Autosomal Dominant disorder that is often associated with a high risk for Colorectal and Endometrial carcinoma, as well as several other malignancies including Ovary, Stomach, Small bowel, Hepatobiliary tract, Brain and Skin. MSI is a hallmark of Lynch Syndrome-associated cancers. MSI tumors tend to have better outcomes and this has been attributed to the abundance of tumor infiltrating lymphocytes in these tumors from increase immunogenicity. These tumors therefore are susceptible to blockade with immune checkpoint inhibitors. MSI testing is performed using a PCR based assay and MSI-High refers to instability at 2 or more of the 5 mononucleotide repeat markers and MSI-Low refers to instability at 1 of the 5 markers. Patients are considered Micro Satellite Stable (MSS) if no instability occurs. MSI-L and MSS are grouped together because MSI-L tumors are uncommon and behave similar to MSS tumors. Tumors considered MSI-H have deficiency of one or more of the DNA MMR genes. MMR gene deficiency can be detected by ImmunoHistoChemistry (IHC). NCCN Guidelines recommend MMR or MSI testing for all patients with a history of Colon or Rectal cancer. Unlike Colorectal and Endometrial cancer, where MSI-H/dMMR testing is routinely undertaken, the characterization of Lynch Syndrome across heterogeneous MSI-H/dMMR tumors is unknown.
KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. The FDA in 2017 granted accelerated approval to KEYTRUDA® for patients with advanced MSI-High or dMMR solid tumors, that have progressed following prior treatment, and who have no satisfactory alternative treatment options. This has led to routine MSI-H/dMMR testing in advanced solid tumors.
KEYNOTE-177 is an International, multicenter, randomized open-label, Phase III trial conducted, to evaluate the efficacy and safety of KEYTRUDA® versus Standard-of-Care (SOC) chemotherapy, as first-line therapy for dMMR or MSI-H metastatic ColoRectal Cancer (mCRC). In this study, a total of 307 patients with MSI-H/dMMR mCRC as determined locally, and with ECOG PS of 0 or 1 were randomly assigned 1:1 to first-line treatment with KEYTRUDA® 200 mg IV every 3 weeks for up to 2 years (N=153) or investigator’s choice of mFOLFOX-6 or FOLFIRI every 2 weeks, with or without Bevacizumab or Cetuximab (N=154). Chemotherapy regimens were chosen prior to randomization. Treatment was continued until disease progression, unacceptable toxicity or completion of 35 cycles (for KEYTRUDA® only). The median patient age was 63 years and both treatment groups were well balanced. The co-Primary endpoints of the study were Progression Free Survival (PFS) and Overall Survival (OS). Key Secondary endpoints included Overall Response Rate (ORR) and Safety. Patients with confirmed disease progression on chemotherapy were given the option to crossover, to receive treatment with KEYTRUDA®. The median follow up was 28 months.
It was noted that KEYTRUDA® was superior to chemotherapy with a median PFS of 16.5 months versus 8.2 months for chemotherapy (HR=0.60; P=0.0002). The 12 and 24-months PFS rates were 55.3% and 48.3% with KEYTRUDA® versus 37.3% and 18.6% with chemotherapy, respectively. The confirmed ORR was 43.8% with KEYTRUDA® versus 33.1% with chemotherapy and the median Duration of Response was not reached in the KEYTRUDA® group and was 10.6 months in the chemotherapy group. Following disease progression, 36% of patients assigned to the chemotherapy group crossed over to the KEYTRUDA® group. This study is being continued to evaluate OS. Grade 3-5 treatment related Adverse Event rates were 22% in the KEYTRUDA® arm and 66% in the chemotherapy group.
The authors concluded that when compared to chemotherapy, first-line therapy with KEYTRUDA® provided a clinically meaningful and statistically significant improvement in Progression Free Survival, among patients with MSI-H/dMMR metastatic colorectal cancer, with fewer treatment-related Adverse Events. The authors added that KEYTRUDA® should be the new standard of care for this patient group.
Pembrolizumab versus chemotherapy for microsatellite instability-high/mismatch repair deficient metastatic colorectal cancer: The phase 3 KEYNOTE-177 study. Andre T, Shiu K-K, Kim TW, et al. J Clin Oncol 38: 2020 (suppl; abstr LBA4)
FDA Approves BRAFTOVI® in combination with ERBITUX® for Metastatic Colorectal Cancer
SUMMARY: The FDA on April 8, 2020, approved BRAFTOVI® (Encorafenib) in combination with ERBITUX® (Cetuximab) for the treatment of adult patients with metastatic ColoRectal Cancer (CRC) with a BRAF V600E mutation, detected by an FDA-approved test, after prior therapy. Colorectal Cancer is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 147,950 new cases of CRC will be diagnosed in the United States in 2020 and about 53,200 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Advanced colon cancer is often incurable and standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC (mCRC), whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now also clear that even among the KRAS Wild Type patient group about 15-20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Patients with stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations. KRAS mutations are predictive of resistance to EGFR targeted therapy. Approximately 8-15% of all metastatic CRC tumors present with BRAF V600E mutations and BRAF V600E is recognized as a marker of poor prognosis in this patient group. These patients tend to have aggressive disease with a higher rate of peritoneal metastasis and do not respond well to standard treatment intervention. Approximately 20% of the BRAF-mutated population in the metastatic setting has MSI-High tumors, but MSI-High status does not confer protection to this patient group.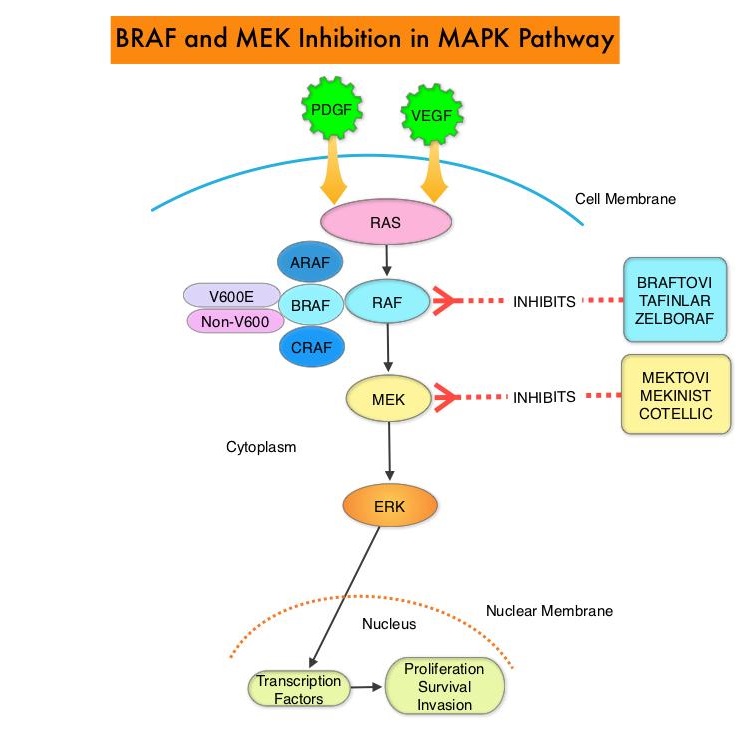
The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. The BRAF V600E mutations results in constitutive activation of the MAP kinase pathway. Inhibiting BRAF can transiently reduce MAP kinase signaling. However, this can result in feedback upregulation of EGFR signaling pathway, which can then reactivate the MAP kinase pathway. This aberrant signaling can be blocked by dual inhibition of both BRAF and EGFR. It should be noted that BRAF V600E-mutated CRC is inherently less sensitive to BRAF inhibition than Malignant Melanoma.
BRAFTOVI® (Encorafenib) is a BRAF inhibitor and has target binding characteristics that differ from other BRAF inhibitors such as ZELBORAF® (Vemurafenib) and TAFINLAR® (Dabrafenib), with a prolonged target dissociation half-life and higher potency. The combination of BRAFTOVI® along with anti-EGFR monoclonal antibody ERBITUX® (Cetuximab) showed promising activity in early-phase clinical trials.
The present FDA approval was based on BEACON CRC (Binimetinib, Encorafenib, and Cetuximab Combined to Treat BRAF-Mutant Colorectal Cancer) trial, which is an international, multicenter, randomized, open-label, Phase III study in which the efficacy and safety of BRAFTOVI® plus ERBITUX® with or without a MEK inhibitor MEKTOVI® (Binimetinib), was compared with the investigators’ choice of ERBITUX® combined with either Irinotecan or Fluorouracil, Folinic acid, and Irinotecan, in patients with BRAF V600E-mutant mCRC, whose disease has progressed after one or two prior regimens. Eligible patients were required to have BRAF V600E mutation-positive metastatic CRC (detected by the Qiagen therascreen® BRAF V600E RGQ PCR kit), with disease progression after one or two prior regimens. In this trial, 665 patients were randomly assigned in a 1:1:1 ratio to receive either triplet therapy of BRAFTOVI® 300 mg orally daily, MEKTOVI® 45 mg orally twice daily, and ERBITUX® 400 mg/m2 IV as an initial dose, then 250 mg/m2 IV weekly (N=224), doublet-therapy of BRAFTOVI® and ERBITUX® administered in the same doses and on the same schedule as the triplet regimen (N=220) or investigators’ choice of ERBITUX® combined with either Irinotecan or Fluorouracil, Folinic acid, and Irinotecan (N=221). Patients were stratified according to previous Irinotecan use and treatment was administered in 28-day cycles until disease progression. The co-Primary end points were Overall Survival (OS) in the triplet-therapy group as compared with the control group and Secondary end points included OS in the doublet-therapy group as compared with the control group, as well as Progression Free Survival, Duration of Response, and Safety in all groups. This study was not powered to compare the triplet-therapy group against the doublet-therapy group. The Overall Response Rate (ORR) and Duration of Response were assessed by blinded Independent Central Review in the subset of the first 220 patients assigned to receive either BRAFTOVI® and ERBITUX® or the control group.
The median OS was 8.4 months in the BRAFTOVI® plus ERBITUX® group, compared to 5.4 months in the control group (HR=0.60; P=0.0003), and this represented 40% reduction in the risk of death among the BRAFTOVI® plus ERBITUX® group. Median PFS was 4.2 months in the BRAFTOVI® plus ERBITUX® group compared to 1.5 months in the control group (HR=0.40; P< 0.0001). The ORR was 20% and 2% respectively. The median Duration of Response was 6.1 months for the BRAFTOVI® plus ERBITUX® group and Not Reached in the control arm. The median OS was 9.0 months in the triplet-therapy group and 5.4 months in the control group (HR for death=0.52; P<0.001). This represented 48% reduction in the risk of death in the triplet-therapy group. Both the triplet and doublet regimens reduced the risk of Quality of Life (QoL) deterioration by about 45% by different QoL assessment instruments, compared with the control regimen. The most common adverse reactions in the BRAFTOVI® plus ERBITUX® group were fatigue, nausea, diarrhea, dermatitis acneiform, abdominal pain, decreased appetite, arthralgia, and rash.
It was concluded from the BEACON CRC trial that a combination of BRAFTOVI®, MEKTOVI® and ERBITUX® as well as a combination of BRAFTOVI® plus ERBITUX® resulted in significantly longer Overall Survival and a higher Response Rate than standard therapy, in patients with metastatic Colorectal Cancer, with the BRAF V600E mutation. Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. Kopetz S, Grothey A, Yaeger R, et al. N Engl J Med 2019; 381:1632-1643
LONSURF® Plus AVASTIN® Combination for Chemo-Refractory Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 147,950 new cases of CRC will be diagnosed in the United States in 2020 and about 53,200 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23. Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness. Patients with metastatic CRC, whose disease has progressed after treatment with standard therapies, have limited therapeutic options available, to treat their disease.
LONSURF® is a combination of two agents - a novel oral nucleoside, Trifluridine and a thymidine phosphorylase inhibitor, Tipiracil hydrochloride. This combination has a unique mechanism of action. Trifluridine, the active ingredient of LONSURF® incorporates into DNA resulting in DNA damage. Degradation of Trifluridine which occurs when taken orally is prevented by Tipiracil hydrochloride. In a pivotal, global, Phase III trial (RECOURSE), LONSURF® significantly improved Overall Survival (OS) compared to placebo, with a 32% reduction in the risk of death, among patients with chemo-refractory metastatic CRC. AVASTIN® (Bevacizumab) is a humanized anti-VEGF monoclonal IgG1 antibody that directly binds Vascular Endothelial Growth Factor (VEGF) to inhibit angiogenesis.
In a previously published multicenter Phase I/II study (C-TASK FORCE), the combination of LONSURF® in combination with AVASTIN® showed promising antitumor activity with acceptable toxicity among patients with metastatic CRC. Based on the encouraging results of this study, the authors conducted an open-label, randomized, Phase II study in which the efficacy of LONSURF® plus AVASTIN® was compared with LONSURF® monotherapy in patients with refractory metastatic CRC. This study enrolled and randomly assigned 93 patients in 1:1 ratio to LONSURF® plus AVASTIN® (N=46) or LONSURF® alone (N=47). The main inclusion criteria were histopathologically confirmed metastatic CRC, refractory or intolerant to a Fluoropyrimidine (5-FU), Irinotecan (CAMPTOSAR®), Oxaliplatin (ELOXATIN®), and Cetuximab (ERBITUX®) or Panitumumab (VECTIBIX®), with the latter two agents offered only for RAS wild-type tumors. Patients had a WHO performance status of 0 or 1 and previous therapy with AVASTIN®, ZALTRAP® (Aflibercept), CYRAMZA® (Ramucirumab), or STIVARGA® (Regorafenib) was allowed. Randomized patients received LONSURF® 35 mg/m2 orally twice daily on days 1-5 and 8-12 every 28 days alone, or in combination with AVASTIN® 5 mg/kg IV on days 1 and 15 of each treatment cycle, until disease progression or unacceptable toxicity. Patients were stratified by institution and RAS mutation status. The Primary endpoint was Progression Free Survival (PFS).
After a median follow up of 10.0 months, the median PFS was 4.6 months in the LONSURF® plus AVASTIN® group versus 2.6 months in the LONSURF® monotherapy group (HR=0.45; P=0.0015). This represented a 55% reduction in the risk of progression or death. This benefit remained significant when analysis was adjusted for the stratification factors of study center and RAS mutation status (HR = 0.47, P =0.0015). The median Overall Survival was 9.4 months versus 6.7 months (HR=0.55, P =0.03) and Disease Control Rates were 67% versus 51% (P=0.14), in favor of the combination therapy. The most common treatment-related Grade 3 or more adverse events in the combination group were neutropenia and diarrhea.
It was concluded that among patients with chemo-refractory metastatic CRC, a combination of LONSURF® and AVASTIN® was associated with a significant and clinically relevant improvement in Progression Free Survival with tolerable toxicity, compared with LONSURF® monotherapy. The authors added that this could be a new treatment option and practice-changing development for patients with refractory metastatic CRC. TAS-102 with or without bevacizumab in patients with chemorefractory metastatic colorectal cancer: an investigator-initiated, open-label, randomised, phase 2 trial. Pfeiffer P, Yilmaz M, Möller S, et al. THE LANCET Oncology. Published:January 27, 2020DOI:https://doi.org/10.1016/S1470-2045(19)30827-7
Improved Quality of Life and Efficacy with BRAFTOVI®, MEKTOVI® and ERBITUX® Triplet Therapy in Patients with BRAF V600E-Mutant Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 147,950 new cases of CRC will be diagnosed in the United States in 2020 and about 53,200 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23. Advanced colon cancer is often incurable and standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab), as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC (mCRC), whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now also clear that even among the KRAS Wild Type patient group about 15-20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Patients with Stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations. KRAS mutations are predictive of resistance to EGFR targeted therapy. Approximately 5-20% of all metastatic CRC tumors present with BRAF V600E mutations and BRAF V600E is recognized as a marker of poor prognosis in this patient group. These patients tend to have aggressive disease with a higher rate of peritoneal metastasis and do not respond well to standard treatment intervention. Approximately 20% of the BRAF-mutated population in the metastatic setting has MSI-High tumors, but MSI-High status does not confer protection to this patient group.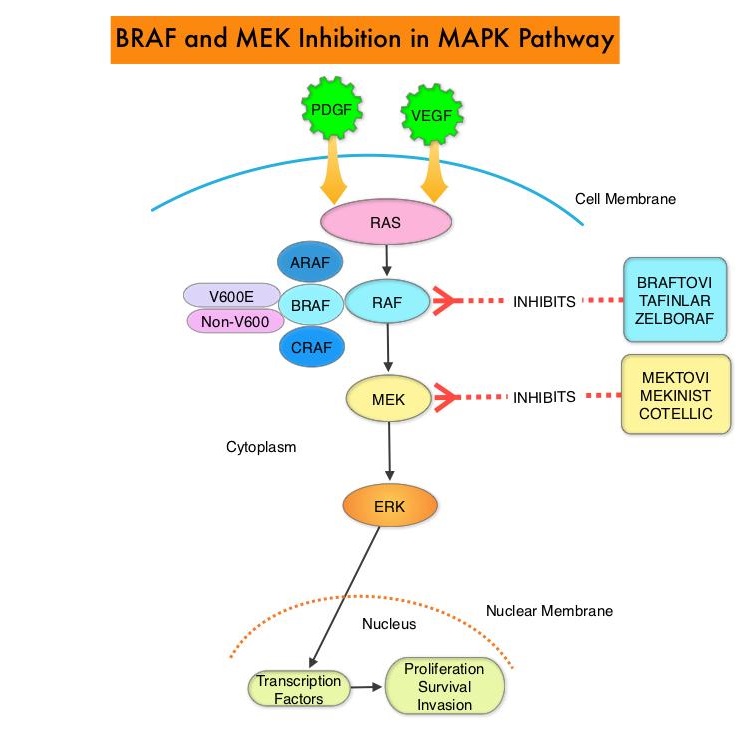
The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. The BRAF V600E mutations results in constitutive activation of the MAP kinase pathway. Inhibiting BRAF can transiently reduce MAP kinase signaling. However, this can result in feedback upregulation of EGFR signaling pathway, which can then reactivate the MAP kinase pathway. This aberrant signaling can be blocked by dual inhibition of both BRAF and EGFR. However, BRAF V600E-mutated CRC is inherently less sensitive to BRAF inhibition than melanoma. BRAFTOVI® (Encorafenib) is a BRAF inhibitor and has target binding characteristics that differ from other BRAF inhibitors such as ZELBORAF® (Vemurafenib) and TAFINLAR® (Dabrafenib), with a prolonged target dissociation half-life and higher potency. The combination of BRAFTOVI® along with anti-EGFR monoclonal antibody ERBITUX® (Cetuximab) showed promising activity in early-phase clinical trials.
The BEACON CRC (Binimetinib, Encorafenib, and Cetuximab Combined to Treat BRAF-Mutant Colorectal Cancer) trial is an international, multicenter, randomized, open-label, Phase III study in which the efficacy and safety of BRAFTOVI® plus ERBITUX® with or without a MEK inhibitor MEKTOVI® (Binimetinib), was compared with the investigators’ choice of ERBITUX® combined with either Irinotecan or Fluorouracil, Folinic acid, and Irinotecan, in patients with BRAF V600E-mutant mCRC, whose disease has progressed after one or two prior regimens. In this trial, 665 patients were randomly assigned in a 1:1:1 ratio to receive either triplet therapy of BRAFTOVI® 300 mg orally daily, MEKTOVI® 45 mg orally twice daily, and ERBITUX® 400 mg/m2 IV as an initial dose, then 250 mg/m2 IV weekly (N=224), doublet-therapy of BRAFTOVI® and ERBITUX® administered in the same doses and on the same schedule as the triplet regimen (N=220) or investigators’ choice of ERBITUX® combined with either Irinotecan or Fluorouracil, Folinic acid, and Irinotecan (N=221). Patients were stratified according to previous Irinotecan use and treatment was administered in 28-day cycles until disease progression. The co-Primary end points were Overall Survival (OS) in the triplet-therapy group as compared with the control group and Secondary end points included OS in the doublet-therapy group as compared with the control group, as well as PFS, Duration of Response, and Safety in all groups. This study was not powered to compare the triplet-therapy group against the doublet-therapy group.
At the time of prespecified interim analysis, with a median duration of follow up for survival at 7.8 months across the three groups, the median OS was 9.0 months in the triplet-therapy group and 5.4 months in the control group (HR for death=0.52; P<0.001). This represented 48% reduction in the risk of death in the triplet-therapy group. The confirmed Response Rate was 26% in the triplet-therapy group and 2% in the control group (P<0.001). The median OS in the doublet-therapy group was 8.4 months (HR for death versus control=0.60; P<0.001).
The authors in this updated analysis focused on the patient-reported Quality of Life (QOL) assessments from this study. QOL assessments using 4 validated QOL measures were secondary endpoints in the trial. They included EORTC QOL Questionnaire (QLQ C30), Functional Assessment of Cancer Therapy Colon Cancer (FACT C), EuroQol 5D 5L, and Patient Global Impression of Change (PGIC). The risk of QOL deterioration was reduced by 45% (HR=0.55) and 44% (HR=0.56), using EORTC QLQ C30 and FACT C assessments respectively, in favor of the triplet regimen over control. Similar findings were observed when the doublet-therapy regimen was compared with the regimen in the control group, and when QOL assessments were made using the other two QOL measures (EuroQol 5D 5L and PGIC). There was however no significant differences in QOL when the triplet and doublet regimen groups were compared.
It was concluded based on this updated analysis of the BEACON CRC trial, that among patients with BRAF V600E-mutant metastatic Colorectal Cancer, a combination of BRAFTOVI® plus ERBITUX® with or without a MEK inhibitor MEKTOVI®, demonstrated longer maintenance of QOL on patient-reported assessments, compared to the current standard of care. Encorafenib plus cetuximab with or without binimetinib for BRAF V600E-mutant metastatic colorectal cancer: Quality-of-life results from a randomized, three-arm, phase III study versus the choice of either irinotecan or FOLFIRI plus cetuximab (BEACON CRC). Kopetz S, Grothey A, Van Cutsem E, et al. J Clin Oncol. 2020;38(suppl 4; abstr 8).
Circulating Tumor DNA in the Peripheral Blood Predicts Recurrence Risk After Surgery and Adjuvant Chemotherapy in Stage III Colon Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 145,600 new cases of CRC were diagnosed in the United States in 2019 and about 51,020 patients died of the disease. The lifetime risk of developing CRC is about 1 in 23. Adjuvant chemotherapy for patients with resected, locally advanced, node-positive (Stage III) colon cancer has been the standard of care since the 1990s. Adjuvant treatment with an ELOXATIN® (Oxaliplatin) based chemotherapy regimen has been considered standard intervention since 2004, for patients with Stage III colon cancer, following surgical resection, and has been proven to decrease the chance of recurrent disease. Chemotherapy regimens have included (FOLFOX - Leucovorin, 5-FluoroUracil, ELOXATIN®) or CAPOX/XELOX (XELODA®/Capecitabine and ELOXATIN®), given over a period of 6 months. In spite of these advancements, defining patient subsets at high risk of recurrence following standard adjuvant therapy remains challenging and treatment failure can only be acknowledged when clinical recurrence is documented.
Cell-free DNA (cfDNA) refers to DNA molecules that circulate in the bloodstream after cell apoptosis or necrosis. A specific portion of cfDNA that originates from tumor cells is referred to as circulating tumor DNA (ctDNA), which can be detected in the cell-free component of peripheral blood samples in almost all patients with advanced solid tumors including advanced colorectal cancer. ctDNA is a valuable biomarker and allows early detection of relapse. Several studies have shown that detectable ctDNA following surgery for early stage cancers, is associated with a very high risk of recurrence. The authors in this publication report on the results of a correlative biomarker study in patients with Stage III colon cancer, undergoing standard adjuvant chemotherapy.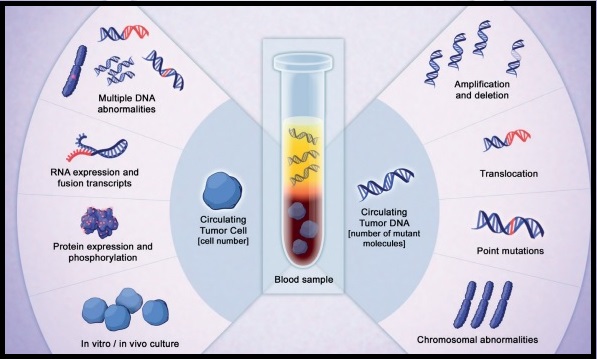
A multicenter, population-based, cohort study was conducted to determine whether serial post-surgical and post-chemotherapy ctDNA analysis could provide a real-time indication of efficacy of adjuvant therapy in Stage III colon cancer. In this study, 100 patients with newly diagnosed Stage III colon cancer who were planned to receive 24 weeks of adjuvant chemotherapy were enrolled. Patients had R0 resection with no evidence of metastatic disease on staging CT of the chest, abdomen, and pelvis before surgery. The chemotherapy regimen was chosen by the treating physician, who was blinded to the ctDNA result. High-risk patients were defined as those having pT4 and/or pN2 disease according to the pTNM staging system. Blood samples for ctDNA and CEA (CarcinoEmbryonic Antigen) analysis were collected 4-10 weeks after surgery prior to commencement of adjuvant chemotherapy and at the completion of adjuvant therapy, within 6 weeks of the final cycle of chemotherapy. All patients had a surveillance CT scan 4-8 weeks after completion of adjuvant chemotherapy. Follow up surveillance included clinical exam every 3 months along with CEA measurement and annual CT imaging for 3 years. Serial plasma samples were collected after surgery and after chemotherapy. Somatic mutations in individual patient tumors were identified by massively parallel sequencing of 15 genes commonly mutated in colorectal cancer, and personalized assays were designed to quantify ctDNA. For each patient, one mutation identified in the tumor tissue was assessed in the plasma for the presence of ctDNA. The median duration of follow up was 28.9 months and the primary aim of this study was to demonstrate the association between postsurgical and post-chemotherapy ctDNA detection and the risk of recurrence.
Among the 96 evaluable patients, circulating tumor DNA was detectable in 20 of 96 (21%) post-surgical samples and these patients had an increased risk of recurrence with associated inferior Recurrence-Free Survival, (HR=3.8; P<0.001). The estimated 3 year Recurrence Free Interval (RFI) for patients with positive ctDNA findings was 47% and for those with ctDNA-negative findings was 76%. Circulating tumor DNA was detectable in 15 of 88 (17%) post-chemotherapy samples. The estimated 3 year RFI was 30% when ctDNA was detectable after chemotherapy and 77% when ctDNA was undetectable (HR=6.8; P<0.001). Postsurgical ctDNA status was an independent predictor of disease recurrence after adjusting for known clinicopathologic risk factors (HR=7.5; P<0.001).
The authors concluded that post-surgical and post-chemotherapy circulating tumor DNA analyses is a promising prognostic marker in Stage III colon cancer, and may identify patients at high risk of recurrence, despite completing standard adjuvant treatment. This high-risk population presents a unique opportunity to explore additional therapeutic approaches. Circulating Tumor DNA Analyses as Markers of Recurrence Risk and Benefit of Adjuvant Therapy for Stage III Colon Cancer. Tie J, Cohen JD, Wang Y, et al. JAMA Oncol. 2019;5:1710-1717.
NCCN updates Colorectal Cancer Testing and Treatment Guidelines
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 145,600 new cases of CRC will be diagnosed in the United States in 2019 and about 51,020 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23. Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable with a 5-year survival rate of 11%.
The 2019 NCCN guideline update for colon cancer has expanded the scope of personalized medicine and clinical diagnostics by incorporating biomarker testing to guide treatment. With the identification of new biomarkers and expansion of biomarker testing to guide treatment among patients with colorectal cancer, studies are underway to classify colorectal cancer (CRC) based on comprehensive gene expression profiles. The Consensus Molecular Subtypes (CMS) is one of the most robust transcriptome-based classification of colorectal cancer (CRC). The CMS subtype may influence the efficacy of chemotherapy and CMS might be a new predictive factor for the efficacy of chemotherapy against mCRCs. The CRC Subtyping Consortium (CRCSC) initiated by 15 institutions analyzed more than 30 different gene expression sets across multiple platforms and sample preparation methods and identified four different molecular subtypes, CMS1, CMS2, CMS3 and CMS4. This covers approximately 87% of all CRC cases, thus leaving approximately 13% of cases molecularly uncharacterized.
CMS1: Approximately 14 percent of all CRC are considered CMS1, of which approximately 12 percent are sporadic (non-inherited), while the remaining patients have inherited disease (Lynch Syndrome). Tumors are located in the proximal colon, have a high BRAF V600E mutation rate and are associated with impaired DNA mismatch repair (MMR). Patients in this group tend to have a lower rate of relapse and if relapse does occur, they are associated with poor outcomes (about 9 months). The 5-year survival rate for this group is about 73%.
CMS2: This is the most common CRC subtype with approximately 39% of the CRC patients belonging to this group. Majority of the tumors are located in the left colon and tumors are characterized by the initial loss of APC, a tumor suppressor gene, followed by an activating mutation in KRAS and loss of TP53. Patients in this group have higher survival rates (35 months) after relapse. The 5-year survival rate for this group is 77%, the best among the four different CRC subtypes.
CMS3: Approximately 13 percent of CRC patients belong to this group. KRAS mutations are most frequently found in this patient group (68%) and approximately 3% of patients in this group overexpress HER2. Patients in this group have the second highest survival rates, with a 5-year survival rate of 75%.
CMS4: These tumors are characterized by MSS (MicroSatellite Stable) with frequent mutation of genes such as APC, KRAS, PIK3CA, and TP53. Patients in this group often have poor prognosis as they are diagnosed at advanced stages. They have little or no benefit from systemic adjuvant therapy and those with metastatic disease are often resistant to EGFR inhibitors, independent of KRAS mutation status. They have the worst 5-year Overall Survival (62%) of any molecular subtype.
The following are the key 2019 NCCN guideline updates
KRAS, NRAS and BRAF Mutation Testing
All patients with metastatic colorectal cancer should have tumor tissue genotyped for KRAS, NRAS and BRAF mutations individually or as a part of Next Generation Sequencing (NGS) panel
MicroSatellite Instability (MSI) or MisMatch Repair (MMR) Testing
1) The presence of BRAF V600E mutation in the setting of absence of MLH1 would preclude the diagnosis of Lynch Syndrome in a majority of cases. However, approximately 1% of cancers with BRAF V600E mutation and loss of MLH-1 are Lynch Syndrome and therefore, caution should be exercised, in excluding patients with a strong family history from germline screening in the case of BRAF V600E mutations
2) ImmunoHistoChemistry (IHC) refers to staining of tumor tissue for protein expression of the four mismatch repair MMR genes, MLH1, MSH2, MSH6, and PMS2, known to be mutated in Lynch Syndrome. A normal IHC test implies that all 4 MMR proteins are normally expressed or retained. An abnormal or positive IHC test implies loss or absence of expression of one or more of the 4 MMR proteins. When IHC is reported as positive, caution should be exercised to ensure that positive IHC refers to absence of mismatch expression and not presence of expression. Loss of expression by IHC in any of the MMR genes should then be followed up with genetic testing. Abnormal MLH1 on IHC should be followed by tumor testing for BRAF V600E mutation. The presence of BRAF V600 E mutation is consistent with sporadic cancer.
mFOLFOXIRI + EGFR
mFOLFOXIRI with EGFR inhibitor VECTIBIX® (Panitumumab) or ERBITUX® (Cetuximab) was added as a treatment option for unresectable stage IV mCRC that are left-sided and are KRAS/NRAS/BRAF wild-type.
mFOLFOX + EGFR
The combination regimen FOLFOX + VECTIBIX® or ERBITUX® was added for KRAS/NRAS/BRAF wild-type tumors.
Immunotherapy
Patients with advanced or metastatic CRC who are not appropriate candidates for intensive therapy may be offered OPDIVO® (Nivolumab) or KEYTRUDA® (Pembrolizumab), as a single agent or a combination of OPDIVO® and YERVOY® (Ipilimumab), only for tumors that are MMR deficient and MSI High (Category 2B). These same immunotherapy options are also listed in the guidelines as second and third-line options for MMR deficient and MSI High patients.
NTRK Gene Fusion
Tumors should be tested for Neurotrophic Receptor Tyrosine Kinase (NTRK) gene fusion, and VITRAKVI® (Larotrectinib) is now a second-line treatment option for patients with metastatic CRC that is NTRK gene fusion positive.
BRAF and MEK
BRAF wild-type was added as an indication for treatment, where KRAS and NRAS wild-type are noted. Combination therapies added to the guidelines as second-line options include
1) TAFINLAR® (Dabrafenib) targeting BRAF plus MEKINIST® (Trametinib) targeting MEK along with ERBITUX® or VECTIBIX® which are EGFR targeted monoclonal antibodies
2) BRAFTOVI® (Encorafenib) targeting BRAF plus MEKTOVI® (Binimetinib) targeting MEK along with ERBITUX® or VECTIBIX®.
NCCN Guidelines Updates: Management of Metastatic Colorectal Cancer. Messersmith WA. Presented at 2019 NCCN Annual Conference; March 21-23, 2019; Orlando, FL.
Duration of Oxaliplatin-Containing Adjuvant Therapy for Stage III Colon Cancer: ASCO Clinical Practice Guideline
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 145,600 new cases of CRC will be diagnosed in the United States in 2019 and about 51,020 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Adjuvant chemotherapy for patients with resected, locally advanced, node-positive (Stage III) Colon Cancer, has been the standard of care since the 1990s. Adjuvant treatment with an ELOXATIN® (Oxaliplatin) based chemotherapy regimen has been considered standard intervention since 2004, for patients with Stage III colon cancer, following surgical resection, and has been proven to decrease the chance of recurrent disease. Chemotherapy regimens have included (FOLFOX - Leucovorin, 5-FluoroUracil, ELOXATIN®) or CAPOX/XELOX (XELODA®/Capecitabine and ELOXATIN®), given over a period of 6 months. ELOXATIN® can however be associated with neuropathy which can be long lasting or permanent, depending on the duration of therapy. Additional toxicities with longer duration of chemotherapy include diarrhea, fatigue as well as more office visits.
This ASCO Clinical Practice Guideline was based on the IDEA Collaboration, which is a prospective, pre-planned pooled analysis of 6 concurrently conducted randomized phase III trials, which included 12,834 patients from 12 countries. The goal of this study was to determine if 3 months of adjuvant chemotherapy would be as effective as 6 months of therapy and would be non-inferior. Approximately, 40% of patients received CAPOX regimen and 60% received FOLFOX regimen. The Primary endpoint was Disease Free Survival (DFS).
In an exploratory subgroup analyses by risk of recurrence within the high-risk group defined in the IDEA Collaboration (T4 - tumor invades through the visceral peritoneum including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum or tumor directly invades or adheres to other adjacent organs or structures and/or N2 - metastasis in 4 or more regional lymph nodes), superior DFS was found with 6 months versus 3 months duration of ELOXATIN® based adjuvant chemotherapy. In the low-risk group however, (T1-tumor invades submucosa, T2-tumor invades muscularis propria, or T3-tumor invades through the muscularis propria into the pericolorectal tissues and N1-metastasis in 1-3 regional lymph nodes), DFS was noninferior with 3 months versus 6 months duration of adjuvant chemotherapy.
In prespecified subgroup analysis by type of ELOXATIN®-based chemotherapy, 3 months of treatment was non-inferior to 6 months for patients treated with CAPOX regimen. However, 3 months of treatment was inferior to 6 months, for patients treated with FOLFOX regimen. It has been hypothesized that the protracted delivery of a Fluoropyrimidine with CAPOX might have been more effective than the twice-monthly 5-FUinfusions with FOLFOX as an adjuvant therapy. Grade 2 or more neurotoxicity was significantly lower for patients who received 3 months of adjuvant therapy versus 6 months (P <0.0001), regardless of the treatment regimen (17% vs 48% for FOLFOX and 15% vs 45% for CAPOX/XELOX, respectively).
It was concluded from this study that a risk-based approach has to be taken when making adjuvant chemotherapy recommendations for patients with Stage III Colon Cancer, taking into consideration choice of treatment regimen and duration of therapy. In patients treated with adjuvant CAPOX/XELOX regimen, 3 months of therapy was as effective as 6 months, particularly in the low risk subgroup. In patients treated with FOLFOX, 6 months of adjuvant therapy compared to 3 months, resulted in a higher rate of Disease Free Survival, particularly in the high-risk subgroup.
Guideline Question: What is the optimal duration (3 months vs 6 months) of ELOXATIN®-based chemotherapy for patients with completely resected Stage III Colon Cancer?
Target Population: Patients with completely resected Stage III Colon Cancer. Target Audience: Medical oncologists, general surgeons, colorectal surgeons, surgical oncologists, and oncology Advanced Practice Providers who treat patients with Colon Cancer.
Methods: A multidisciplinary Expert Panel which included clinicians with expertise in colorectal surgery and medical oncology as well as a patient representative and an ASCO guidelines health research expert, was convened to develop clinical practice guideline recommendations, based on a systematic review of the medical literature from April 2004 to August 2018, for Phase III randomized clinical trials (RCTs) that included a comparison of two or more durations of treatment with FOLFOX or CAPOX chemotherapy.
Recommendations for patients with Stage III resected Colon Cancer who are being offered treatment with ELOXATIN®-based chemotherapy.
Recommendation 1: For patients with High-risk (T4 and/or N2) Stage III resected Colon Cancer, adjuvant ELOXATIN®-based chemotherapy should be offered for a duration of 6 months.
Recommendation 2: For patients with Low-risk (T1, T2, or T3 and N1) Stage III resected Colon Cancer, adjuvant ELOXATIN®-based chemotherapy may be offered for a duration of 3 months or 6 months, after a discussion with the patient of the potential benefits and risks of harm associated with the options for treatment duration.
Recommendation 3: A shared decision-making approach should be used for duration of ELOXATIN®-based chemotherapy for patients with Stage III resected Colon Cancer, taking into account a patient’s tumor characteristics, completeness of surgical resection, number of lymph nodes examined, comorbidities, functional status, performance status, values and preferences, age at diagnosis, life expectancy, potential years at risk for long-term sequelae of treatment, and including a discussion of the potential for benefit and risks of harm associated with treatment duration.
Duration of Oxaliplatin-Containing Adjuvant Therapy for Stage III Colon Cancer: ASCO Clinical Practice Guideline.Lieu C, Kennedy EB, Bergsland E, J Clin Oncol. 2019;37:1436-1447.
Dramatic Increase in ColoRectal Cancer Incidence among Young Adults
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 145,600 new cases of CRC will be diagnosed in the United States in 2019 and about 51,020 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23.
Even though the incidence of Colorectal cancer (CRC) in the United States has been rapidly declining overall, primarily driven by screening, the incidence however has been increasing among adults younger than 50 years of age, according to data in the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) program. Based on these findings, the American Cancer Society in 2018 updated its guidelines to include a “qualified recommendation” to begin CRC screening at the age of 45 yrs. The US Preventive Services Task Force (USPSTF) and other major US organizations have however not yet changed their recommendations. The increase in the incidence of CRC in young adults has been attributed to western style, high carbohydrate, high fat, low fiber diet, which can initiate inflammation and proliferation in the colonic mucosa within two weeks. Other lifestyle factors associated with CRC include obesity, high consumption of processed meat and alcohol, low levels of physical activity and cigarette smoking.
The authors in this publication performed a retrospective study examining the National Cancer Data Base (NCDB) registry to determine whether the trends seen through 2013, as published from SEER program had continued to worsen through 2015 (the most recent available data from the NCDB). The National Cancer Data Base is one of the largest cancer registries in the world and includes more than 70% of newly diagnosed cancer cases in the United States and more than 34 million historical records. The researchers also examined available demographic and socioeconomic factors to determine whether they were related to CRC in young adults and further compared clinical characteristics of CRC tumors among age groups, to determine whether younger patients had differences in clinical presentation. A total of 1,185,763 cases were included in the study of whom 130,165 patients were diagnosed at an age younger than 50 yrs and 1,055,598 patients were diagnosed at the age of 50 yrs or older. The proportion of patients diagnosed before the age of 50 yrs was chosen as the Primary endpoint, as most current guidelines recommend screening starting at an age of 50 yrs.
The proportion of the total number of patients diagnosed with CRC under the age of 50 yrs rose from 10% in 2004 to 12.2% in 2015 (P<0.0001). Younger adults presented with more advanced stage of disease (Stage III/IV) than those 50 yrs or older (51.6% versus 40.0% respectively). When racial and ethnic groups were stratified by sex, among men with a diagnosis of CRC before age 50, non‐Hispanic whites showed a proportional increase in diagnosis (P<0.0001), whereas among women, both Hispanic whites (P<0.05) and non‐Hispanic whites (P<0.001) had increases in the proportion of CRC diagnosed before age 50. The rates of CRC diagnosis in young adults increased over time, regardless of income level (P<0.001).The highest proportion of young adult CRC diagnoses occurred in the highest income group. The proportion of CRC cases diagnosed in younger individuals rose in urban areas (P<0.001), but not in rural areas.
It was concluded that based on this study, that the proportion of individuals diagnosed with CRC at an age younger than 50 years, has continued to increase over the past decade in the US. Younger adults also present with more advanced disease and Health Care Providers should be mindful of these data, when screening guidelines are discussed with patients. This study however does not capture oncogenic mutations or tumor laterality, which are known to affect the prognosis. The authors pointed out that the National Cancer Data Base which provided the patient information for this study currently captures laterality only for paired organs. Recent trends in the age at diagnosis of colorectal cancer in the US National Cancer Data Base, 2004‐2015. Virostko J, Capasso A, Yankeelov TE, et al. First published: 22 July 2019. https://doi.org/10.1002/cncr.32347
BRAFTOVI®, MEKTOVI® and ERBITUX® Triplet Therapy for Patients with BRAF V600E-Mutant Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 145,600 new cases of CRC will be diagnosed in the United States in 2019 and about 51,020 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 23. Advanced colon cancer is often incurable and standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC (mCRC), whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now also clear that even among the KRAS Wild Type patient group about 15-20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Patients with stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations. KRAS mutations are predictive of resistance to EGFR targeted therapy. Approximately 8-15% of all metastatic CRC tumors present with BRAF V600E mutations and BRAF V600E is recognized as a marker of poor prognosis in this patient group. These patients tend to have aggressive disease with a higher rate of peritoneal metastasis and do not respond well to standard treatment intervention. Approximately 20% of the BRAF-mutated population in the metastatic setting has MSI-High tumors, but MSI-High status does not confer protection to this patient group.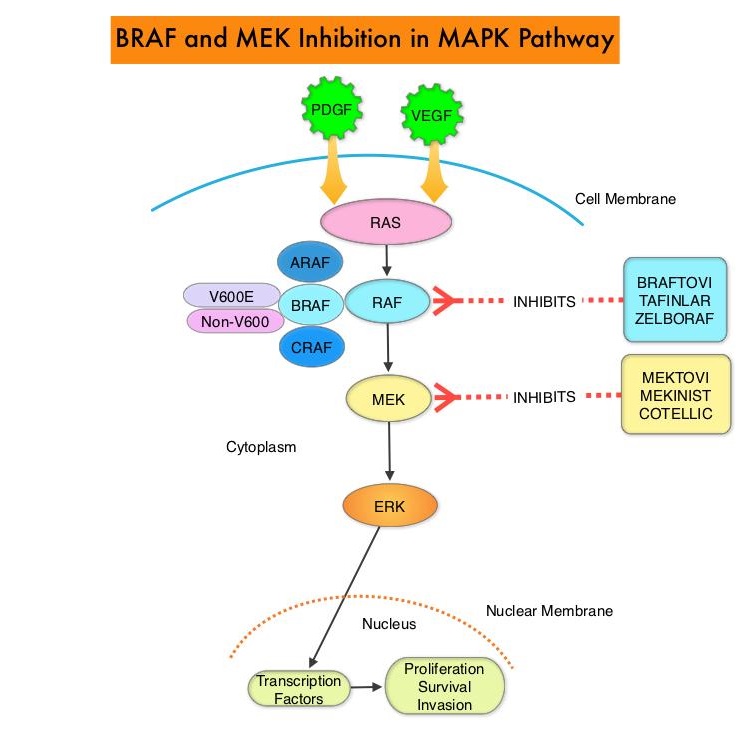
The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. The BRAF V600E mutations results in constitutive activation of the MAP kinase pathway. Inhibiting BRAF can transiently reduce MAP kinase signaling. However, this can result in feedback upregulation of EGFR signaling pathway, which can then reactivate the MAP kinase pathway. This aberrant signaling can be blocked by dual inhibition of both BRAF and EGFR. However, BRAF V600E-mutated CRC is inherently less sensitive to BRAF inhibition than melanoma.
The FDA approved BRAFTOVI® (Encorafenib) and MEKTOVI® (Binimetinib) in combination for the first-line treatment of patients with BRAF V600-mutant melanoma, in June 2018. In a recent Phase II study among previously treated patients with BRAF V600E-mutant mCRC, treatment with a combination of BRAFTOVI® plus ERBITUX® resulted in an Objective Response Rate (ORR) of 24%, PFS of 4.2 months, and OS of 9.3 months. These results were significantly better than the standard of care, as well as other BRAF, MEK, and EGFR-inhibitor triplet combinations. Preclinical data suggests that BRAFTOVI® has target binding characteristics that differ from other BRAF inhibitors such as ZELBORAF® (Vemurafenib) and TAFINLAR® (Dabrafenib), with a prolonged target dissociation half-life and higher potency. This may explain the superior efficacy of BRAFTOVI® over other BRAF inhibitors in BRAF V600E-mutated CRC. These encouraging results with the BRAFTOVI® plus ERBITUX® doublet led to the initiation of the Phase III BEACON CRC study.
The BEACON Colorectal Cancer trial is an open-label, randomized, three-arm, Phase III study in which the efficacy and safety of BRAFTOVI® plus ERBITUX® with or without MEKTOVI® was compared with the investigators’ choice of ERBITUX® combined with either Irinotecan or Fluorouracil, Folinic acid, and Irinotecan, in patients with BRAF V600E-mutant mCRC whose disease has progressed after one or two prior regimens. At the time BEACON CRC was initiated, the triplet combination of MEKTOVI®, BRAFTOVI®, and ERBITUX® had not been clinically evaluated. The authors therefore conducted a Safety Lead-In (SLI) to determine the Safety, tolerability, and preliminary efficacy of this triplet combination at the same doses planned for the randomized portion of the trial.
The randomized portion of the trial was ongoing at the time of this analysis. The BEACON trial included patients with mCRC whose tumor tissue was positive for the presence of BRAF V600E mutation. Majority of the patients had right-sided disease as is characteristic of BRAF V600E-mutant mCRC, with a high frequency of nodal and peritoneal metastasis. Liver however, was the most frequent site of metastasis. Enrolled patients must have had progressive disease on one, but no more than two prior treatment regimens, in the metastatic setting. Enrolled patients received BRAFTOVI® 300 mg PO daily plus MEKTOVI® 45 mg PO BID along with ERBITUX® 400 mg/m2 IV, followed by 250 mg/m2 IV weekly every 28 days. The Safety Lead-In was initiated before the randomized portion of the BEACON trial and included 30 patients with disease characteristics and treatment schedule as described above. The Primary end point was Safety, including the incidence of dose-limiting toxicities. Efficacy end points included Overall Response Rate, Progression Free Survival, and Overall Survival.
The median follow up was 18.2 months, and the median time on study drug was 7.9 months. The confirmed Overall Response Rate was 48%, median Duration of Response was 5.5 months, median Progression Free Survival was 8.0 months, and median Overall Survival was 15.3 months. Approximately 79% of responding patients achieved a response within 2 months. The most common adverse events were nausea, diarrhea, fatigue and dermatitis. Approximately 6% of patients experienced serous retinopathy without loss of visual acuity.
It was concluded that in this Safety Lead-In, the combination regimen of BRAFTOVI®, MEKTOVI® and ERBITUX® resulted in promising results compared with available therapies, among patients with previously treated BRAF V600E-mutant mCRC, and if confirmed in the randomized portion of the trial, could become the new standard of care in this patient group. Binimetinib, Encorafenib, and Cetuximab Triplet Therapy for Patients With BRAF V600E–Mutant Metastatic Colorectal Cancer: Safety Lead-In Results From the Phase III BEACON Colorectal Cancer Study. Van Cutsem E, Huijberts S, Grothey A, et al. Journal of Clinical Oncology 2019; 37:1460-1469.
STIVARGA® Dose Optimization Improves Outcomes in Patients with Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of CRC will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%). Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable. STIVARGA® (Regorafenib), is an oral multi-kinase inhibitor and inhibits multiple kinases including VEGF1, VEGF2, VEGF3, PDGFR, FGFR involved in tumor angiogenesis and KIT, RET, RAF-1, BRAF involved in oncogenesis. STIVARGA® is approved by the FDA for the treatment of patients with metastatic CRC, who have progressed on 5FU, ELOXATIN® (Oxaliplatin), CAMPTOSAR® (Irinotecan), anti-VEGF and anti-EGFR therapies, at a dose of 160 mg orally, once daily for the first 21 days of each 28-day cycle. The approval was based on a phase III trial in which patients receiving STIVARGA® had a statistically significant improvement in the Overall Survival (OS) and Progression Free Survival (PFS), compared to placebo.
The starting dose of STIVARGA® has been an obstacle and toxicities such as Palmar-Plantar Erythrodysesthesia Syndrome (PPES) commonly occurring during the first 2 weeks, as well as fatigue and hypertension have limited its use. Various dosing schedules have been implemented into clinical practice, despite the absence of reliable supportive data. There is therefore a need to optimize the dose of STIVARGA® in patients with refractory mCRC to maintain efficacy, while improving the tolerability profile. CORRELATE study looked at the data from the real-world setting of refractory mCRC regarding the dosing of STIVARGA® and safety, whereas the ReDos study evaluated a dose-escalation strategy, starting with a lower dose of STIVARGA®.
CORRELATE is a prospective, international observational study conducted in 13 countries to evaluate the use STIVARGA® in a real-world setting, based on safety and efficacy. The primary objective of this study was to assess safety. This final analysis describes the real-world dosing of STIVARGA® in mCRC.
Of the 1037 patients included in this study, 57% started treatment at 160 mg, 30% at 120 mg, and 13% at 80 mg or less. The mean dose administered was 75% of the approved dose. The median patient age was 65 years and majority of the patients had an ECOG performance status (PS) of 0-1 (87%). Dose reductions were more frequent in the 160 versus 120 mg group and treatment modifications were most commonly due to treatment related adverse events (66%). Most treatment discontinuations (49%) were due to radiologic disease progression, whereas 19% were due to STIVARGA® related adverse events. Treatment related adverse events of any grade occurred in 95% of patients, and 80% were attributed to STIVARGA®. Median overall survival (OS) was 7.6 months and the estimated 1-year OS was 34%.
It was concluded from this real-world, observational study that the starting dose of STIVARGA® for nearly half of patients was less than 160 mg/day and the common treatment related adverse events were generally consistent with the known safety profile of STIVARGA® in mCRC. Despite the dose modifications of STIVARGA®, there was no significant impact on its efficacy in terms of the median OS and median PFS.
ReDOS is a randomized phase II study in which STIVARGA® dose-escalation strategy beginning at a lower starting dose of 80 mg daily and ending at 160 mg daily was compared with the standard dose, in patients with refractory mCRC. In this dose escalation study, patients in Arm A (N=54) received STIVARGA® 80 mg daily, with weekly dose escalation up to 160 mg daily, if no significant drug-related toxicities were experienced, where as in Arm B (N=62), patients received the standard dose of STIVARGA® 160 mg daily, for 21 days of a 28-day cycle. The median age was 61 years and both treatment groups were well balanced. The Primary endpoint was the proportion of patients who completed 2 cycles of treatment and initiated the 3rd cycle if there was no progression.
The study met its primary endpoint with 43% of patients on Arm A initiating the 3rd cycle versus only 25% of patients on Arm B (P=0.028). The median Overall Survival (OS) was improved in Arm A versus Arm B (9 months versus 5.9 months ; P=0.094). The median Progression Free Survival (PFS) was 2.5 months for Arm A and 2 months for Arm B (P=0.55). Overall grade 3 and 4 toxicities were lower on Arm A versus Arm B and multiple Quality Of Life parameters were improved in Arm A versus Arm B, at week 2 of the first cycle.
It was concluded that weekly dose escalation of STIVARGA® from 80 mg to 160 mg daily was superior to a starting dose of 160 mg daily. Based on this study, the NCCN has updated its ColoRectal Cancer (CRC) guidelines, recommending a weekly STIVARGA® dose-escalation strategy beginning at 80 mg and ending at 160 mg, for previously treated patients with metastatic ColoRectal Cancer.
Real-world dosing of regorafenib (REG) in metastatic colorectal cancer (mCRC): final results from the prospective, observational CORRELATE study. O'Connor JM, Ducreux M, Petersen LN, et al. Ann Oncol. 2018;29 (suppl_8): viii150-viii204. 10.1093/annonc/mdy281
Regorafenib dose optimization study (ReDOS): Randomized phase II trial to evaluate dosing strategies for regorafenib in refractory metastatic colorectal cancer (mCRC)-an ACCRU Network study. Bekaii-Saab TS, Ou FS, Anderson DM, et al. J Clin Oncol. 2018;36(suppl 4S; abstr 611)
BRAF V600E Mutation is a Very Poor Prognostic Factor in Metastatic Colorectal Carcinoma
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of CRC will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%). Advanced colon cancer is often incurable and standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC, whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now also clear that even among the KRAS Wild Type patients, about 15-20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Patients with stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations. KRAS mutations are predictive of resistance to Epidermal Growth Factor Receptor (EGFR) targeted therapy. Approximately 5-10% of all metastatic CRC tumors present with BRAF V600E mutations and BRAF V600E is recognized as a marker of poor prognosis in this patient group. These patients tend to have aggressive disease with a higher rate of peritoneal metastasis and do not respond well to standard treatment intervention. Approximately 25% of the BRAF-mutated population in the metastatic setting has MSI-High tumors, but MSI-High status does not confer protection to this patient group.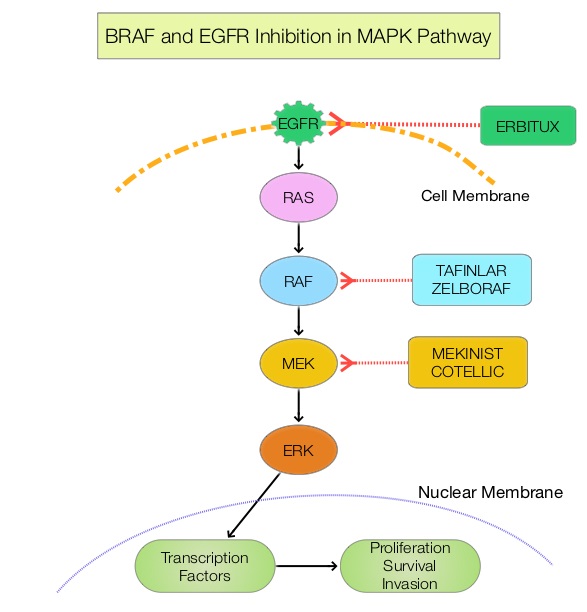
The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. The BRAF V600E mutations results in constitutive activation of the MAP kinase pathway. Inhibiting BRAF can transiently reduce MAP kinase signaling. However, this can result in feedback upregulation of EGFR signaling pathway, which can then reactivate the MAP kinase pathway. This aberrant signaling can be blocked by dual inhibition of both BRAF and EGFR.
ZELBORAF® (Vemurafenib), is a selective oral inhibitor of mutated BRAF whereas ERBITUX® is a monoclonal antibody targeting Epidermal Growth Factor Receptor (EGFR). In a phase II SWOG trial (SWOG 1406), the addition of ZELBORAF® to the combination of CAMPTOSAR® (Irinotecan) and ERBITUX® resulted in a 58% reduction in the risk of disease progression and a higher Disease Control Rate, suggesting that simultaneous EGFR and BRAF inhibition (Dual Inhibition) is effective in BRAF V600 mutated ColoRectal Cancer.
Unlike primary colorectal cancer, the association of BRAF V600E and non-V600E mutations with survival and tumor recurrence after resection of ColoRectal Liver Metastases (CRLM), has remained unclear. This present study was conducted to investigate the prognostic association of BRAF mutations with survival and recurrence independently, and to understand how BRAF mutations compared with other prognostic determinants, such as KRAS mutations. This cohort study enrolled 853 patients with colorectal tumors and liver metastases, of whom 849 patients were evaluable and included in the study analyses. All patients underwent resection of their ColoRectal Liver Metastases with a curative intent from January 1, 2000, through December 31, 2016, at institutions participating in the International Genetic Consortium for Colorectal Liver Metastasis and had available data on BRAF and KRAS mutational status. The median age was 60 years, and 60% were male. The main outcomes and measures were the association of BRAF V600E and non-V600E mutations with Disease Free Survival (DFS) and Overall Survival (OS).
Forty three patients (5.1%) had a mutated BRAF (V600E and non-V600E) /wild-type KRAS genotype, 480 patients (56.5%) had wild-type BRAF/wild-type KRAS genotype; and 326 patients (38.4%) had a wild-type BRAF/mutated KRAS genotype. Compared with the wild-type BRAF/wild-type KRAS genotype group, patients with a mutated BRAF/wild-type KRAS genotype more frequently were female (62.8% vs 35.2%) and 65 years or older (51.2% vs 36.9%), had right-sided primary tumors (62.8% vs 17.4%), and presented with a metachronous liver metastasis (64.3% vs 46.8%). The median follow up was 28.3 months.
On multivariable analysis, the presence of BRAF V600E but not non-V600E mutation was associated with significantly poor Overall Survival (HR=2.76; P<0.001) and Disease Free Survival (HR=2.04; P=0.002). Compared with KRAS mutation, the BRAF V600E mutation had a stronger association with OS and DFS than the KRAS mutations.
It was concluded that the presence of BRAF V600E mutation was associated with worse prognosis and increased risk of recurrence, and BRAF V600E mutation was not only a stronger prognostic factor than KRAS but also was the strongest prognostic determinant in the overall cohort. It remains to be seen if BRAF V600E mutated metastatic colorectal tumors would have better outcomes with targeted triplet combination therapies such as ZELBORAF® CAMPTOSAR® and ERBITUX® or TAFINLAR® (Dabrafenib-BRAF inhibitor), MEKINIST® (Trametinib-MEK inhibitor) and VECTIBIX®. Association of BRAF Mutations With Survival and Recurrence in Surgically Treated Patients With Metastatic Colorectal Liver Cancer. Margonis, GA, Buettner, S, Andreatos, N, et al. JAMA Surg. 2018;153(7):e180996. doi:10.1001/jamasurg.2018.0996
MicroRNA-31-3p Expression is a Predictive Biomarker of Anti-EGFR Efficacy in Patients with RAS Wild-type Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of CRC will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%). Advanced colon cancer is often incurable and standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC, whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now also clear that even among the KRAS Wild Type patients, about 15-20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents.
MicroRNAs (MiRNA) are small non-coding RNA molecules that play a key role in the regulation of intracellular processes through post-transcriptional regulation of gene expression. It has been shown that MicroRNAs controlling expression of oncogenes and tumor suppressor genes are frequently deregulated in cancer cells. One MiRNA which is frequently deregulated in a variety of cancers is MiR-31, which is frequently overexpressed in colorectal cancer, with high expression correlating with advanced disease. A mature sequence of MiR-31, MiR-31-3p, has been shown to predict outcomes among for colorectal cancer patients treated with anti-EGFR therapy such as ERBITUX® and VECTIBIX®.
FIRE-3 is an open-label, randomized Phase III trial in which FOLFIRI plus ERBITUX® was compared with FOLFIRI plus AVASTIN®, as first line treatment in patients with metastatic ColoRectal Cancer (CRC). This study suggested that patients with KRAS exon 2 wild-type metastatic CRC had a longer Overall Survival (OS) when treated with FOLFIRI plus ERBITUX® compared with FOLFIRI plus AVASTIN®.
Based on the premise that MiR-31-3p expression has been shown to be associated with response to anti-EGFR therapy, in previously published studies, the authors investigated the predictive role of this biomarker in the FIRE-3 study patient population, in its ability to differentiate outcomes between patients receiving anti-EGFR and anti-VEGF therapy. In this study, MiR-31-3p expression was measured in primary tumors obtained from 340 RAS wild-type mCRC patients enrolled in the FIRE-3 Trial. The study population included 164 patients randomized to receive FOLFIRI plus ERBITUX® and 176 patients to FOLFIRI plus AVASTIN®. Patients were divided into subgroups, defined by Low or High MiR-31-3p expression.
It was noted that patients with Low MiR-31-3p expression benefited from ERBITUX® combination compared to AVASTIN® for PFS (HR=0.74;P=0.05), OS (HR=0.61;P<0.01) and Objective Response Rate (P<0.01). There was however no difference in outcomes among High MiR-31-3p expressors between the two treatment groups.
It was concluded that MiR-31-3p expression level is a validated predictive biomarker of anti EGFR therapy efficacy for RAS wild-type mCRC patients, and can enable clinicians to identify patients who would benefit from first-line anti-EGFR treatment. MiRNAs are well preserved in Formalin-Fixed Paraffin-Embedded (FFPE) tissues and MiR-31- 3p expression levels can be measured using RT qPCR. Validation of miR-31-3p Expression to Predict Cetuximab Efficacy When Used as First-Line Treatment in RAS Wild-Type Metastatic Colorectal Cancer. Laurent-Puig P, Grisoni ML, Heinemann V, et al. Clin Cancer Res. 2018 Aug 14. pii: clincanres.1324.2018. doi: 10.1158/1078-0432.CCR-18-1324. [Epub ahead of print]
American Cancer Society Updates Colorectal Cancer Screening Guideline for Average Risk Adults
SUMMARY: The American Cancer Society estimates that approximately 140,250 new cases of ColoRectal Cancer will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%). ColoRectal cancer (CRC) is the fourth most common cancer diagnosed among adults in the US and the second leading cause of death from cancer.
The ACS recently updated Colorectal Cancer Screening Guideline using prevailing evidence as well as microsimulation modeling analyses, and included a new evaluation of the age, to begin screening by race and sex and additional modeling that incorporates changes in United States CRC incidence. The ACS Guideline Development Group applied the Grades of Recommendations, Assessment, Development, and Evaluation (GRADE) criteria in developing and rating the recommendations. The new guideline does not prioritize among screening test options. This is because test preferences vary among individuals and the guidelines development committee emphasized that screening rates could be improved by endorsing the full range of tests without preference.
Even though the incidence of Colorectal cancer (CRC) in the United States has been rapidly declining overall in people 55 and over primarily driven by screening, among adults younger than 55 years there was a 51% increase in the incidence of colorectal cancer (CRC) from 1994 to 2014 and a 11% increase in deaths from 2005 to 2015. Adults born around 1990 have twice the risk of colon cancer and four times the risk of rectal cancer compared with adults born around 1950, who have the lowest risk. Studies suggest that the younger individuals will continue to be at a higher risk as they age. The increase in the incidence of CRC in young adults has been attributed to western life style including high carbohydrate, high fat, low fiber diet which can initiate inflammation and proliferation in the colonic mucosa within two weeks. Other lifestyle factors associated with CRC include obesity, high consumption of processed meat and alcohol, low levels of physical activity and cigarette smoking. Further, young patients are 58% more likely than older patients to be diagnosed with advanced versus localized stage CRC, due to delayed follow up of symptoms, sometimes for years, and these young adults are less likely to be screened for colon cancer, despite their symptoms.
The current ACS recommendations are as follows:
1) Adults aged 45 and older with an average risk of colorectal cancer should undergo regular screening with either a high-sensitivity stool-based test or a structural (visual) exam, depending on patient preference and test availability.
2) As a part of the screening process, all positive results on non-colonoscopy screening tests should be followed up with timely colonoscopy.
3) The recommendation to begin screening at age 45 years is a “qualified recommendation”. The change in starting age is designated as a “qualified recommendation” because there is less direct evidence of the balance of benefits and harms, or patients’ values and preferences, related to colorectal cancer screening in adults aged 45 to 49, since most studies have only included adults aged 50 and older.
4) The recommendation for regular screening in adults aged 50 years and older is designated as a “strong recommendation,” on the basis of the greater strength of the evidence and the judgment of the overall benefit.
5) Average-risk adults in good health with a life expectancy of greater than 10 years should continue colorectal cancer screening through age 75 years.
6) Clinicians should individualize colorectal cancer screening decisions for individuals aged 76 through 85 years, based on patient preferences, life expectancy, health status, and prior screening history.
7) Clinicians should discourage individuals over age 85 years from continuing colorectal cancer screening.
Test options for CRC screening include the following:
Stool-based tests
1) Highly sensitive Fecal Immunochemical Test (FIT) annually
2) Highly sensitive guaiac-based Fecal Occult Blood Test (gFOBT) annually
3) Multi-targeted stool DNA test every 3 years
Visual exams
1) Colonoscopy every 10 years
2) CT colonography (virtual colonoscopy) every 5 years
3) Flexible sigmoidoscopy every 5 years
Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. Wolf AM, Fontham ET, Church TR, et al. CA Cancer J Clin 2018;68:250-281.
FDA Approves OPDIVO® and YERVOY® Combination for Metastatic Colorectal Cancer
SUMMARY: The FDA on July 10, 2018, granted accelerated approval to YERVOY® (Ipilimumab) for use in combination with OPDIVO® (Nivolumab), for the treatment of patients 12 years of age and older with MicroSatellite Instability-High (MSI-H) or MisMatch Repair deficient (dMMR) metastatic ColoRectal Cancer, that has progressed following treatment with a Fluoropyrimidine, Oxaliplatin, and Irinotecan. The FDA in July, 2017, granted accelerated approval to single agent OPDIVO® (Nivolumab) for treatment of this same group of patients. ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of CRC will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%).
The DNA MisMatchRepair (MMR) system is responsible for molecular surveillance and works as an editing tool that identifies errors within the microsatellite regions of DNA and removes them. Defective MMR system leads to MSI (Micro Satellite Instability) and hypermutation, triggering an enhanced antitumor immune response. MSI (Micro Satellite Instability) is therefore a hallmark of defective/deficient DNA MisMatchRepair (dMMR) system and occurs in 15% of all colorectal cancers. Defective MisMatchRepair can be a sporadic or heritable event. Approximately 65% of the MSI tumors are sporadic and when sporadic, the DNA MisMatchRepair gene is MLH1. Defective MisMatchRepair can also manifest as a germline mutation occurring in 1 of the 4 MisMatchRepair genes which include MLH1, MSH2, MSH6, PMS2. This produces Lynch Syndrome (Hereditary Nonpolyposis Colorectal Carcinoma – HNPCC), an Autosomal Dominant disorder and is the most common form of hereditary colon cancer, accounting for 35% of the MSI colorectal cancers. MSI tumors tend to have better outcomes and this has been attributed to the abundance of tumor infiltrating lymphocytes in these tumors from increase immunogenicity. These tumors therefore are susceptible to blockade with immune checkpoint inhibitors. MSI (Micro Satellite Instability) testing is performed using a PCR based assay and MSI-High refers to instability at 2 or more of the 5 mononucleotide repeat markers and MSI-Low refers to instability at 1 of the 5 markers. Patients are considered Micro Satellite Stable (MSS) if no instability occurs. MSI-L and MSS are grouped together because MSI-L tumors are uncommon and behave similar to MSS tumors. Tumors considered MSI-H have deficiency of one or more of the DNA MisMatchRepair genes. MMR gene deficiency can be detected by ImmunoHistoChemistry (IHC). MLH1 gene is often lost in association with PMS2. NCCN Guidelines recommend MMR or MSI testing for all patients with a history of Colon or Rectal cancer.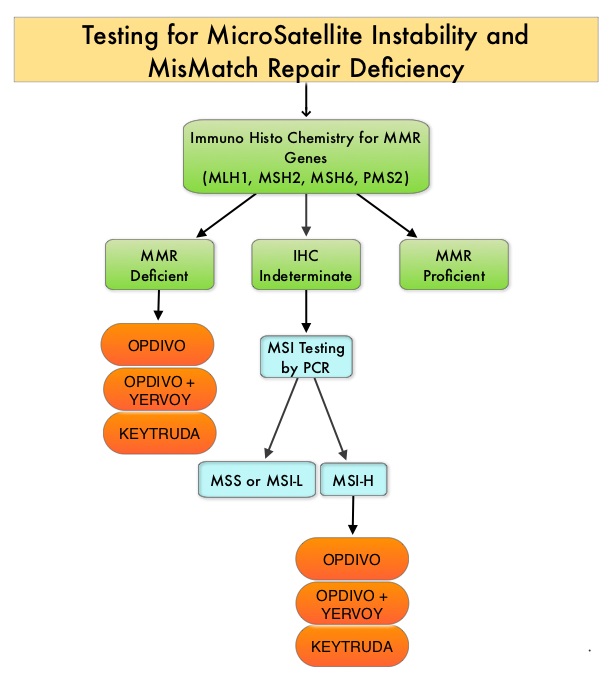
OPDIVO® is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, whereas YERVOY® is a fully human immunoglobulin G1 monoclonal antibody that blocks Immune checkpoint protein/receptor CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152). Blocking the Immune checkpoint proteins unleashes the T cells, resulting in T cell proliferation, activation and a therapeutic response.
This new FDA approval was based on data from the ongoing CheckMate-142, which is a multicenter, open-label, phase II trial, designed to determine within the dMMR/MSI-H population, whether OPDIVO® alone or in combination with another checkpoint inhibitor YERVOY®, could result in meaningful responses in patients with metastatic CRC, following at least one prior line of therapy. This study was not designed to compare the outcomes in cohorts receiving single agent OPDIVO® and combination checkpoint inhibitors. The rationale behind combining OPDIVO® a PD-1 inhibitor and YERVOY®, a CTLA-4 inhibitor, was based on the synergy between these two agents, to promote T-cell antitumor activity, thereby improving upon single-agent activity of OPDIVO®.
This study enrolled 74 patients, who received single agent OPDIVO® 3 mg/kg IV every 2 weeks and 119 patients who received OPDIVO® 3 mg/kg IV plus YERVOY® 1 mg/kg IV, every 3 weeks for four doses, followed by OPDIVO® 3 mg/kg as a single agent every 2 weeks, until unacceptable toxicity or radiographic progression. In this study, from a cohort of 119 patients with MSI-H or dMMR mCRC, 82 patients received prior treatment with a Fluoropyrimidine, Oxaliplatin, and Irinotecan. Among the cohort of 119 patients receiving OPDIVO® plus YERVOY®, the median age was 58 years, 29% had a known history of Lynch syndrome, 24% had BRAF mutations, 37% had KRAS mutations and 22% of patients had high PD-L1 expression (1% or more) on tumor cells at baseline. Primary tumor location was in the right colon in 55% of patients, 25% had left and sigmoid colon disease and 13% had primary tumor in the transverse colon. Seventy six percent (76%) of patients had two or more prior lines of therapy. The Primary end point was investigator-assessed ORR (Overall Response Rate) and Secondary end points included DCR (Disease Control Rate - CR, PR, or stable disease) Safety and tolerability, PFS (Progression Free Survival) and OS (Overall Survival).
At median follow-up of 13.4 months, the ORR in those patients receiving OPDIVO® plus YERVOY®, was 55% and the Disease Control Rate for 12 or more weeks was 80%. Median duration of response was not reached and 94% of the responses were ongoing at data cutoff. PFS and OS rates at 1 year were 71% and 85%, respectively. Further, clinically meaningful and statistically significant improvements were observed in patient-reported outcomes, including functioning, symptoms, and quality of life. Approximately 13% of patients who discontinued treatment because of toxicities still had an ORR of 63%, consistent with that of the overall population. Grade 3 to 4 toxicities occurred in 32% of patients and were manageable. Indirect comparisons in this nonrandomized CheckMate-142 trial suggested that OPDIVO® plus YERVOY® provided numerically higher response rates and improved long term clinical benefit relative to OPDIVO® monotherapy.
It was concluded that OPDIVO® plus YERVOY® results in a high response rates, encouraging PFS and OS at 12 months, with manageable toxicities. These data from the CheckMate-142 study support the use of OPDIVO® as a single agent or in combination with YERVOY®, for the treatment of patients with previously treated dMMR/MSI-H metastatic CRC. Durable Clinical Benefit With Nivolumab Plus Ipilimumab in DNA Mismatch Repair–Deficient/Microsatellite Instability–High Metastatic Colorectal Cancer. Overman MJ, Lonardi S, Wong KYM, et al. J Clin Oncol. 2018;36:773-779
Higher Plasma Vitamin D Levels Associated with Lower Colorectal Cancer Risk
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer and third leading cause of cancer-related deaths in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of ColoRectal Cancer will be diagnosed in the United States in 2018 and over 50,630 patients are expected to die of the disease. The lifetime risk of colorectal cancer is 4.2% (1 in 24) in women and 4.5% (1 in 22) in men.
Vitamin D is known for its role in maintaining bone health and there is a growing body of evidence suggesting that Vitamin D has colon cancer preventing properties and may induce antitumor immunity. A study by Song and colleagues (Gut. 2015;64:260-271) showed that high plasma level 25-Hydroxy Vitamin D [25(OH)D] was associated with lower risk of colorectal cancer with intense immune reaction, supporting that vitamin D through tumor-host interaction may play a role in cancer immunoprevention. There also appears to be a strong association between plasma 25(OH)D level and colorectal cancer (CRC) specific mortality, with better outcomes in CRC patients with higher plasma levels of 25(OH)D, treated with a combination of chemotherapy and biologic agents. However the plasma concentrations of 25(OH)D that minimize colorectal cancer risk are unknown and even though epidemiological studies suggest a protective role for vitamin D in colorectal carcinogenesis, the evidence has been inconclusive. The current recommendations regarding vitamin D intake are based only on bone health. Sources of vitamin D include fatty fish like salmon, tuna and mackerel, foods fortified with vitamin D like some dairy products, cereals and orange juice as well as egg yolks. It is recommended that vitamin D be obtained through diet whenever possible rather than sun exposure, because of the risk of skin cancer with excessive UV radiation.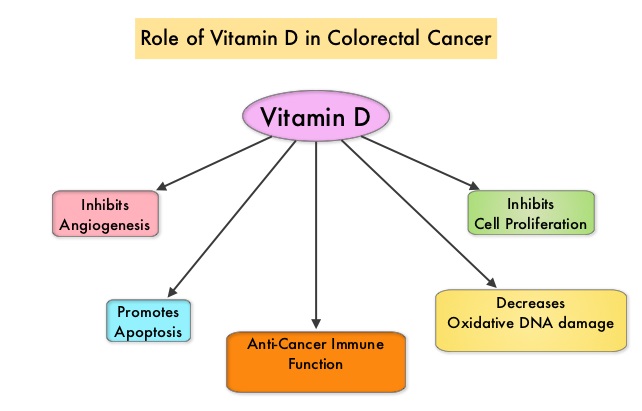
The Institute of Medicine defines vitamin D deficiency as plasma 25(OH)D level of less than 50 nmol/L and the plasma 25(OH)D threshold for fracture prevention is 75 nmol/L. All adults aged 50-70 years and more than 70 years will require at least 600 and 800 IU (15-20 μg) of vitamin D3 per day, respectively, for optimal bone health and muscle function. However, to raise the plasma level of 25(OH)D above 75 nmol/L, individuals will require at least 1500-2000 IU (37.5–50 μg) per day of supplemental vitamin D. Doses of up to 10 000 IU (250 μg) per day have been proven to be safe.
This present study was conducted to address inconsistencies in prior studies, on the protective role for vitamin D in colorectal cancer, and to investigate associations in population subgroups. The authors analyzed participant-level data, collected before colorectal cancer diagnosis, from 17 prospective cohorts which included 5706 colorectal cancer cases and 7107 control participants, from the US, Europe, and Asia, with a wide range of plasma 25(OH)D concentrations. A single, widely accepted assay and laboratory was used for new plasma 25(OH)D measurements, and calibration of previously measured plasma 25(OH)D. This calibration approach enabled the authors to systematically explore risk, utilizing the same assay, over the broad range of vitamin D levels seen internationally.
It was noted that compared to participants with plasma 25(OH)D concentrations sufficient for bone health (50-62.5 nmol/L), those with deficient 25(OH)D levels (less than 30 nmol/L) had a 31% higher risk of colorectal cancer during follow-up, which averaged 5.5 years. In contrast, individuals with plasma 25(OH)D levels above sufficiency for bone health, (75 to less than 87.5 nmol/L) had 19% lower risk and among those with plasma 25(OH)D levels 87.5 to less than 100 nmol/L, the risk of developing colorectal cancer was even lower at 27%. The risk however, did not continue to decline at plasma 25(OH)D levels of 100 nmol/L or greater. The protective association of high levels of plasma 25(OH)D persisted even after adjusting for known colorectal cancer risk factors such as Body Mass Index, physical activity, and other risk factors, and was seen in all subgroups examined. The protective association was more significant in women than men at plasma 25(OH)D levels above bone health sufficiency. For each 25 nmol/L increment in plasma 25(OH)D levels, colorectal cancer risk was 19% lower in women and 7% lower in men.
It was concluded that higher plasma 25(OH)D levels (75-100 nmol/L) was associated with a statistically significant lower colorectal cancer risk in women and non-statistically significant lower risk in men. This study suggested that the optimal plasma 25(OH)D level concentrations for colorectal cancer risk reduction appear higher than the levels recommended for bone health. Circulating Vitamin D and Colorectal Cancer Risk: An International Pooling Project of 17 Cohorts. McCullough ML, Zoltick ES, Weinstein SJ, et al. JNCI: Journal of the National Cancer Institute, https://doi.org/10.1093/jnci/djy087. Published: 14 June 2018.
Elevated Postoperative CEA is an Early Indicator of Colon Cancer Recurrence
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of ColoRectal Cancer will be diagnosed in the United States in 2018 and over 50,630 patients are expected to die of the disease. CarcinoEmbryonic Antigen (CEA) is a group of highly related glycoproteins involved in cell adhesion and was first described in 1965. CEA is normally produced in gastrointestinal tissue during fetal development and is usually present at very low levels in the serum of healthy adults. Elevated serum levels of CEA are seen in certain malignancies and also in heavy smokers. Measurement of CEA is recommended for patients with colorectal cancer as a surveillance tool for early detection of potentially curable recurrent disease, following primary resection. Further, elevated preoperative CEA in patients with nonmetastatic colorectal cancer is associated with worse outcomes, in patients with early-stage disease (Stages I-III), independent of tumor stage. Lack of CEA normalization after resection of the primary tumor, is indicative of residual occult disease. Clinically, patients with an elevated preoperative CEA and an otherwise normal contrast-enhanced CT of the chest, abdomen, and pelvis proceed to surgery with the assumption that the primary lesion is the source of the elevated CEA.
This study was conducted to determine whether pre or postoperative CEA is more prognostic and more specifically whether patients with elevated preoperative CEA that normalizes after resection of the primary tumor had a risk of recurrence similar to that of patients with normal preoperative CEA. In this retrospective cohort study conducted at a comprehensive cancer center, 1027 consecutive patients with Stage I-III colon cancer who underwent curative resection and who had a preoperative CEA result available, were identified. Patients were then grouped into 3 cohorts - normal preoperative CEA, elevated preoperative but normalized postoperative CEA, and elevated preoperative and postoperative CEA. The Primary end point was Recurrence Free Survival (RFS) at 3 years.
The 3-year RFS rate for the patients with elevated preoperative CEA (N=312) was 82.3% compared with 89.7% for the patients (N=715) with normal preoperative CEA (HR=1.68; P=0.05). This represented a 7.4% higher 3-year RFS among patients with normal preoperative CEA compared with those with elevated preoperative levels. The negative prognostic impact of elevated preoperative CEA was negated in those patients whose CEA normalized in the postoperative period. Patients with elevated postoperative CEA (N=57) had a 3-year RFS of 74.5% compared with 89.4% for the patients with either normal preoperative CEA (N=715) or normalized postoperative CEA (N=142), (HR=2.53; P=0.001). This represented a 14.9% higher 3-year RFS for patients with normal postoperative CEA, regardless of preoperative level, compared to those with elevated postoperative CEA. Multivariate analyses confirmed that elevated postoperative CEA but not normalized postoperative CEA was independently associated with shorter RFS.
It was concluded that elevated preoperative CEA that normalizes after resection is not an indicator of poor prognosis. Patients with elevated postoperative CEA are at increased risk for recurrence especially within the first 12 months after surgery. Routine measurement of postoperative, rather than preoperative CEA is strongly recommended and CEA can be a valuable biomarker and is an early indicator of tumor recurrence. Association of Preoperative and Postoperative Serum Carcinoembryonic Antigen and Colon Cancer Outcome. Konishi T, Shimada Y, Hsu M, et al. JAMA Oncol. 2018;4:309-315
Shorter Duration of Adjuvant Chemotherapy for Stage III Colon Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of ColoRectal Cancer will be diagnosed in the United States in 2018 and over 50,630 patients are expected to die of the disease. Adjuvant chemotherapy for patients with resected, locally advanced, node-positive (stage III) colon cancer, has been the standard of care since the 1990s. Adjuvant treatment with an ELOXATIN® (Oxaliplatin) based chemotherapy regimen has been considered standard intervention since 2004, for patients with stage III colon cancer, following surgical resection, and has been proven to decrease the chance of recurrent disease. Chemotherapy regimens have included (FOLFOX - Leucovorin, 5-FluoroUracil, ELOXATIN®) or CAPOX/XELOX (XELODA®/Capecitabine and ELOXATIN®), given over a period of 6 months. ELOXATIN® can however be associated with neuropathy which can be long lasting or permanent, depending on the duration of therapy. Additional toxicities with longer duration of chemotherapy include diarrhea, fatigue as well as more office visits.
The IDEA Collaboration is a prospective, pre-planned pooled analysis of 6 concurrently conducted randomized phase III trials, which included 12,834 patients from 12 countries. The goal of this study was to determine if 3 months of adjuvant chemotherapy would be as effective as 6 months of therapy and would be non-inferior. Of the enrolled patients with stage III disease, 13% had T1-2 disease, 66% had T3 tumors and 21% had T4 tumors. Seventy one percent (71%) had N1 disease and 28% of the patients had N2 disease. Approximately 60% had low-risk disease (T1-3, N1) and 40% had high-risk (T4 or N2). Overall, about 40% of patients received CAPOX regimen and 60% received FOLFOX regimen. The primary endpoint was Disease Free Survival (DFS).
At a median follow up of 41.8 months, although non-inferiority of 3 months of therapy as compared with 6 months of therapy could not be confirmed in the overall treatment population, clinically relevant findings according to treatment were noted, in prespecified subgroups of patients. Among those patients who received FOLFOX regimen, 6 months of adjuvant therapy was superior to 3 months (HR=1.16; P=0.001 for superiority of 6-month therapy). However, among those patients who received CAPOX, the Disease Free Survival for 3 months versus 6 months was non-inferior (HR=0.95; P=0.006), and this was highly significant.
In an exploratory analysis, it was noted that among the patient group with low-risk cancers (T1-3, N1 cancers), 3 months of therapy was non-inferior to 6 months of therapy (HR= 1.01) with 3-year disease-free survival of 83.1% and 83.3%, respectively. However, among the patients with high-risk cancers (T4, N2, or both), 6 months of adjuvant therapy was superior to 3 months (HR= 1.12; P=0.01 for superiority).
When subgroup analysis was performed according to treatment and risk group, among the patients with low-risk tumors, 3 months of adjuvant therapy with CAPOX was non-inferior to 6 months of therapy. Outcomes after 3 months of adjuvant FOLFOX therapy were worse than those after 6 months, independent of risk group. For patients with high-risk tumors, 6 months of adjuvant therapy with FOLFOX was superior to 3 months, with a 3-year disease-free survival of 64.7% versus 61.5%. It has been hypothesized that the protracted delivery of a Fluoropyrimidine with CAPOX might have been more effective than the twice-monthly 5-FUinfusions with FOLFOX as an adjuvant therapy. Grade 2 or more neurotoxicity was significantly lower for patients who received 3 months of adjuvant therapy versus 6 months (P <0.0001), regardless of the treatment regimen (17% vs 48% for FOLFOX and 15% vs 45% for CAPOX/XELOX, respectively).
It was concluded by the IDEA collaboration that, a risk-based approach has to be taken when making adjuvant chemotherapy recommendations for patients with stage III colon cancer, taking into consideration choice of treatment regimen and duration of therapy. In patients treated with adjuvant CAPOX/XELOX regimen, 3 months of therapy was as effective as 6 months, particularly in the low risk subgroup. In patients treated with FOLFOX, 6 months of adjuvant therapy compared to 3 months, resulted in a higher rate of Disease Free Survival, particularly in the high-risk subgroup. Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. Grothey A, Sobrero AF, Shields AF, et al. N Engl J Med 2018; 378:1177-1188
Treatment Sequencing with STIVARGA® before ERBITUX® Improves Survival in Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of CRC will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%). Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable. Standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC, whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now also clear that even among the KRAS Wild Type patients, about 15-20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Therefore, pan RAS (expanded RAS) testing is now recommended.
STIVARGA® (Regorafenib), is an oral multi-kinase inhibitor approved by the FDA for the treatment of patients with metastatic CRC, who have progressed on 5FU, ELOXATIN® (Oxaliplatin), CAMPTOSAR® (Irinotecan), anti-VEGF and anti-EGFR therapies. STIVARGA® inhibits multiple kinases including VEGF1, VEGF2, VEGF3, PDGFR, FGFR involved in tumor angiogenesis and KIT, RET, RAF-1, BRAF involved in oncogenesis. The approval was based on a phase III trial in which patients receiving STIVARGA® had a statistically significant improvement in the Overall Survival and Progression Free Survival, compared to placebo.
Both STIVARGA® and ERBITUX® are approved for metastatic CRC. The optimal sequencing of these drugs however, has remained unclear. The current standard of care is to offer an ERBITUX® based regimen followed by STIVARGA®. STIVARGA® however has demonstrated activity in patients with metastatic CRC, when given earlier in the course of the disease. Further preclinical data suggests that downregulation of MAP kinase and Akt with STIVARGA® was shown to sensitize metastatic CRC cells to anti-EGFR therapies, such as ERBITUX®.
The REVERCE trial is a multicenter, randomized phase II trial which enrolled patients with KRAS wild-type metastatic CRC, after failure on combination chemotherapy with Fluoropyrimidine, Oxaliplatin, and Irinotecan. A total of 101 patients were randomized in a 1:1 ratio to receive sequential treatment with STIVARGA® followed by ERBITUX® with or without Irinotecan or reverse sequence of ERBITUX® with or without Irinotecan followed by STIVARGA®. Patients were stratified by prior use of AVASTIN® and intent to use ERBITUX® in combination with Irinotecan. Patients continued each sequence until disease progression or unacceptable toxicity, at which time patients switched to the alternative drug. The Primary endpoint was Overall Survival. Secondary endpoints included Progression Free Survival (PFS) with initial treatment (PFS1), PFS with second treatment (PFS2), Time to sequential Treatment Failure (TTF), Response Rate, Safety, and Quality of Life (QOL). The authors further investigated possible biomarkers including oncogenic mutations from circulating cell free DNA by liquid biopsy, with serial measurements.
It was noted that giving STIVARGA® before ERBITUX® resulted in a significantly longer median Overall Survival of 17.4 months, compared with 11.6 months with ERBITUX® followed by STIVARGA®. After a median follow up of 29 months, there was a 39% reduction in the risk of death with the STIVARGA®-ERBITUX® sequence (HR=0.61; P=0.029). The benefit with STIVARGA®-ERBITUX® sequence was consistently noted across all patient subgroups. In the subgroup of patients with left-sided primary tumors (N=81), patients who started treatment with STIVARGA® first followed by ERBITUX®, had a median Overall Survival of 20.5 months compared with 11.9 months for those receiving ERBITUX® first, and this meant a 49% reduction in mortality risk, which was statistically significant (P=0.01).
The first Progression Free Survival (PFS1) did not differ significantly according to the drug sequence, but the second PFS (PFS2) was more prolonged in those receiving ERBITUX® after STIVARGA®, with a 71% reduction in the risk of progression or death following the second treatment (HR=0.29; P<0.0001). The time to treatment failure was a median of 7.4 months with STIVARGA® followed by ERBITUX® and 6.1 months with ERBITUX® followed by STIVARGA® (HR=0.60; P=0.017). Safety and quality of life were comparable between the two treatment groups.
It was concluded that data from this study suggest that treatment with STIVARGA® first, followed by ERBITUX® resulted in longer survival than that of the current standard sequence and the longer Progression Free Survival following the second treatment period with ERBITUX® may have contributed to the improvement in Overall Survival with the STIVARGA®-ERBITUX® sequence. A biomarker analysis is still ongoing. Randomized phase II study of regorafenib followed by cetuximab versus reverse sequence for wild-type KRAS metastatic colorectal cancer previously treated with fluoropyrimidine, oxaliplatin, and irinotecan (REVERCE). Shitara K, Yamanaka T, Denda T, et al. DOI: 10.1200/JCO.2018.36.4_suppl.557 Journal of Clinical Oncology 36, no. 4_suppl (February 2018) 557-557.
Germline Testing with NGS Multigene Cancer Panels Recommended for All Young Patients with Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of CRC will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%).
Even though the incidence of Colorectal cancer (CRC) in the United States has been rapidly declining overall, primarily driven by screening, the incidence however has been increasing among adults younger than age 50 years. Currently, genetic testing is recommended in patients with polyposis phenotypes, strong family histories, and those whose tumors demonstrate MicroSatellite Instability (MSI) or fail to stain for MisMatch Repair (MMR) gene proteins by immunohistochemistry. Whether patients younger than 50 years of age with CRC, should be tested with a broad multigene panel to detect additional genetic abnormalities, has remained unclear.
The authors conducted this study to ascertain the proportion of young CRC cases associated with genetic predisposition. In this retrospective study, 430 individuals diagnosed with CRC at an age younger than 50 years were evaluated by the clinical genetics service at a single tertiary care cancer center from 1998 through 2015. Data collection included patient histories, tumor phenotypes, and results of germline DNA sequencing. If information was uninformative, germline DNA samples were resequenced using a research-based Next-Generation Sequencing multigene panel. The primary outcome was identification of a pathogenic germline mutation associated with cancer predisposition.
The researchers noted that 26% of young CRC cases had a first-degree relative with CRC and 10% had tumors with histologic evidence for MisMatch Repair (MMR) deficiency and 6% had polyposis phenotype. Germline mutations associated with a hereditary cancer syndrome were identified in 79 patients (18%) following clinically driven germline sequencing, and Next-Generation Sequence analysis using a multigene panel detected actionable germline variants in 6 patients (5%) with uninformative clinical evaluations. Lynch syndrome was identified in 56 patients (14%) of the entire cohort, Familial Adenomatous Polyposis in 2%, MUTYH in 2%, and SMAD4 was mutated in 2 patients, BRCA1 in one, TP53 in one, and CHEK2 in one. Only 51% of the patients with germline mutations associated with a hereditary cancer syndrome gave a family history of CRC diagnosis in a first-degree relative.
The authors concluded that 20% of patients diagnosed with CRC at age younger than 50 years carry a germline mutation associated with cancer, and half of these patients do not have clinical histories typically associated with the identified syndrome. Germline testing with Next-Generation Sequencing multigene cancer panels should therefore be considered for all young patients with CRC. Germline Genetic Features of Young Individuals with Colorectal Cancer. Stoffel EM, Koeppe E, Everett J, et al. Gastroenterology 2017 Nov 13; [e-pub]. (http://dx.doi.org/10.1053/j.gastro.2017.11.004)
OPDIVO® and YERVOY® Combination Improves Survival in Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 140,250 new cases of CRC will be diagnosed in the United States in 2018 and about 50,630 patients are expected to die of the disease. The lifetime risk of developing CRC is about 1 in 21 (4.7%).
The DNA MisMatchRepair (MMR) system is responsible for molecular surveillance and works as an editing tool that identifies errors within the microsatellite regions of DNA and removes them. Defective MMR system leads to MSI (Micro Satellite Instability) and hypermutation, triggering an enhanced antitumor immune response. MSI (Micro Satellite Instability) is therefore a hallmark of defective/deficient DNA MisMatchRepair (dMMR) system and occurs in 15% of all colorectal cancers. Defective MisMatchRepair can be a sporadic or heritable event. Approximately 65% of the MSI tumors are sporadic and when sporadic, the DNA MisMatchRepair gene is MLH1. Defective MisMatchRepair can also manifest as a germline mutation occurring in 1 of the 4 MisMatchRepair genes which include MLH1, MSH2, MSH6, PMS2. This produces Lynch Syndrome (Hereditary Nonpolyposis Colorectal Carcinoma – HNPCC), an Autosomal Dominant disorder and is the most common form of hereditary colon cancer, accounting for 35% of the MSI colorectal cancers. MSI tumors tend to have better outcomes and this has been attributed to the abundance of tumor infiltrating lymphocytes in these tumors from increase immunogenicity. These tumors therefore are susceptible to PD-1 blockade with immune checkpoint inhibitors.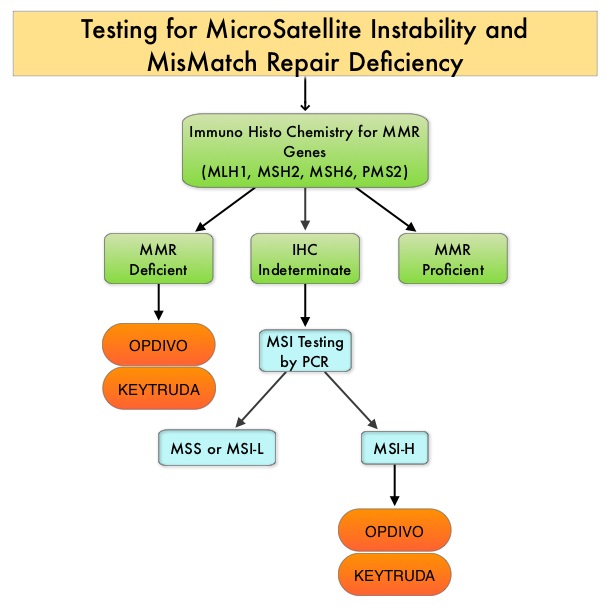
MSI (Micro Satellite Instability) testing is performed using a PCR based assay and MSI-High refers to instability at 2 or more of the 5 mononucleotide repeat markers and MSI-Low refers to instability at 1 of the 5 markers. Patients are considered Micro Satellite Stable (MSS) if no instability occurs. MSI-L and MSS are grouped together because MSI-L tumors are uncommon and behave similar to MSS tumors. Tumors considered MSI-H have deficiency of one or more of the DNA MisMatchRepair genes. MMR gene deficiency can be detected by ImmunoHistoChemistry (IHC). MLH1 gene is often lost in association with PMS2. NCCN Guidelines recommend MMR or MSI testing for all patients with a history of Colon or Rectal cancer.
CheckMate 142 is a large, multi-center, open label, phase II trial which evaluated the efficacy and safety of PD-1 inhibitor treatment in patients with dMMR/MSI-H metastatic colorectal cancer. This study evaluated the benefit of OPDIVO® alone or in combination YERVOY® in this patient population. The rationale behind combining OPDIVO® a PD-1 inhibitor and YERVOY®, a CTLA-4 inhibitor, was based on the synergy between these two agents, to promote T-cell antitumor activity, thereby improving upon single-agent activity of OPDIVO®. The study enrolled 119 patients who received OPDIVO® as a single agent at 3 mg/kg IV every 2 weeks or OPDIVO® 3 mg/kg plus YERVOY® 1 mg/kg every 3 weeks for 4 doses, followed by OPDIVO® 3 mg/kg every 2 weeks. Treatment was continued until disease progression or unacceptable toxicities. The Primary endpoint was Objective Response Rate (ORR) and exploratory endpoints included Safety, Progression Free Survival (PFS), Overall Survival (OS) and efficacy in biomarker-defined populations. This study was not designed to compare the outcomes in these two treatment cohorts. Based on initial data from CheckMate-142, the FDA in July 2017 granted accelerated approval to OPDIVO® for the treatment of patients with MisMatch Repair deficient (dMMR) and MicroSatellite Instability-High (MSI-H) metastatic CRC, that has progressed, following treatment with a Fluoropyrimidine, Oxaliplatin, and Irinotecan.
This review provides an update on outcomes with monotherapy and immunotherapy combination. In the OPDIVO® monotherapy group which included 74 patients, the updated analysis at 21 months showed a response rate was 34%, with 9% being complete responses, and the disease control rate was 62%. The median duration of response has not been reached in the overall cohort of patients and among those responding, 64% had responses lasting at least 1 year. Longer follow up resulted in deepening response rates. The median Progression Free Survival (PFS) for the entire cohort was 6.6 months. Clinical Benefit was seen regardless of PD-L1 expression, BRAF mutation status, KRAS mutation status, and clinical history of Lynch Syndrome.
In the combination immunotherapy group, the median follow up was 13.4 months and the authors of this analysis, André, et al., compared the results of this cohort with those of the OPDIVO® monotherapy group, for the same 13.4 month median follow up period. The most common prior therapies included Fluoropyrimidine (99%), Oxaliplatin (93%) and Irinotecan (73%). Of the 119 patients who received this combination immunotherapy, 76% had 2 or more prior lines of therapy. The Objective Response Rate with a combination of OPDIVO® and YERVOY® was 55%, with 3.4% Complete Responses, and the Disease Control Rate was 80%. About 78% of the patients had reduction in tumor burden with combination immunotherapy. The median time to response was 2.8 months and the median Duration of Response has not yet been reached. Among patients who responded to the combination, 94% had ongoing responses at the time of data cutoff and 63% of the cohort receiving combination immunotherapy remained on treatment. These responses were noted regardless of PD-L1 expression, BRAF or KRAS mutation status, or clinical history of Lynch syndrome. The PFS and Overall Survival with combination immune checkpoint inhibitor therapy at 12 months were 71% and 85%, respectively. There were statistically significant and clinically meaningful improvements in quality-of-life measurements as well.
These data from the CheckMate-142 study support the use of OPDIVO® as a single agent or in combination with YERVOY®, for the treatment of patients with previously treated DNA MisMatch Repair-Deficient/MicroSatellite Instability-High (MSI-H) metastatic CRC.
1. Overman MJ, Bergamo F, McDermott RS, et al. Nivolumab in patients with DNA mismatch repair-deficient/microsatellite instability-high (dMMR/MSI-H) metastatic colorectal cancer (mCRC): Long-term survival according to prior line of treatment from CheckMate-142. Overman MJ, Bergamo F, McDermott RS, et al. J Clin Oncol 36, 2018 (suppl 4S; abstr 554)
2. Nivolumab + ipilimumab combination in patients with DNA mismatch repair-deficient/microsatellite instability-high (dMMR/MSI-H) metastatic colorectal cancer (mCRC): First report of the full cohort from CheckMate-142. André T, Lonardi S, Wong M, et al. J Clin Oncol 36, 2018 (suppl 4S; abstr 553)
Non-V600 BRAF Mutations Define a Clinically Distinct Molecular Subtype of Metastatic Colorectal Cancer with Excellent Prognosis
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. The lifetime risk of developing ColoRectal Cancer (CRC) is about 1 in 20 (5%). The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. The BRAF V600 mutations results in constitutive activation of the MAP kinase pathway. Inhibiting BRAF can transiently reduce MAP kinase signaling. However, this can result in feedback upregulation of EGFR signaling pathway, which can then reactivate the MAP kinase pathway. This aberrant signaling can be blocked by dual inhibition of both BRAF and EGFR.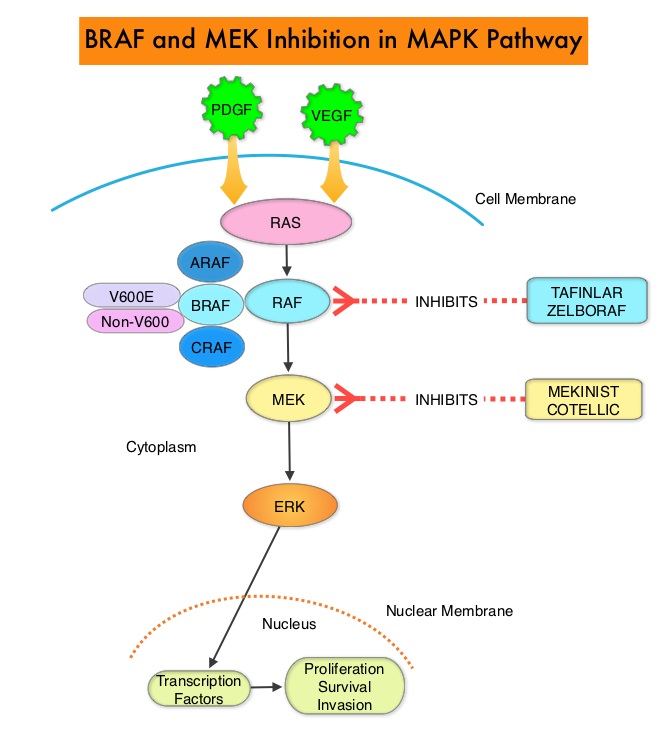
The initial evaluation of patients with metastatic ColoRectal Cancer (CRC) includes Molecular diagnostic testing including testing for extended RAS (RAt Sarcoma) and RAF (Rapid Accelerated Fibrosarcoma) mutations. Next-Generation Sequencing (NGS) allows expanded mutational testing for RAS which includes KRAS, NRAS and HRAS. RAS mutations are predictive of resistance to EGFR targeted therapy. NGS is able to detect approximately 20% of the patients who were originally classified as having KRAS Wild-Type (WT) metastatic CRC but were subsequently found to have KRAS or NRAS mutations, thus predicting resistance to EGFR targeted therapy.
Approximately 10% of CRCs detected by NGS harbor BRAF V600E mutation and the detection of BRAF V600E mutation is recognized as a marker of poor prognosis in patients with metastatic CRC. RAS and BRAF V600E mutations occur in a mutually exclusive fashion. Patients with this molecular subtype of CRC are older than age 60 years, more frequently female, have a right-sided tumor with high-grade histology, and often have MicroSatellite Instability (MSI-H). These patients often have peritoneal metastasis and despite chemotherapeutic intervention have a shortened overall survival. These tumors have limited response to EGFR targeted therapy and current guidelines recommend against the use of anti-EGFR antibodies in BRAF V600E-mutated mCRC.
The significance of non-V600 BRAF mutations detected by NGS however has remained unclear. The authors in this multicenter, retrospective cohort study, pooled NGS data from three large US reference laboratories and attempted to establish the clinical characteristics of patients with non-V600 BRAF mutations. Using NGS databases from the Mayo Clinic (MC), The University of Texas MD Anderson Cancer Center (MDACC), and Foundation Medicine (FM) from 2013-2016, patients with non-V600 BRAF mutations from these three institutions were identified and pooled for the primary analysis. Out of a total of 9,643 patients with metastatic CRC who underwent NGS testing, 208 patients with non-V600 BRAF mutations and 133 patients with V600E BRAF mutations, were identified. This study also included 249 patients with Wild-Type BRAF metastatic CRC, for comparative analysis , identified from the same NGS database, from the Mayo Clinic.
It was noted that the prevalence rate of any BRAF mutation was 10%, non-V600 BRAF mutations occurred in 2.2% of all patients tested and accounted for 22% of all BRAF mutations identified. Of particular clinical interest, compared with those with V600E BRAF mutations, patients harboring a non-V600 BRAF mutation were significantly younger, more frequently male, and presented with left-sided MicroSatellite-Stable (MSS) tumors. Additionally, non-V600 BRAF-mutated tumors were mostly low grade and did not often metastasize to the peritoneum. The median Overall Survival was significantly longer in patients with non-V600 BRAF-mutant metastatic CRC compared with those with both V600E BRAF-mutant and Wild-Type BRAF metastatic CRC (60.7 vs 11.4 vs 43.0 months, respectively; P<0.001) and in multivariable analysis, non-V600 BRAF mutation was independently associated with improved Overall Survival (HR=0.18; P<0.001).
This study concluded that Non-V600 BRAF mutations in metastatic ColoRectal Cancer (CRC), which accounted for 22% of all BRAF mutations identified by NGS, is a clinically distinct subtype of CRC, with an excellent prognosis and aggressive chemotherapeutic intervention could be avoided for this group of patients. Non-V600 BRAF Mutations Define a Clinically Distinct Molecular Subtype of Metastatic Colorectal Cancer. Jones JC, Renfro LA, Al-Shamsi HO, et al. J Clin Oncol 2017;35: 2624-2630
Study Finds Dramatic Increase in ColoRectal Cancer Incidence among Young Adults
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. The lifetime risk of developing ColoRectal Cancer is about 1 in 20 (5%).
Even though the incidence of Colorectal cancer (CRC) in the United States has been rapidly declining overall, primarily driven by screening, the incidence however has been increasing among adults younger than age 50 years. To understand this trend, the authors in this publication conducted a retrospective cohort study among 490,305 patients aged 20 years and older, who were diagnosed with colorectal cancer between 1974 and 2013, using data from nine oldest Surveillance, Epidemiology, and End Results (SEER) registries. The SEER program is considered the gold standard for cancer registration worldwide because of the high quality of data and is the only source for historical population-based cancer incidence in the United States. This study included people born in 1890 thru 1990. Colorectal cancer incidence trends were analyzed by 5-year age group and birth cohorts.
The authors noted variations in CRC incidence patterns by age, tumor location in the colon, calendar period, and birth cohort. The study found that in adults aged 20-39 years, after a decrease in the previous decade, colon cancer incidence rates increased by 1.0-2.4% per year since the mid-1980s thru 2013. For adults aged 40-54 years during the same period, colon cancer incidence rates increased by 0.5-1.3%. Conversely, from the mid-1980s thru 2013, colon cancer rates declined in adults aged 55 years and older. In adults younger than age 50 years, there was an increasing trend for tumors to be confined to the distal colon, with the exception of adults aged 40-49 years, among whom there was an also an increasing trend for proximal tumors.
The incidence of rectal cancer has been increasing even longer and faster than colon cancer, rising about 3.2% per year from 1974-2013 in adults aged 20-29 years and from 1980-2013 in adults aged 30-39 years. In adults aged 40 to 54, rectal cancer rates increased by 2.3% per year from the 1990s to 2013. Again, rectal cancer rates declined, in adults aged 55 years and older, from 1974-2013.
Compared with adults born around 1950, those born around 1990 had double the risk of colon cancer and quadruple the risk of rectal cancer. The increase in the incidence of CRC in young adults has been attributed to western style, high carbohydrate, high fat, low fiber diet which can initiate inflammation and proliferation in the colonic mucosa within two weeks. Other lifestyle factors associated with CRC include obesity, high consumption of processed meat and alcohol, low levels of physical activity and cigarette smoking. Further, young patients are 58% more likely than older patients to be diagnosed with advanced versus localized stage CRC, due to delayed follow-up of symptoms, sometimes for years and these young adults are less likely to be screened for colon cancer, despite their symptoms.
The authors concluded that there is an increasing rate of colon and rectal cancer among young and middle-aged adults in the US and compared with adults born around 1950 when the risk was at the lowest, those born around 1990 have double the risk of colon cancer and quadruple the risk of rectal cancer. They added that as nearly a third of rectal cancer patients are younger than age 55 years, screening initiation before age 50 years should be considered. Colorectal Cancer Incidence Patterns in the United States, 1974-2013. Siegel RL, Fedewa SA, Anderson WF, et al. J Natl Cancer Inst. 2017 Aug 1;109(8). doi: 10.1093/jnci/djw322.
FDA Approves OPDIVO® for MSI-H or dMMR Metastatic Colorectal Cancer
SUMMARY: The FDA on July 31, 2017, granted accelerated approval to OPDIVO® (Nivolumab) for the treatment of patients 12 years and older with MisMatch Repair deficient (dMMR) and MicroSatellite Instability-High (MSI-H) metastatic ColoRectal Cancer, that has progressed following treatment with a Fluoropyrimidine, Oxaliplatin, and Irinotecan. ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. The lifetime risk of developing ColoRectal Cancer is about 1 in 20 (5%).
The DNA MisMatchRepair (MMR) system is responsible for molecular surveillance and works as an editing tool that identifies errors within the microsatellite regions of DNA and removes them. Defective MMR system leads to MSI (Micro Satellite Instability) and hypermutation, triggering an enhanced antitumor immune response. MSI (Micro Satellite Instability) is therefore a hallmark of defective/deficient DNA MisMatchRepair (MMR) system and occurs in 15% of all colorectal cancers. Defective MisMatchRepair can be a sporadic or heritable event. Approximately 65% of the MSI tumors are sporadic and when sporadic, the DNA MisMatchRepair gene is MLH1. Defective MisMatchRepair can also manifest as a germline mutation occurring in 1 of the 4 MisMatchRepair genes which include MLH1, MSH2, MSH6, PMS2. This produces Lynch Syndrome (Hereditary Nonpolyposis Colorectal Carcinoma – HNPCC), an Autosomal Dominant disorder and is the most common form of hereditary colon cancer, accounting for 35% of the MSI colorectal cancers. MSI tumors tend to have better outcomes and this has been attributed to the abundance of tumor infiltrating lymphocytes in these tumors from increase immunogenicity. These tumors therefore are susceptible to PD-1 blockade with immune checkpoint inhibitors.
MSI (Micro Satellite Instability) testing is performed using a PCR based assay and MSI-High refers to instability at 2 or more of the 5 mononucleotide repeat markers and MSI-Low refers to instability at 1 of the 5 markers. Patients are considered Micro Satellite Stable (MSS) if no instability occurs. MSI-L and MSS are grouped together because MSI-L tumors are uncommon and behave similar to MSS tumors. Tumors considered MSI-H have deficiency of one or more of the DNA MisMatchRepair genes. MMR gene deficiency can be detected by ImmunoHistoChemistry (IHC). MLH1 gene is often lost in association with PMS2. NCCN Guidelines recommend MMR or MSI testing for all patients with a history of Colon or Rectal cancer.
This latest approval for OPDIVO® was based on results from the phase II CheckMate-142 trial, which is a multicenter, open label, single arm study, involving 53 patients with dMMR or MSI-H metastatic ColoRectal Cancer, who had disease progression during, after, or were intolerant to prior treatment with Fluoropyrimidine, Oxaliplatin, and Irinotecan-based chemotherapy. These 53 patients were a subset of the 74 patients who received at least one prior treatment regimen containing a Fluoropyrimidine with Oxaliplatin or Irinotecan for metastatic disease. All patients received OPDIVO® 3 mg/kg by intravenous infusion every 2 weeks until unacceptable toxicity or radiographic progression. The median age was 53 years. The Primary endpoint was Objective Response Rate (ORR) and exploratory endpoints included Safety, Progression Free Survival, Overall Survival and efficacy in biomarker-defined populations.
The Objective Response Rate as assessed by independent radiographic review committee, was 28% in the 53 patients who received prior Fluoropyrimidine, Oxaliplatin, and Irinotecan and responses lasted 6 months or more for the 67% of the responding patients. There was 1 complete response and 14 partial responses. The ORR was 32% among the 74 patients in the overall population. These responses and Clinical Benefit was seen regardless of PD-L1 expression, BRAF mutation status, KRAS mutation status, and clinical history of Lynch Syndrome. The most common adverse reactions related to OPDIVO® included fatigue, asthenia, rash, fever, nausea, diarrhea, musculoskeletal pain, cough and dyspnea.
The authors concluded that patients with metastatic ColoRectal Cancer who have dMMR or MSI-H tumors are less likely to respond to conventional chemotherapy and OPDIVO® demonstrated durable responses and disease control in this heavily pretreated patient group. Nivolumab in patients with DNA mismatch repair deficient/microsatellite instability high metastatic colorectal cancer: Update from CheckMate 142. Overman MJ, Lonardi S, Leone F, et al. J Clin Oncol 35, 2017 (suppl 4S; abstract 519).
Late Breaking Abstract - ASCO 2017: Three Months of Adjuvant Therapy Adequate for Stage III Colon Cancer Patients with T1-3, N1 Disease
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. Adjuvant chemotherapy for patients with resected, locally advanced, node-positive (stage III) colon cancer, has been the standard of care since 1990s. Adjuvant treatment with an ELOXATIN® (Oxaliplatin) based chemotherapy regimen has been considered standard intervention since 2004, for patients with stage III colon cancer following surgical resection and has been proven to decrease the chance of recurrent disease. Chemotherapy regimens have included (FOLFOX - Leucovorin, 5-FluoroUracil, ELOXATIN®) or CAPOX/XELOX (XELODA®/Capecitabine and ELOXATIN®/Oxaliplatin), given over a period of 6 months. ELOXATIN® can however be associated with neuropathy which can be long lasting or permanent, depending on the duration of therapy. Additional toxicities with longer duration of chemotherapy include diarrhea, fatigue as well as more office visits.
The IDEA Collaboration is a prospective, pre-planned pooled analysis of 6 concurrently conducted randomized phase III trials which included 12,834 patients from 12 countries. The goal of this study was to determine if 3 months of adjuvant chemotherapy would be as effective as 6 months of therapy and would be Non Inferior. Of the enrolled patients with Stage III disease, 13% had T1-2 disease, 66% had T3 disease, and 21% had T4 tumors. Twenty eight percent (28%) of the patients had N2 disease and 40% of the patients received XELOX chemotherapy. Approximately 60% had low-risk disease (T1-3, N1) and 40% had high-risk (T4 or N2). The primary endpoint was Disease Free Survival (DFS). The median follow up was 39 months.
It was noted that a shorter 3 month course of adjuvant chemotherapy was associated with a less than 1% lower risk of recurrence at 3 years compared to the standard 6 month course of therapy (74.6% versus 75.5%). In the subset of patients considered to be at low risk of cancer recurrence (1-3 positive lymph nodes and tumor not completely penetrating through the bowel wall), there was almost no difference in the DFS between a 3-month versus 6-month course of therapy (83.1% vs 83.3%). Even though Non Inferiority was not established for the overall cohort of patients, patients with stage T1-3 N1 disease showed Non Inferiority for 3 months versus 6 month course of adjuvant therapy. Further, 3 months of XELOX adjuvant therapy was Non Inferior to 6 months of ELOXATIN® based adjuvant therapy. Grade 2 or more neurotoxicity was significantly lower for patients who received 3 months of adjuvant therapy versus 6 months (P <0.0001), regardless of the treatment regimen (17% vs 48% for FOLFOX and 15% vs 45% for XELOX, respectively).
It was concluded by the IDEA collaboration that, a risk-based approach has to be taken when making adjuvant chemotherapy recommendations for patients with stage III colon cancer. Three months of adjuvant chemotherapy is adequate for patients with T1-3, N1 disease. For patients with T4 and/or N2 disease or other high risk factors, the duration of adjuvant therapy has to be determined based on patient preference, assessment of recurrent risk and tolerability. Prospective pooled analysis of six phase III trials investigating duration of adjuvant (adjuv) oxaliplatin-based therapy (3 vs 6 months) for patients (pts) with stage III colon cancer (CC): The IDEA (International Duration Evaluation of Adjuvant chemotherapy) collaboration. Shi Q, Sobrero AF, Shields AF, et al. J Clin Oncol 35, 2017 (suppl; abstr LBA1)
PET-CT in Colorectal Cancer Patients with a Rising CEA Can Detect Occult Recurrent Disease Amenable to Curative Therapy
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. Patients with ColoRectal Carcinoma are often followed up with regular CEA measurements after curative surgical resection and a rising CEA may be the first sign of CRC recurrence and warrants further investigation. Approximately 50% of the patients with early-stage disease after surgical resection will relapse with metastatic disease, during the first 3 years of follow-up. They may present with synchronous disease defined as distant metastases occurring within 6 months, and metachronous disease defined as distant metastases occuring beyond 6 months, of the primary diagnosis of CRC. These patients with oligo-metastatic disease, when detected early, may be potentially curable.
The authors in this study sought to (a) evaluate the utility of PET-CT in detecting occult disease recurrence in patients with raised CEA and (b) establish the prognostic effects of early detection of disease recurrence in patients with CRC. This retrospective analysis screened1200 patients from 2004 to 2010, with a confirmed diagnosis of CRC, who on follow up after curative therapy underwent FDG PET-CT imaging, for an elevated CEA, after normal findings on conventional investigations. Patients who had already received treatment with curative intent for synchronous or metachronous oligo-metastatic disease, including surgical resection, radiofrequency ablation (RFA), and radical chemoradiation, were also included. An elevated CEA level was defined as more than 3 ng/mL in nonsmokers and more than 5 ng/mL in smokers. A minimum of clinical and radiological follow up for 12 months or histopathological confirmation, were required, to ascertain recurrent disease. Eighty eight (N=88) patients who underwent PET-CT imaging because of any clinical indication and met the eligibility criteria, were included in the study. The mean age of patients was 66 years and 59% were male.
Recurrent disease was confirmed in 64% of the patients within the 12 months after their FDG PET-CT scan and the PET scan was able to detect the site of subtle relapse. The sensitivity of PET-CT to detect recurrence was 88% and the specificity was 88% as well. Fifty five percent (55%) of the patients with PET-CT-detected relapsed disease were deemed eligible for further curative therapy of whom 70% went on to receive potentially curative therapy. The Positive Predictive Value and Negative Predictive Value for FDG PET-CT to predict recurrence were 93% and 80% respectively.
The median Time To Progression for patients who received potentially curative therapy for the PET-CT-detected recurrence was 8.8 months versus 2.2 months for the patients not treated with curative intent. The median Overall Survival was 39.9 months for those who received potentially curative treatment versus 15.6 months for those who did not receive curative therapy. The 5-year survival rate in the curative group was 36.8% versus 6.1% in the non-curative group (P <0.001).
The authors concluded that early use of FDG PET-CT in patients with rising CEA levels is a highly sensitive and specific tool for the detection of occult ColoRectal Cancer recurrence, and in more than 50% of these patients, recurrent disease may still be amenable to curative therapy, and long-term survival can be achieved in a subgroup of this patient population. Survival Outcomes in Asymptomatic Patients With Normal Conventional Imaging but Raised Carcinoembryonic Antigen Levels in Colorectal Cancer Following Positron Emission Tomography-Computed Tomography Imaging. Khana K, Athaudaa A, Aitken K, et al. The Oncologist 2016;21:1502-1508
Location of Primary Tumor in the Colon Predicts Survival and Choice of Treatment in Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. Several published studies have demonstrated a nearly 20% reduced risk of death for patients diagnosed with left sided colon cancer compared with those who had right sided tumors. Venook and colleagues had previously presented their findings from a retrospective evaluation of the phase III 80405 clinical trial which included data from 1,025 metastatic ColoRectal Cancer patients with KRAS wild-type disease. The researchers assessed the impact of tumor location on Overall and Progression Free Survival in this group of patients. The median age was 59 yrs and 293 patients had a right-sided primary tumor (location in the cecum to hepatic flexure) and 732 patients had a left-sided primary tumor (location in the splenic flexure to rectum). It was noted that patients with tumors originating in the right side of the colon had much shorter median Overall Survival (19.4 months) compared to patients with left-sided tumors (33.3 months), (HR=1.60; P<0.001), with a 14 month survival improvement in the left versus right-sided primary tumors, for patients with metastatic disease. Tumor location in the colon also had a bearing on response to ERBITUX® (Cetuximab) and AVASTIN® (Bevacizumab). For the patient group who received ERBITUX®, the median Overall Survival (OS) was 36 months for patients with left-sided tumors but only 16.7 months for patients with right-sided tumors. For those who received AVASTIN®, the median OS was 31.4 months for patients with left-sided tumors and 24.2 months for those with right-sided tumors. The median Progression Free Survival was also influenced by the site of the primary tumor and was 11.5 months for left-sided tumors versus 8.9 months for right-sided tumors in the overall cohort of patients (HR = 1.26; P = 0.002). It was concluded that the biology of tumors originating in the right colon may be different from those originating in the left colon and regardless of KRAS mutational status, AVASTIN® based, first line chemotherapy regimen should be considered, for all patients with metastatic colorectal cancer, with a right-sided colon primary tumor and ERBITUX® should be avoided in this patient group.
Understanding that there is a difference in outcomes with biologic therapy, based on tumor location in the colon, the authors in this study evaluated the molecular variations of tumors arising in different parts of the left colon. Using protein expression, gene amplification and NextGen sequencing, 1,457 primary tumors (125 from splenic flexure to descending colon, 460 in the sigmoid colon and 872 in the rectum) were examined. MicroSatellite Instability (MSI) was measured by PCR and tumor mutational load was calculated using somatic nonsynonymous missense mutations.
They noted that the incidence of to MSI significantly decreased from right colon (22%), to descending colon (7%),sigmoid colon (4%) to rectum (1%) and this was statistically significant (P=0.01). Rectal tumors had a higher frequency of TP53 and APC gene mutations and higher expression of TOPO1, ERCC1 and MGMT, compared to tumors in the descending colon. Compared to sigmoid colon tumors, rectal tumors had a higher expression of TOPO1, MGMT, TLE3 and TUBB3.
The authors concluded that tumors arising in the rectum have a distinct set of genetic alterations compared with other left colon tumors, and these distinct biologic entities may need to be addressed with individually tailored therapy. Molecular variances between rectal and left-sided colon cancers. Marshall J, Lenz H, Xiu J, et al. J Clin Oncol 35, 2017 (suppl 4S; abstract 522)
Dual Inhibition Improves Outcomes for Patients with BRAF-Mutated Colorectal Tumors
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. The DNA MisMatchRepair (MMR) system is responsible for molecular surveillance and works as an editing tool that identifies errors within the microsatellite regions of DNA and removes them. Defective MMR system leads to MSI (Micro Satellite Instability) and hypermutation, triggering an enhanced antitumor immune response. MSI (Micro Satellite Instability) is therefore a hallmark of defective/deficient DNA MisMatchRepair (MMR) system and occurs in 15% of all colorectal cancers. Defective MisMatchRepair can be a sporadic or heritable event. Approximately 65% of the MSI tumors are sporadic and MSI-High tumors tend to have better outcomes. Patients with stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations. KRAS mutations are predictive of resistance to Epidermal Growth Factor Receptor (EGFR) targeted therapy. Approximately 5-10% of all metastatic CRC tumors present with BRAF V600 mutations and BRAF V600 is recognized as a marker of poor prognosis in this patient group. These patients tend to have aggressive disease with a higher rate of peritoneal metastasis and do not respond well to standard treatment intervention. Approximately 25% of the BRAF-mutated population in the metastatic setting has MSI-High tumors, but MSI-High status does not confer protection to this patient group.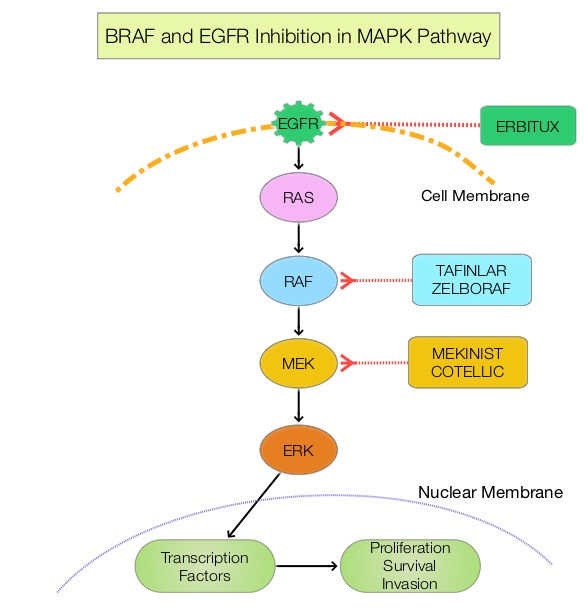
The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. The BRAF V600 mutations results in constitutive activation of the MAP kinase pathway. Inhibiting BRAF can transiently reduce MAP kinase signaling. However, this can result in feedback upregulation of EGFR signaling pathway, which can then reactivate the MAP kinase pathway. This aberrant signaling can be blocked by dual inhibition of both BRAF and EGFR.
ZELBORAF® (Vemurafenib), is a selective oral inhibitor of mutated BRAF whereas ERBITUX® (Cetuximab) is a monoclonal antibody targeting Epidermal Growth Factor Receptor (EGFR). Preclinical studies have shown that adding CAMPTOSAR® (Irinotecan) to ZELBORAF® and ERBITUX®, in patients with refractory BRAF V600E metastatic CRC, led to a durable responses and this combination was safe and tolerable. However, both single agent ZELBORAF® and ERBITUX® were shown to have limited activity in this patient group.
Based on this scientific rationale, a phase II trial was conducted (SWOG 1406), in which 106 metastatic ColoRectal Cancer patients, with mutations in BRAF V600 and extended RAS wild-type, were enrolled. Patients were randomized to receive CAMPTOSAR® 180 mg/m2 IV every 14 days and ERBITUX® 500 mg/m2 IV every 14 days, with or without ZELBORAF® 960 mg orally twice daily. The median age was 62 years and about 50% of patients had received 1 prior regimen for metastatic or locally advanced unresectable metastatic CRC, and 39% had received prior treatment with CAMPTOSAR® . Prior therapy with anti-EGFR agent or RAF or MEK inhibitors was not allowed. Crossover from the control arm to the experimental group was allowed, after documented disease progression. The primary endpoint was Progression Free Survival.
The median Progression Free Survival was 4.4 months with the triplet, versus 2.0 months with CAMPTOSAR® plus ERBITUX® (HR=0.42; P =0.0002). The response rate was 16% versus 4%, and the Disease Control Rate was 67% versus 22% (P =0.001), with a higher Duration of Response with the addition of ZELBORAF® to CAMPTOSAR® and ERBITUX® (Triplet). Approximately 50% of the patients in the control group crossed over to the experimental group at the time of disease progression. Overall Survival data and efficacy at cross-over, data, remain immature. Patients in the experimental group (Triplet group) experienced more grade 3/4 toxicities such as neutropenia, anemia and nausea, and this increase was attributed to increased duration of exposure to therapy.
The authors concluded that the addition of ZELBORAF® to the combination of CAMPTOSAR® and ERBITUX® resulted in a 58% reduction in the risk of disease progression and a higher Disease Control Rate, suggesting that simultaneous EGFR and BRAF inhibition (Dual Inhibition) is effective in BRAF V600 mutated ColoRectal Cancer. Subgroup analysis will examine the role of CAMPTOSAR® pre-treatment and the outcomes of patients based on tumor MicroSatellite Instability. Randomized trial of irinotecan and cetuximab with or without vemurafenib in BRAF-mutant metastatic colorectal cancer (SWOG 1406). Kopetz S, McDonough SL, Morris VK, et al. J Clin Oncol 35, 2017 (suppl 4S; abstract 520)
Influence of Tumor Genetics (MSI) on Prognostic Effect of BRAF and KRAS Mutations in Patients with Colon Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,000 new cases of ColoRectal Cancer will be diagnosed in the United States in 2016 and over 49,000 patients are expected to die of the disease. The role of adjuvant chemotherapy in patients with Stage III ColoRectalCancer (CRC) has been well established, with improvement in Disease Free Survival (DFS) and Overall Survival (OS). However, not all patients equally benefit from this therapy. Patients with MSI (Micro Satellite Instability) tumor phenotype have better survival when cancer is at an earlier stage although this beneficial effect in Stage III colon cancer remains unclear.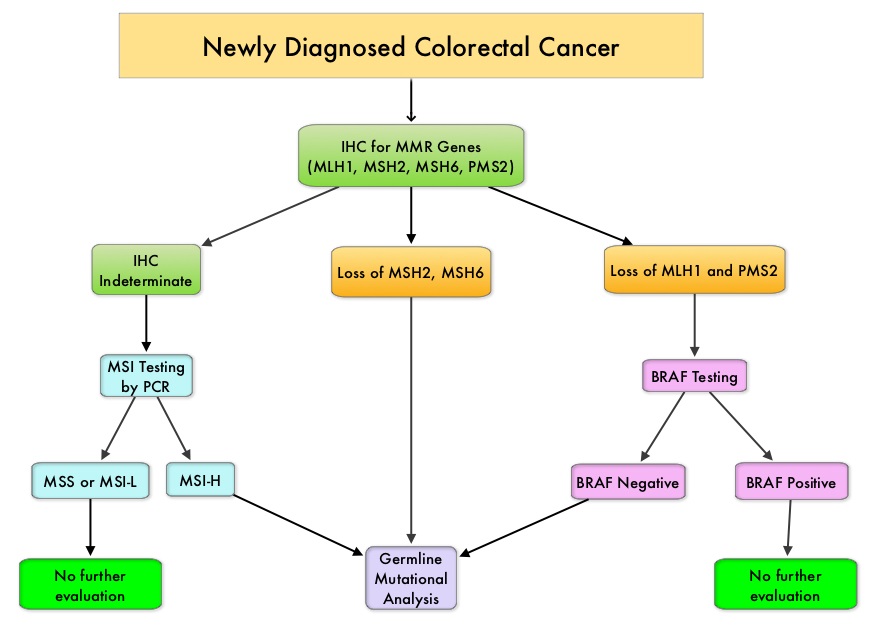
The DNA MisMatchRepair (MMR) system is responsible for molecular surveillance and works as an editing tool that identifies errors within the microsatellite regions of DNA and removes them. Defective MMR system leads to MSI (Micro Satellite Instability) and hypermutation, triggering an enhanced antitumor immune response. MSI (Micro Satellite Instability) is therefore a hallmark of defective/deficient DNA MisMatchRepair (MMR) system and occurs in 15% of all colorectal cancers. Defective MisMatchRepair can be a sporadic or heritable event. Approximately 65% of the MSI tumors are sporadic and when sporadic, the DNA MisMatchRepair gene is MLH1. Defective MisMatchRepair can also manifest as a germline mutation occurring in 1 of the 4 MisMatchRepair genes which include MLH1, MSH2, MSH6, PMS2. This produces Lynch Syndrome (Hereditary Nonpolyposis Colorectal Carcinoma – HNPCC), an autosomal dominant disorder and is the most common form of hereditary colon cancer, accounting for 35% of the MSI colorectal cancers. MSI tumors tend to have better outcomes and this has been attributed to the abundance of tumor infiltrating lymphocytes in these tumors from increase immunogenicity. These tumors are susceptible to PD-1 blockade and respond to treatment with checkpoint inhibitors such as Pembrolizumab (N Engl J Med 372:2509-2520, 2015).
MSI (Micro Satellite Instability) testing is performed using a PCR based assay and MSI-High refers to instability at 2 or more of the 5 mononucleotide repeat markers and MSI-Low refers to instability at 1 of the 5 markers. Patients are considered Micro Satellite Stable (MSS) if no instability occurs. MSI-L and MSS are grouped together because MSI-L tumors are uncommon and behave similar to MSS tumors. Tumors considered MSI-H have deficiency of one or more of the DNA MisMatchRepair genes. MMR gene deficiency can be detected by ImmunoHistoChemistry (IHC). MLH1 gene is often lost in association with PMS2.
Patients with stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations because KRAS mutations are predictive of resistance to EGFR targeted therapy and BRAF V600E is recognized as a marker of poor prognosis in this patient group. BRAF mutations occur in approximately 45% of patients with sporadic colorectal cancer with MSI but not seen in patients with Lynch syndrome. The prognostic effect of these mutations in early stage disease has however remained controversial. This publication is a Post Hoc Analysis of the PETACC-8 study, a randomized phase III trial, in which patients with resected Stage III colon cancer received treatment with adjuvant FOLFOX with or without Cetuximab. The authors in this publication examined the prognostic effect of BRAF and KRAS mutations in this patient population, as it relates to MSI of the tumor.
The PETACC-8 trial enrolled 2559 patients with surgically resected colon cancer, treated with adjuvant FOLFOX chemotherapy regimen. The median age was 60 years. MisMatch Repair, BRAF V600E, and KRAS exon 2 mutational status, were determined on tumor blocks that were collected prospectively from the enrolled patients. MSI phenotype was noted in 9.9% (N=177), KRAS mutations in 33.1% (N=588) and BRAF V600E mutations in 9% (N=148) of the patients. The primary end point was Disease Free Survival (DFS) and Overall Survival (OS), as it relates to these mutations.
In multivariate analysis, MSI and BRAF V600E mutations for DFS were not prognostic, whereas KRAS mutation was associated with significantly shorter DFS (P<0.001) and OS (P=0.008). The subgroup analysis showed that in patients with Micro Satellite Stable (MSS) tumors, DFS and OS was inferior among those with KRAS and BRAF V600E mutation and were independently associated with worse clinical outcomes. In patients with MSI tumors, KRAS status was not prognostic, whereas BRAF V600E mutation was associated with significantly longer DFS (P=0.04), but not OS (P=0.08).
The authors based on this large analysis of patients with Stage III colon cancer receiving FOFOX adjuvant chemotherapy, concluded that BRAF V600E and KRAS mutations were significantly associated with shorter DFS and OS in patients with Micro Satellite Stable (MSS) tumors, but not in patients with MSI tumors. Prognostic Effect of BRAF and KRAS Mutations in Patients With Stage III Colon Cancer Treated With Leucovorin, Fluorouracil, and Oxaliplatin With or Without Cetuximab. A Post Hoc Analysis of the PETACC-8 Trial. Taieb J, Zaanan A, Le Malicot, et al. JAMA Oncol. 2016;2:643-653.
Location of Primary Tumor Predicts Survival and Choice of Treatment in Metastatic Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,000 new cases of ColoRectal Cancer will be diagnosed in the United States in 2016 and over 49,000 patients are expected to die of the disease. Even though prognosis for patients with Colon Cancer has improved over the past two to three decades, it has remained unclear if improvement in survival was greater for left sided Colon Cancer versus cancer originating in the Right hemicolon.
Venook and colleagues had previously presented data from the primary analysis of a phase III CALGB/SWOG 80405 study which compared AVASTIN®: (Bevacizumab) or ERBITUX® (Cetuximab), given in conjunction with FOLFOX (Leucovorin, 5-Fluorouracil, Oxaliplatin) or FOLFIRI (Leucovorin, 5-FU, Irinotecan), as first line treatment of metastatic colorectal cancer. This study showed that chemotherapy plus ERBITUX® resulted in similar Overall Survival (29.9 months) as chemotherapy plus AVASTIN® (29 months) as well as Progression Free Survival (PFS). The present publication is a retrospective evaluation from the phase III 80405 clinical trial which included data from 1,025 patients with KRAS wild-type disease. The researchers assessed the impact of tumor location on Overall and PFS in this group of patients. The median age was 59 yrs and 293 patients had a right-sided primary tumor (location in the cecum to hepatic flexure) and 732 patients had a left-sided primary tumor (location in the splenic flexure to rectum).
It was noted that patients with tumors originating in the right side of the colon had much shorter median Overall Survival (19.4 months) compared to patients with left-sided tumors (33.3 months), (HR=1.60; P<0.001), with a 14 month survival improvement in the left versus right-sided primary tumors, for patients with metastatic disease. Tumor location in the colon also had a bearing on response to ERBITUX® and AVASTIN®. For the patient group who received ERBITUX®, the median Overall Survival (OS) was 36 months for patients with left-sided tumors but 16.7 months for patients with right-sided tumors. For those who received AVASTIN®, the median OS was 31.4 months for patients with left-sided tumors and 24.2 months for those with right-sided tumors. The median PFS was also influenced by the site of the primary tumor and was 8.9 months for right-sided tumors versus 11.5 months for left-sided tumors in the overall cohort of patients (HR = 1.26; P = 0.002). In a separate analysis, the authors also evaluated data from an additional 213 patients in CALGB/SWOG 80405 study who harbored KRAS mutations. These patients were originally included in this study prior to knowledge that ERBITUX® only benefited KRAS wild-type tumors. In this group of patients, those with left-sided primary tumors again achieved a longer median OS (30.3 months) compared to 23.1 months, among patients with right-sided tumors.
It was concluded that the biology of tumors originating in the right colon may be different from those originating in the left colon with ERBITUX® showing superiority over AVASTIN® when combined with chemotherapy in KRAS wild-type patients with left-sided colon cancer, whereas patients with right-sided colon cancer appear to benefit more from AVASTIN® based chemotherapy regimen. Regardless of KRAS mutational status, AVASTIN® based, first line chemotherapy regimen should be considered, for all patients with metastatic colorectal cancer, with a right-sided primary tumor. Impact of primary (1º) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts) with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). Venook AP, Niedzwiecki D, Innocenti F, et al. J Clin Oncol 34, 2016 (suppl; abstr 3504)
Influence of MSI on Prognostic Effect of BRAF and KRAS Mutations in Patients with Stage III Colon Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,000 new cases of ColoRectal Cancer will be diagnosed in the United States in 2016 and over 49,000 patients are expected to die of the disease. The role of adjuvant chemotherapy in patients with Stage III ColoRectalCancer (CRC) has been well established, with improvement in Disease Free Survival (DFS) and Overall Survival (OS). However, not all patients equally benefit from this therapy. Patients with MSI (Micro Satellite Instability) tumor phenotype have better survival when cancer is at an earlier stage although this beneficial effect in Stage III colon cancer remains unclear.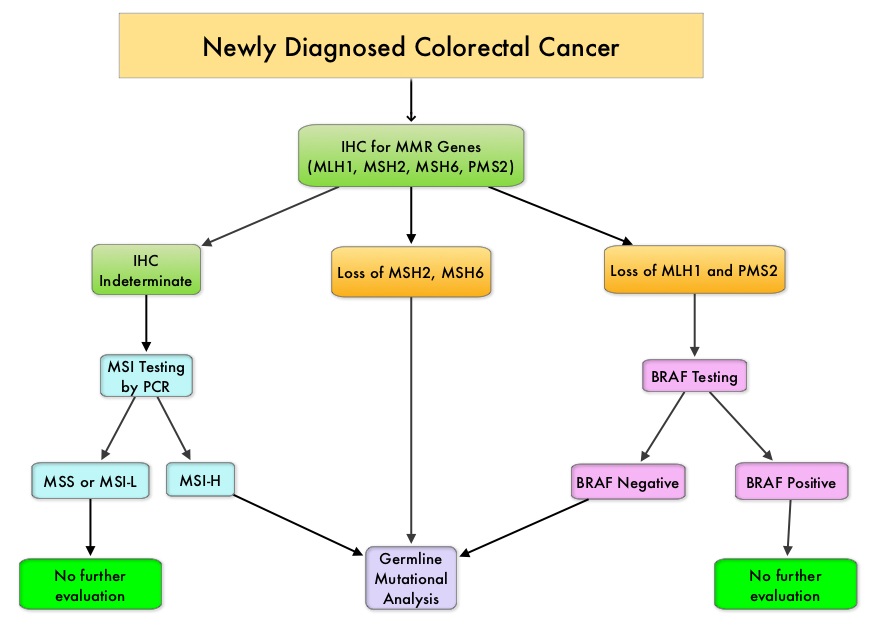
The DNA MisMatchRepair (MMR) system is responsible for molecular surveillance and works as an editing tool that identifies errors within the microsatellite regions of DNA and removes them. Defective MMR system leads to MSI (Micro Satellite Instability) and hypermutation, triggering an enhanced antitumor immune response. MSI (Micro Satellite Instability) is therefore a hallmark of defective/deficient DNA MisMatchRepair (MMR) system and occurs in 15% of all colorectal cancers. Defective MisMatchRepair can be a sporadic or heritable event. Approximately 65% of the MSI tumors are sporadic and when sporadic, the DNA MisMatchRepair gene is MLH1. Defective MisMatchRepair can also manifest as a germline mutation occurring in 1 of the 4 MisMatchRepair genes which include MLH1, MSH2, MSH6, PMS2. This produces Lynch Syndrome (Hereditary Nonpolyposis Colorectal Carcinoma – HNPCC), an autosomal dominant disorder and is the most common form of hereditary colon cancer, accounting for 35% of the MSI colorectal cancers. MSI tumors tend to have better outcomes and this has been attributed to the abundance of tumor infiltrating lymphocytes in these tumors from increase immunogenicity. MSI (Micro Satellite Instability) testing is performed using a PCR based assay and MSI-High refers to instability at 2 or more of the 5 mononucleotide repeat markers and MSI-Low refers to instability at 1 of the 5 markers. Patients are considered Micro Satellite Stable (MSS) if no instability occurs. MSI-L and MSS are grouped together because MSI-L tumors are uncommon and behave similar to MSS tumors. Tumors considered MSI-H have deficiency of one or more of the DNA MisMatchRepair genes. MMR gene deficiency can be detected by ImmunoHistoChemistry (IHC). MLH1 gene is often lost in association with PMS2.
Patients with stage IV colorectal cancer are now routinely analyzed for extended RAS and BRAF mutations because KRAS mutations are predictive of resistance to EGFR targeted therapy and BRAF V600E is recognized as a marker of poor prognosis in this patient group. BRAF mutations occur in approximately 45% of patients with sporadic colorectal cancer with MSI but not seen in patients with Lynch syndrome. The prognostic effect of these mutations in early stage disease has however remained controversial. This is a Post Hoc Analysis of the PETACC-8 study, a randomized phase III trial, in which patients with resected Stage III colon cancer received treatment with adjuvant FOLFOX with or without Cetuximab. The authors in this publication examined the prognostic effect of BRAF and KRAS mutations in this patient population, as it relates to MSI of the tumor.
The PETACC-8 trial enrolled 2559 patients with surgically resected colon cancer, treated with adjuvant FOLFOX chemotherapy regimen. The median age was 60 years. MisMatch Repair, BRAF V600E, and KRAS exon 2 mutational status, were determined on tumor blocks that were collected prospectively from the enrolled patients. MSI phenotype was noted in 9.9% (N=177), KRAS mutations in 33.1% (N=588) and BRAF V600E mutations in 9% (N=148) of the patients. The primary end point was Disease Free Survival (DFS) and Overall Survival (OS), as it relates to these mutations.
In multivariate analysis, MSI and BRAF V600E mutations for DFS were not prognostic, whereas KRAS mutation was associated with significantly shorter DFS (P<0.001) and OS (P=0.008). The subgroup analysis showed that in patients with Micro Satellite Stable (MSS) tumors, DFS and OS was inferior among those with KRAS and BRAF V600E mutation and were independently associated with worse clinical outcomes. In patients with MSI tumors, KRAS status was not prognostic, whereas BRAF V600E mutation was associated with significantly longer DFS (P=0.04), but not OS (P=0.08).
The authors based on this large analysis of patients with Stage III colon cancer receiving FOFOX adjuvant chemotherapy, concluded that BRAF V600E and KRAS mutations were significantly associated with shorter DFS and OS in patients with Micro Satellite Stable (MSS) tumors, but not in patients with MSI tumors. Prognostic Effect of BRAF and KRAS Mutations in Patients With Stage III Colon Cancer Treated With Leucovorin, Fluorouracil, and Oxaliplatin With or Without Cetuximab. A Post Hoc Analysis of the PETACC-8 Trial. Taieb J, Zaanan A, Le Malicot, et al. JAMA Oncol. 2016;2:643-653.
Daily Aspirin May Improve Survival after Diagnosis of Colorectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,000 new cases of ColoRectal Cancer will be diagnosed in the United States in 2016 and over 49,000 patients are expected to die of the disease. Several epidemiological studies as well as randomized controlled trials have shown that Aspirin and NonSteroidal Anti-Inflammatory Drugs (NSAIDs) reduce the incidence of ColoRectal Cancer (CRC) and CRC associated mortality. Nonetheless, use of aspirin for the primary prevention of CRC, is not routinely recommended, for the fear of aspirin-induced gastric and cerebral hemorrhages. Even though the benefits of Aspirin in the primary prevention of CRC remains well established, the role of Aspirin in secondary prevention in patients with CRC (after the diagnosis of CRC) is unclear. Platelets have long been implicated in the mechanism of tumor metastases. More recent data suggests that platelets may play a role in tumorigenesis as well, through the release of angiogenic and growth factors due to overexpression of COX-2. Daily low dose Aspirin inhibits COX-1 and COX-2. It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties.
Even though the benefits of Aspirin in the primary prevention of CRC remains well established, the role of Aspirin in secondary prevention in patients with CRC (after the diagnosis of CRC) is unclear. Platelets have long been implicated in the mechanism of tumor metastases. More recent data suggests that platelets may play a role in tumorigenesis as well, through the release of angiogenic and growth factors due to overexpression of COX-2. Daily low dose Aspirin inhibits COX-1 and COX-2. It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties.
The authors conducted this trial to evaluate the association between Aspirin use after diagnosis of CRC and CRC-Specific Survival (CSS) and Overall Survival (OS), in the largest group of patients ever studied. The study authors in this retrospective, population-based study identified 24,495 patients in the Cancer Registry of Norway, diagnosed with ColoRectal Cancer from 2004 through 2011 and a total of 23,162 patients diagnosed with CRC were included. Using the Norwegian Prescription Database, the authors were then able to establish that 6,102 patients in this large cohort had documented exposure to Aspirin. Exposure to Aspirin was defined as a prescription for more than 6 months of Aspirin, following a diagnosis of CRC. The median follow up was 3 years.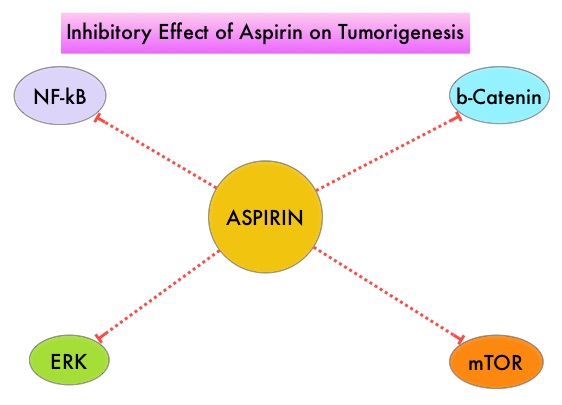
The authors performed a multivariate regression analysis controlling for age, gender, tumor stage, tumor differentiation and noted that exposure to Aspirin post-diagnosis, independently improved ColoRectal Cancer-Specific Survival (HR=0.85; P<0.001) and Overall Survival (HR=0.95; P<0.076). Patients who used Aspirin both before and after diagnosis of CRC had additional improvement in ColoRectal Cancer-Specific Survival (HR= 0.77; P<0.001) and Overall Survival (HR=0.86; P<0.001). Further, patients with poorly and moderately differentiated tumors experienced the greatest benefits of Aspirin exposure, as well as those with stage II disease. The researchers were also able to demonstrate that Aspirin use was most beneficial in the first 2 to 3 years after diagnosis.
It was concluded that Aspirin use after the diagnosis of ColoRectal Cancer, is independently associated with improved Colorectal Cancer-Specific Survival and Overall Survival. Because of the increased risk for bleeding, the risk-benefit should be assessed before Aspirin is routinely recommended to this patient population. Aspirin as Secondary Prevention in Patients With Colorectal Cancer: An Unselected Population-Based Study. Bains SJ, Mahic M, Myklebust TA, et al. Published online before print May 31, 2016, doi:10.1200/JCO.2015.65.3519JCO May 31, 2016 JCO653519
Left Sided Colon Cancer Patients Have Better Outcomes than Those with Right Sided Tumors
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,000 new cases of ColoRectal Cancer will be diagnosed in the United States in 2016 and over 49,000 patients are expected to die of the disease. Even though prognosis for patients with Colon Cancer has improved over the past two to three decades, it has remained unclear if improvement in survival was greater for Left sided Colon Cancer versus cancer originating in the Right hemicolon. To address this question, the authors in this study used the Geneva population-based registry and collected the data on all Colon Cancer patients from 1980-2006. They then compared outcomes ided Tumorsin 3396 patients with proximal (Right-sided) and distal (Left-sided) Colon Cancer. In the study population, 1,334 patients (39%) had Right-sided tumors and 2,062 (61%) had Left-sided tumors. Colon Cancer specific survival was then determined and compared, taking into consideration tumor and treatment characteristics of Left and Right sided tumors, as well as putative confounding variables. The authors also compared changes in survival between Colon Cancer location in early and late years of this observation study.
At the beginning of the study period (1980s), the 5-year specific survival was identical for Right and Left sided Colon Cancers (49% versus 48%). However, over the course of the study period, there was a marked improvement in survival, for patients with Left-sided cancers (HR=0.42; P<0.001), but this benefit was not noted in Right-sided Colon Cancer patients (HR=0.76; P=0.69). As such, distal Colon Cancer (Left sided) had a better prognosis than patients with proximal or Right sided Colon Cancer (Hazard Ratio for Left versus Right Colon Cancer = 0.81; P<0.001).
The authors concluded from this study that survival of patients with Right Colon Cancer did not improve since 1980, and tend to have the worse prognosis of all Colon Cancer patients. Therefore, change in treatment strategy is warranted for this patient subgroup. Right colon cancer: left behind. Gervaza P, Usel M, Rapiti E, et al. European Journal of Surgical Oncology 2016;doi:10.1016/j.ejso.2016.04.002
EGFR Inhibition may not be Effective Immediately after VEGF blockade in Metastatic ColoRectal Cancer
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,000 new cases of ColoRectal Cancer will be diagnosed in the United States in 2016 and over 49,000 patients are expected to die of the disease. Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable. Standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival (PFS) and Overall Survival (OS). The benefit with anti EGFR agents however is only demonstrable in patients with metastatic CRC, whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now becoming clear that even among the KRAS Wild Type patients, about 15% to 20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Therefore, pan RAS (expanded RAS) testing is now recommended.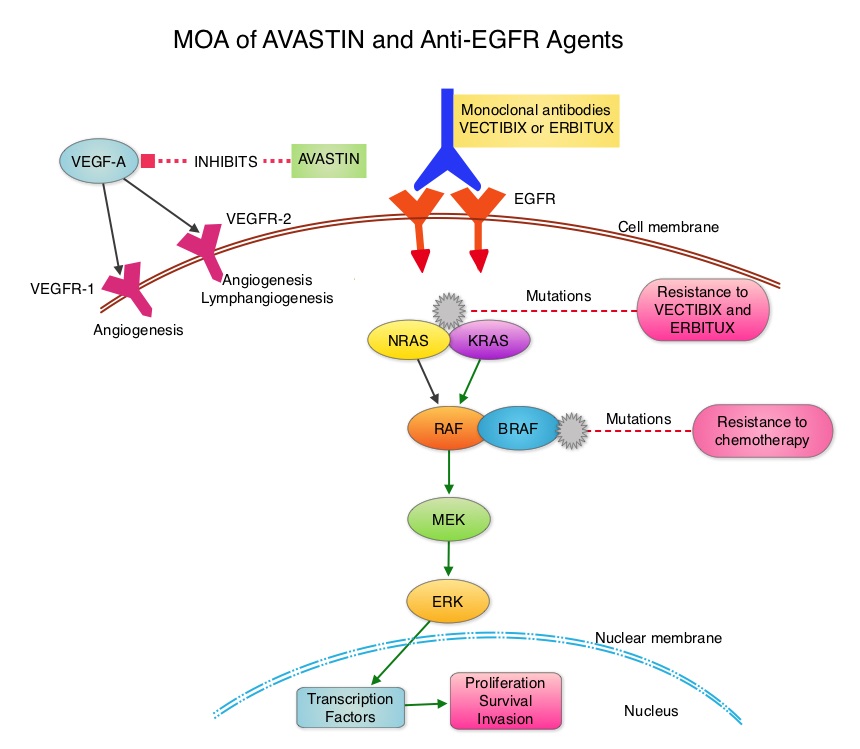
The CALGB/SWOG 80405 study reported that either ERBITUX® or AVASTIN® in combination with chemotherapy have equivalent Overall Survival benefit, when given as first line therapy, for patients with metastatic ColoRectal Cancer (mCRC), whose tumors are KRAS Wild Type. Consequently, the optimal first-line therapy for patients with KRAS Wild Type metastatic CRC still remains unclear. ERBITUX® has a similar activity across all treatment lines whereas AVASTIN® appears to lose its efficacy along the course of treatment lines. Although FOLFOX and FOLFIRI are equally effective as first line treatment for patients with metastatic CRC, FOLFOX might be more effective as second line treatment. Preclinical studies have suggested that a prior anti VEGF therapy, may lower sensitivity to a subsequent anti EGFR treatment.
The authors in a phase III randomized multicenter trial addressed these issues by comparing two different sequences of ERBITUX® and FOLFOX chemotherapy in KRAS Wild Type metastatic CRC patients, refractory to first line FOLFIRI chemotherapy and AVASTIN®. Patients with mCRC (N=110) were randomly assigned in a 1:1 ratio to receive CAMPTOSAR® (Irinotecan)/ERBITUX® as second line followed by FOLFOX-4 chemotherapy as third line (Arm A) or the reverse sequence (FOLFOX-4 chemotherapy second line followed by CAMPTOSAR®/ERBITUX® as third line - Arm B). The primary endpoint was Progression Free Survival (PFS) and secondary endpoints included Overall Survival (OS) and toxicity. It was noted that the median PFS in Arm A was 9.9 months compared to 11.3 months in Arm B (HR=0.85; P=0.42) and the median OS was 12.3 months in Arm A and 18.6 months in Arm B (HR=0.79; P=0.28). The Objective Response Rate in Arm A was 37% and in Arm B was 57% (P=0.05). Treatment was well tolerated with a low incidence of serious adverse events.
It was concluded that EGFR inhibition is not active immediately after VEGF blockade and therefore ERBITUX® is less effective immediately after AVASTIN®. The sequence of biological agents appears to be more important than the first-line chemotherapy choice. In RAS Wild Type metastatic CRC patients progressing after a first line AVASTIN® based therapy, ERBITUX® should be given in the third line setting or should be considered in first line treatment regimen. Efficacy of cetuximab immediately after bevacizumab: A phase III multicenter trial comparing two different sequences of cetuximab and FOLFOX in K-Ras WT metastatic colorectal cancer patients refractory FOLFIRI/bevacizumab. Cascinu S, Zaniboni A, Lonardi S, et al. J Clin Oncol 34, 2016 (suppl 4S; abstr 632)
XELOX Adjuvant Chemotherapy Regimen Improves Overall Survival in Stage III Colorectal Cancer
SUMMARY: The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. Adjuvant chemotherapy for patients with resected locally advanced, node-positive (stage III) colon cancer has been the standard of care since 1990s with improved Overall Survival noted after 6 months of bolus schedule of 5-Fluouracil (5-FU) and Leucovorin. Subsequently, the Multicenter International Study of Oxaliplatin/5-Fluorouracil/Leucovorin in the Adjuvant Treatment of Colon Cancer (MOSAIC) and National Surgical Adjuvant Breast and Bowel Project (NSABP) C-07 trials showed that the addition of ELOXATIN® (Oxaliplatin) to infusional 5- FU and Leucovorin (FOLFOX) or bolus 5-FU and Leucovorin (FLOX) significantly prolonged 3 year Disease Free Survival (DFS) when given in an adjuvant setting, in patients with stage II or III colon cancer. However, there was no significant Overall Survival (OS) benefit noted in the NSABP C-07 study.
XELOXA or NO16968 is a multinational, open-label, randomized phase III study, which only enrolled patients with stage III disease. Patients (N=1886) were randomly assigned to receive a more convenient XELOX regimen (N=944) or 5-FU and Leucovorin (N=942). The later regimen was considered the standard therapy when this trial was designed.The XELOX regimen consisted of a ELOXATIN® 130 mg/m2 given as a 2-hour IV infusion on day 1 and XELODA® (Capecitabine) 1,000 mg/m2 PO twice daily on days 1 to 14, of a 3 week cycle, for a total of eight cycles. The 5-FU/Leucovorin regimens could be either the Mayo Clinic or Roswell Park regimens. The Mayo Clinic regimen consisted of Leucovorin 20 mg/m2 and 5-FU 425 mg/m2 IV push on days 1-5, repeated every 4 weeks, for a total of six cycles. The Roswell Park regimen consisted of Leucovorin 500 mg/m2 given as a 2-hour infusion and 5-FU 500 mg/m2 IV push at 1 hour after the start of the Leucovorin infusion, repeated every week for six weeks, followed by a 2 week rest period, for a total of four 8-week cycles. The primary end point of this study was Disease Free Survival (DFS). Secondary end points were Overall Survival (OS), Relapse Free Survival (RFS) and safety.
The 3 year DFS data was published in 2011 and it was then noted that the addition of ELOXATIN® to oral Fluoropyrimidine, XELODA® improved DFS (HR=0.80; P=0.0045), similar to the previously published MOSAIC and NSABP C-07 trials. The authors in this publication reported the final efficacy data and biomarker analysis from the NO16968 trial comparing bolus 5-FU and Leucovorin with XELODA® plus ELOXATIN® (XELOX) in resected stage III colon cancer. The 7 year DFS rates were 63% and 56% in the XELOX and 5-FU/Leucovorin groups respectively (HR=0.80; P=0.004). The Overall Survival rates after a median follow up of 7 years were 73% and 67% in the XELOX and 5-FU/Leucovorin groups respectively (HR=0.83; P=0.04). It was noted that in the 498 patients who consented to the biomarker analysis, low tumor expression of DihydroPyrimidine Dehydrogenase was predictive for efficacy with XELOX regimen. There was however no statistically significant associations noted between any tumor biomarker and outcomes in the 5-FU/Leucovorin groups.
The authors concluded that in patients with resected stage III colon cancer, XELOX significantly improved Overall Survival compared to 5-FU/Leucovorin regimens and should be considered a standard adjuvant treatment option for patients with stage III disease. Tumor DihydroPyrimidine Dehydrogenase expression may be a clinically relevant biomarker for XELOX efficacy, but will require further evaluation. Capecitabine Plus Oxaliplatin Compared With Fluorouracil/Folinic Acid As Adjuvant Therapy for Stage III Colon Cancer: Final Results of the NO16968 Randomized Controlled Phase III Trial.Schmoll HJ, Tabernero J, Maroun J, et al. J Clin Oncol. 2015;33:3733-3740
ASCO Recommends Extended RAS Gene Testing in Metastatic Colorectal Cancer
SUMMARY: The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness. Patients with metastatic CRC, whose disease has progressed after treatment with standard therapies, have limited therapeutic options available, to treat their disease. Even though the Epidermal Growth Factor Receptor (EGFR) has been reported to be over expressed in 50-85% of the ColoRectal tumors, the intensity of ImmunoHistoChemical staining of EGFR in these tumors is not predictive of treatment response with EGFR directed antibody therapy such as ERBITUX® (Cetuximab) and VECTIBIX® (Panitumumab) and EGFR ImmunoHistoChemical staining should therefore not be a part of testing. The most common RAS oncogenes in human cancer are HRAS, KRAS, and NRAS. Mutations in HRAS are not common in colon cancer whereas KRAS and NRAS mutations are seen in colon cancer and tend to be mutually exclusive. It is also known that mutations in BRAF gene, which is downstream from RAS, may confer poor prognosis in colon cancer, regardless of therapy. It is estimated that approximately 40% of mCRC tumors harbor KRAS mutations and several studies had shown that metastatic ColoRectal Cancer (mCRC) tumors of patients harboring mutations in codon 12 or 13 of exon 2 of the KRAS gene, do not benefit from therapy with monoclonal antibodies directed against EGFR, when used as monotherapy or combined with chemotherapy. More recent studies have shown that KRAS mutations outside of exon 2 and mutations in NRAS are also predictive of lack of benefit with EGFR directed therapy.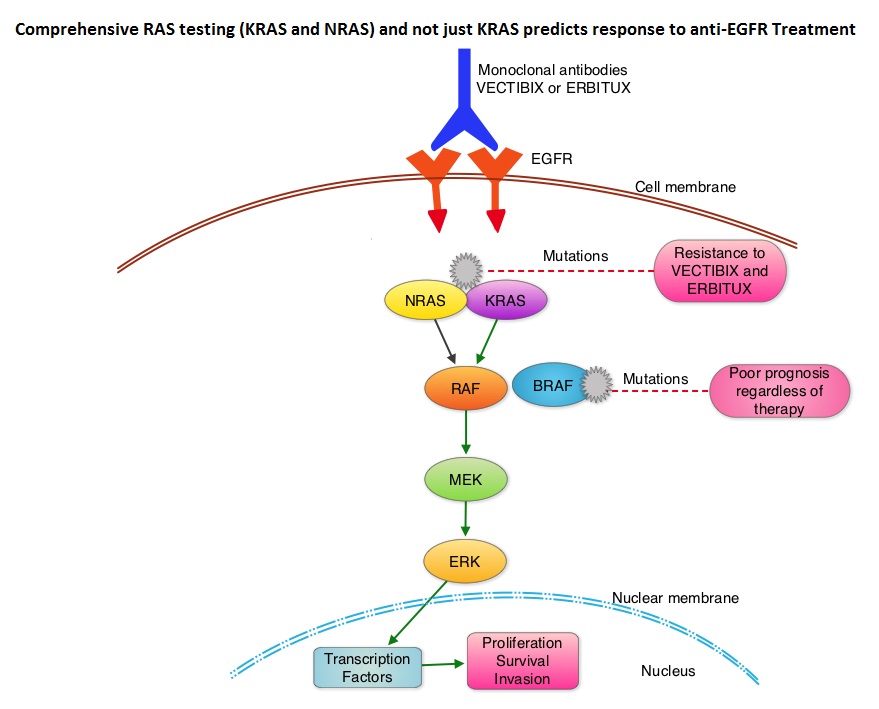
The American Society of Clinical Oncology Provisional Clinical Opinion (PCO) offers clinical direction for practicing oncology Health Care Providers, after publication or presentation of potentially practice-changing data from major studies. This 2015 ASCO Provisional Clinical Opinion update is a concerted effort of several organizations together with ASCO and they include the College of American Pathologists (CAP), the American Society for Clinical Pathology (ASCP), and the Association for Molecular Pathology (AMP). The Provisional Clinical Opinion (PCO) was released following inclusion of a systematic review of 11 meta-analyses, two retrospective analyses, and two health technology assessments in patients with mCRC. These studies evaluated the outcomes for patients with mCRC with no mutation detected or presence of mutation in additional exons in KRAS and NRAS. The extended RAS gene testing included
1) KRAS exons 2 (codons 12 and 13) exons 3 (codons 59 and 61) and exons 4 (codons 117 and 146)
2) NRAS exons 2 (codons 12 and 13), exons 3 (codons 59 and 61) and exons 4 (codons 117 and 146)
Two mCRC studies, the PRIME trial and the CRYSTAL trial, in their analysis included both KRAS and NRAS mutation data. In the PRIME study, the median Overall Survival (OS) in patients with wild-type RAS mCRC treated with VECTIBIX® plus FOLFOX was 26.0 months compared with 20.2 months with FOLFOX alone (HR=0.78; P=0.04). The Progression Free Survival (PFS) in patients not harboring RAS mutations was 10.1 months with VECTIBIX® plus FOLFOX, compared with 7.9 months with FOLFOX alone (HR=0.72; P=0.004). In the CRYSTAL trial, the median OS with ERBITUX® plus FOLFIRI was 28.4 months compared to 20.2 months with FOLFIRI alone, in patients with wild-type RAS mCRC (HR=0.69). The PFS in patients without RAS mutations was 11.4 months with ERBITUX® plus FOLFIRI compared with 8.4 months with FOLFIRI alone (HR, 0.56). Both these studies have shown that EGFR directed monoclonal antibody therapy does not benefit patients with KRAS or NRAS mutations and may even have a detrimental effect in these patients.
It was concluded that the current evidence indicates that EGFR directed therapy with monoclonal antibodies, ERBITUX® and VECTIBIX® should only be considered for treatment of patients with mCRC, whose tumors have no mutations detected after extended RAS mutation analysis. It is recommended that KRAS and NRAS genotyping of tumor should be performed at diagnosis of stage IV disease, as anti-EGFR directed therapy has no role in stage I, II or III disease. BRAF V600E mutation has been associated with poor prognosis in mCRC patients and may also predict lack of response to anti-EGFR monclonal antibody therapy, and should be a part of genotyping, at diagnosis of stage IV disease. Extended RAS Gene Mutation Testing in Metastatic Colorectal Carcinoma to Predict Response to Anti–Epidermal Growth Factor Receptor Monoclonal Antibody Therapy: American Society of Clinical Oncology Provisional Clinical Opinion Update 2015. Allegra CJ, Rumble RB, Hamilton SR, et al. Published online October 5, 2015. J Clin Oncol. doi: 10.1200/JCO.2015.63.9674.
FDA Approves LONSURF®, A Novel Oral Agent for Refractory Colorectal Cancer
SUMMARY: The FDA on September 22, 2015 approved LONSURF® (Trifluridine/Tipiracil) for the treatment of patients with metastatic ColoRectal Cancer (CRC), who have been previously treated with Fluoropyrimidine, Oxaliplatin and Irinotecan-based chemotherapy, an anti-VEGF biological therapy and if RAS wild-type, an anti-EGFR therapy. The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness. Patients with metastatic CRC, whose disease has progressed after treatment with standard therapies, have limited therapeutic options available, to treat their disease.
LONSURF® is a combination of two agents - a novel oral nucleoside, Trifluridine and a thymidine phosphorylase inhibitor, Tipiracil hydrochloride. This combination has a unique mechanism of action. Trifluridine, the active ingredient of LONSURF® incorporates into DNA resulting in DNA damage. Degradation of Trifluridine which occurs when taken orally is prevented by Tipiracil hydrochloride.
The RECOURSE study is a pivotal, global, phase III trial, in which 800 patients with metastatic ColoRectal Cancer, refractory to all standard therapies were randomly assigned in a 2:1 ratio to receive either LONSURF® (N=534) or placebo (N=266). Patients received LONSURF® 35mg/m2 or matching placebo orally, twice daily after meals, on Days 1-5 and 8-12 of each 28 day cycle. Treatment was continued until disease progression or unacceptable toxicity. Eligible patients had metastatic ColoRectal Cancer (mCRC), previously treated with chemotherapy and biological therapy, which included Fluoropyrimidine, Oxaliplatin and Irinotecan-based chemotherapy, an anti-VEGF biological therapy and if RAS wild-type, an anti-EGFR therapy. The primary endpoint of this study was overall survival and the secondary endpoint was progression-free survival.
It was noted that LONSURF® significantly improved Overall Survival compared to placebo (7.1 months vs 5.3 months; HR=0.68; P<0.001), with a 32% reduction in the risk of death. LONSURF® also significantly improved Progression Free Survival compared to placebo (HR = 0.47; P<0.001). The most common grade 3 or more adverse events were leukopenia (21%), anemia (18%) and febrile neutropenia (4%), noted in patients receiving LONSURF®. The authors concluded that LONSURF® significantly improved Overall Survival in patients with refractory metastatic ColoRectal Cancer, providing a novel oral therapeutic option for this patient group. Randomized Trial of TAS-102 for Refractory Metastatic Colorectal Cancer. Mayer RJ, Van Cutsem E, Falcone A, et al. N Engl J Med 2015; 372:1909-1919
NCCN Recommends Universal Screening for Lynch Syndrome in Patients with Newly Diagnosed Colorectal Cancer
SUMMARY: The American Cancer Society estimates that in the United States, for the year 2015, approximately 140,000 new cases of ColoRectal Cancer (CRC) will be diagnosed and close to 50,000 patients will die of the disease. The lifetime risk of developing ColoRectal Cancer is about 1 in 20 (5%). Lynch Syndrome (Hereditary NonPolyposis Colorectal Cancer - HNPCC), is an Autosomal Dominant, inherited disorder, associated with an increased risk of colorectal, endometrial, ovary, gastric, small bowel, pancreatic, brain, ureter or renal pelvis cancer. Approximately 3 to 5 percent of all cases of ColoRectal Cancer, are caused by Lynch Syndrome (LS) and 1 in 35 patients with newly diagnosed ColoRectal Cancer is related to Lynch Syndrome. Four MMR genes (MisMatch Repair genes), MLH1, MSH2, MSH6, and PMS2 are involved in the repair of mistakes that occur during DNA replication. When any of these genes are mutated, repair of DNA replication mistakes is prevented resulting in continuous division of abnormal cells and possibly cancer. The EPCAM gene lies next to the MSH2 gene on chromosome 2 and mutations in the EPCAM gene can cause the MSH2 gene to be inactivated, interrupting DNA repair and leading to accumulation of DNA replication errors and possible malignancy. Germline mutations in the MMR genes, is classically seen in Lynch Syndrome and results in microsatellite instability in tumors. Tumors are described as MSI-High when they have changes in 2 or more, of the 5 microsatellite markers. So, high levels of MSI within a tumor are suggestive of defective DNA mismatch repair. MSI-H is a hallmark of Lynch syndrome. However MSI-H is present in approximately 15% of patients with sporadic CRC. This is secondary to epigenetic silencing of MLH1 through promoter hypermethylation, rather than germline mutations in the MMR genes.
A Clinical Diagnosis of Lynch Syndrome can be made based on personal and family history if at least three relatives have a malignancy associated with Lynch Syndrome such as colorectal, endometrial, small bowel, ureter or renal pelvis cancer. In addition the following criteria should be met: • One relative must be a first-degree relative of the other two. • At least two successive generations must be affected. • At least one relative with a Lynch syndrome associated cancer should be diagnosed before 50 years of age. • Familial Adenomatous Polyposis should be excluded. • Tumors should be verified whenever possible. Because family history can sometimes be difficult to obtain or confirm, NCCN in those circumstances has recommended screening all newly diagnosed colorectal cancer patients for Lynch syndrome.
ImmunoHistoChemistry (IHC) staining can be performed on the tumor tissue for protein expression of the four MMR genes. IHC test is described as normal when all 4 mismatch repair proteins are normally expressed suggesting that an underlying mismatch repair gene mutation is unlikely. When IHC test is abnormal, it means that that at least one of the 4 mismatch repair proteins is not expressed and an inherited mutation may be present in the gene related to that protein. This can be further confirmed by mutation analysis of the corresponding gene. However, the lack of expression of MMR proteins by IHC is highly concordant with molecular MSI testing and IHC is therefore more practical and cost-effective. Tumors with loss of MMR protein expression or MSI-H are classified as MMR deficient (dMMR). Patients with sporadic tumors with MSI-H or MMR deficiency (dMMR) generally are older women with stage II disease and present with tumors in the proximal colon and the tumors are poor differentiated with increased number of tumor-infiltrating lymphocytes. These patients in retrospective studies had superior stage-adjusted survival compared to MMR proficient tumors. Further, single agent 5-Fluorouracil when given in an adjuvant setting was not beneficial in this patient group.
It should also be noted that a majority of colon cancer tumors that lack protein expression on IHC staining of MLH1 (often coexisting with loss of PMS2) are often due to an acquired genetic defect. If the IHC indicates absence of MLH1 protein expression, tumor should be tested for BRAF mutation V600E, which can be seen in sporadic colorectal cancers, but rarely found in patients who have Lynch Syndrome. Once a diagnosis of Lynch Syndrome is made, at risk family members should undergo colonoscopic evaluation at 20-25 years of age or 2-5 years prior to the earliest colon cancer, if it is diagnosed before age 25 and is repeated every 1-2 years. Prophylactic hysterectomy and bilateral salpingo-oophorectomy (BSO) should be considered by women who have completed childbearing. NCCN Guidelines Version 1.2014 Lynch Syndrome
Late Breaking Abstract-ASCO 2015: Treating Cancer Based on Genomics Regardless of Tumor Type
SUMMARY: KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti–PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of the Immune checkpoints. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions.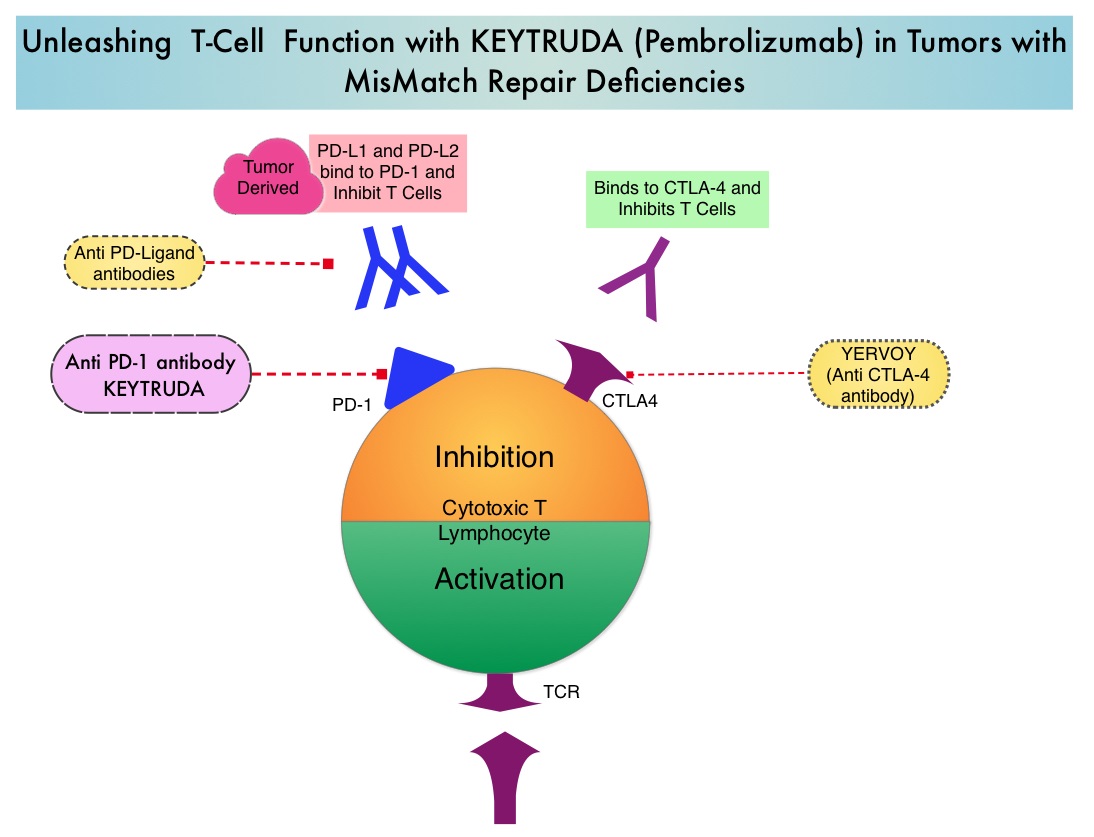 Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response.
Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response.
Somatic mutations are genetic alterations that can occur in any cell of the body except the germ cells (sperm and egg) and can be passed to the progeny of the mutated cell during cell division and can cause cancer or other diseases. Unlike germline mutations, which are inherited genetic alterations that occur in the germ cells (sperm and eggs), somatic mutations are not passed on to children. Based on previously published studies it was noted that 1) Somatic mutations found in tumors can be recognized by the patient’s own immune system, as they encode as “non-self” immunogenic antigens 2) Some patients with advanced colorectal cancers have tumors with MisMatch Repair-deficiency (MMR-deficiency) 3) Colorectal cancers with MMR-deficiency have many more somatic mutations compared to MMR-proficient colorectal cancers.
It was therefore hypothesized that MMR-deficient tumors would be more responsive to PD-1 blockade than MMR-proficient tumors. Based on this hypothesis, the authors conducted a phase II study to evaluate the clinical activity of KEYTRUDA® (Pembrolizumab), a PD-1 immune checkpoint inhibitor, in 41 previously treated patients with progressive metastatic carcinoma with or without MMR deficiency. Patients were divided into three cohorts and KEYTRUDA® was administered at a dose of 10 mg/kg IV every 14 days in patients with MMR-deficient colorectal cancers, patients with MMR-proficient colorectal cancers and patients with MMR-deficient non-colorectal cancer patients. The co-primary end points were the immune-related Objective Response Rate (irORR) and immune-related Progression Free Survival (irPFS) at 20 weeks. Immune-related criteria is one way of evaluating immune-based therapies and unlike Response Evaluation Criteria in Solid Tumors (RECIST), are based on radiographic responses and the tumor burden is measured based on newly developed lesions, detected on radiography. This study met its primary endpoints and the authors reported that the irORR and irPFS at 20 weeks for MMR-deficient colorectal cancers were 40% and 78%, respectively, and for MMR-deficient non-colorectal cancers were 71% and 67%, respectively. However, in the MMR-proficient colorectal cancer patients, the irORR and irPFS at 20 weeks were 0% and 11%, respectively. The median PFS and Overall Survival (OS) were not reached in the MMR-deficient colorectal cancer patient group but was 2.2 and 5.0 months in the MMR-proficient colorectal cancer patient group (HR for PFS=0.10; P< 0.001 and HR for OS=0.22; P=0.05). These positive outcomes in patients with MMR-deficient tumors correlated with a drop in the tumor markers such as CEA, if the levels were elevated at the time of enrollment. It was also noted that there were about 1,782 somatic mutations per MMR-deficient tumor compared to 73 in MMR-proficient tumors on whole exome sequencing (P=0.0015) and the high total somatic mutation loads were associated with improved PFS (P=0.02). The authors concluded that the tumor MisMatch Repair status predicts clinical benefit of immune checkpoint blockade with check point inhibitors such as KEYTRUDA® and this information may open the doors for the treatment of tumors based solely on genomics, regardless of tumor type. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. Le DT, M.D., Uram JN, Wang H, et al. N Engl J Med 2015; 372:2509-2520
ASCO 2015: Selective Internal Radiation Therapy with Y-90 Improves Outcomes in Metastatic Colorectal Cancer
SUMMARY: The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness. About 10-20% of the patients with liver metastases have resectable disease, which may translate into long term survival. CRC patients with synchronous metastases tend to have more extensive disease with bilobar liver involvement. With the availability of more effective chemotherapy regimens and targeted systemic interventions, the median survival of CRC patients with metastatic disease has increased from 6 months in the 1990’s to 24 months. Selective Internal Radiation Therapy (SIRT) or RadioEmbolization using radioisotope Yttrium-90 (Y-90) coated resin particles, a pure beta emitter, has demonstrated significant benefit for patients with unresectable liver metastases, in previously published studies. Y-90 resin microspheres are no bigger in diameter than a human hair and are introduced into the hepatic artery by initially accessing the femoral artery. The blood supply to the liver tumors is via the hepatic artery and these tumors tend to be hypervascular. The Y-90 resin microspheres become preferentially lodged in the narrow capillaries that surround liver tumors and selectively deliver a high dose of short-range beta radiation to the liver tumors. The physical properties of Y-90 resin microspheres facilitate even distribution of radioactivity within and around the liver metastases. SIRFLOX is an International, multi-center, open-label, randomized phase III study, which evaluated the efficacy and safety of combining modified FOLFOX6 (Oxaliplatin, 5-FU and Leucovorin) chemotherapy regimen with or without AVASTIN® (Bevacizumab) with SIRT, using Y-90 resin microspheres, as first line treatment in patients with unresectable liver only or liver dominant metastatic ColoRectal Cancer (mCRC). The randomization included 530 patients of whom 263 patients received mFOLFOX6 with or without AVASTIN® (Group A) and 267 patients received mFOLFOX6 + SIRT administered once with cycle 1, with or without AVASTIN® (Group B), with the treatment given until disease progression. Patients were stratified based on the extent of liver involvement (25% or less versus more than 25%), presence of extra hepatic disease (liver only versus liver dominant disease) and treatment with AVASTIN®, which was at the discretion of the attending physician. Forty percent of the patients had extra hepatic disease. The primary endpoint was Progression Free Survival (PFS). With a median follow up of 36.1 months, the median PFS in the liver was 12.6 months versus 20.5 months in Group A versus Group B respectively (HR=0.69; P=0.002). The hepatic Response Rate was 68.8% versus 78.7% (P=0.042), with a Complete Response Rate of 1.9% versus 6.0% (P=0.02) in Groups A and B respectively. Even though hematologic and gastrointestinal adverse events were higher in the SIRT group, the toxicity levels were acceptable. The authors concluded that the addition of SIRT to chemotherapy resulted in a 7.9 month improvement in Progression Free Survival in the liver, for patients with unresectable metastatic ColoRectal cancer (mCRC), with a 31% reduction in the risk of tumor progression in the liver. With the liver being the most common site of spread in patients with metastatic CRC, this study provides Level One evidence to support the use of SIRT in combination with chemotherapy in this patient group. SIRFLOX: Randomized phase III trial comparing first-line mFOLFOX6 ± bevacizumab (bev) versus mFOLFOX6 + selective internal radiation therapy (SIRT) ± bev in patients (pts) with metastatic colorectal cancer (mCRC). Gibbs P, Heinemann V, Sharma NK, et al. J Clin Oncol 33, 2015 (suppl; abstr 3502)
SIRFLOX is an International, multi-center, open-label, randomized phase III study, which evaluated the efficacy and safety of combining modified FOLFOX6 (Oxaliplatin, 5-FU and Leucovorin) chemotherapy regimen with or without AVASTIN® (Bevacizumab) with SIRT, using Y-90 resin microspheres, as first line treatment in patients with unresectable liver only or liver dominant metastatic ColoRectal Cancer (mCRC). The randomization included 530 patients of whom 263 patients received mFOLFOX6 with or without AVASTIN® (Group A) and 267 patients received mFOLFOX6 + SIRT administered once with cycle 1, with or without AVASTIN® (Group B), with the treatment given until disease progression. Patients were stratified based on the extent of liver involvement (25% or less versus more than 25%), presence of extra hepatic disease (liver only versus liver dominant disease) and treatment with AVASTIN®, which was at the discretion of the attending physician. Forty percent of the patients had extra hepatic disease. The primary endpoint was Progression Free Survival (PFS). With a median follow up of 36.1 months, the median PFS in the liver was 12.6 months versus 20.5 months in Group A versus Group B respectively (HR=0.69; P=0.002). The hepatic Response Rate was 68.8% versus 78.7% (P=0.042), with a Complete Response Rate of 1.9% versus 6.0% (P=0.02) in Groups A and B respectively. Even though hematologic and gastrointestinal adverse events were higher in the SIRT group, the toxicity levels were acceptable. The authors concluded that the addition of SIRT to chemotherapy resulted in a 7.9 month improvement in Progression Free Survival in the liver, for patients with unresectable metastatic ColoRectal cancer (mCRC), with a 31% reduction in the risk of tumor progression in the liver. With the liver being the most common site of spread in patients with metastatic CRC, this study provides Level One evidence to support the use of SIRT in combination with chemotherapy in this patient group. SIRFLOX: Randomized phase III trial comparing first-line mFOLFOX6 ± bevacizumab (bev) versus mFOLFOX6 + selective internal radiation therapy (SIRT) ± bev in patients (pts) with metastatic colorectal cancer (mCRC). Gibbs P, Heinemann V, Sharma NK, et al. J Clin Oncol 33, 2015 (suppl; abstr 3502)
Daily Aspirin May Improve Survival after Diagnosis of Colorectal Cancer
SUMMARY: The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. Several epidemiological studies as well as randomized controlled trials have shown that Aspirin reduces the incidence of ColoRectal Cancer (CRC) and CRC associated mortality. Platelets have long been implicated in the mechanism of tumor metastases. More recent data suggests that platelets may play a role in tumorigenesis as well, through the release of angiogenic and growth factors due to overexpression of COX-2. Daily low dose Aspirin inhibits COX-1 and COX-2. 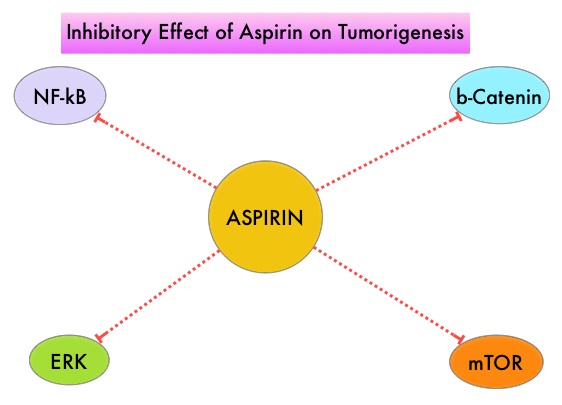 It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties. Even though the benefits of Aspirin in the primary prevention of CRC remains well established, the role of Aspirin in secondary prevention in patients with CRC is unclear. The authors conducted this trial to evaluate the association between Aspirin use after diagnosis of CRC with CRC-Specific Survival (CSS) and Overall Survival (OS) in the largest group of patients ever studied. The study authors in this retrospective study identified 25,644 patients in the Cancer Registry of Norway, diagnosed with ColoRectal Cancer (CRC) from 2004 through 2011. Using the Norwegian Prescription Database, the authors were then able to establish that 6,109 patients in this large cohort had documented exposure to Aspirin. Exposure to Aspirin was defined as a prescription for more than 6 months of Aspirin following a diagnosis of CRC. The median follow up was 2.2 years. The authors performed a multivariate regression analysis controlling for age, gender, tumor stage, tumor differentiation and noted that exposure to Aspirin post-diagnosis, independently improved ColoRectal Cancer (CRC) -Specific Survival (HR=0.75; P<0.001) and Overall Survival (HR=0.86; P<0.001). The authors concluded that in this large group of unselected ColoRectal Cancer (CRC) patients, exposure to Aspirin after the diagnosis of CRC is independently associated with improved Colorectal Cancer-Specific Survival and Overall Survival. They added that because of the risk of bleeding, the risk–benefit should be assessed before Aspirin is routinely recommended to this patient population. Impact of aspirin as secondary prevention in an unselected cohort of 25,644 patients with colorectal cancer: A population-based study. Bains S, Mahic M, Cvancarova M, et al. J Clin Oncol 33, 2015 (suppl; abstr 3504)
It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties. Even though the benefits of Aspirin in the primary prevention of CRC remains well established, the role of Aspirin in secondary prevention in patients with CRC is unclear. The authors conducted this trial to evaluate the association between Aspirin use after diagnosis of CRC with CRC-Specific Survival (CSS) and Overall Survival (OS) in the largest group of patients ever studied. The study authors in this retrospective study identified 25,644 patients in the Cancer Registry of Norway, diagnosed with ColoRectal Cancer (CRC) from 2004 through 2011. Using the Norwegian Prescription Database, the authors were then able to establish that 6,109 patients in this large cohort had documented exposure to Aspirin. Exposure to Aspirin was defined as a prescription for more than 6 months of Aspirin following a diagnosis of CRC. The median follow up was 2.2 years. The authors performed a multivariate regression analysis controlling for age, gender, tumor stage, tumor differentiation and noted that exposure to Aspirin post-diagnosis, independently improved ColoRectal Cancer (CRC) -Specific Survival (HR=0.75; P<0.001) and Overall Survival (HR=0.86; P<0.001). The authors concluded that in this large group of unselected ColoRectal Cancer (CRC) patients, exposure to Aspirin after the diagnosis of CRC is independently associated with improved Colorectal Cancer-Specific Survival and Overall Survival. They added that because of the risk of bleeding, the risk–benefit should be assessed before Aspirin is routinely recommended to this patient population. Impact of aspirin as secondary prevention in an unselected cohort of 25,644 patients with colorectal cancer: A population-based study. Bains S, Mahic M, Cvancarova M, et al. J Clin Oncol 33, 2015 (suppl; abstr 3504)
FDA Approves CYRAMZA® for Metastatic ColoRectal Cancer
SUMMARY: The FDA on April 24, 2015 approved CYRAMZA® for use in combination with FOLFIRI for the treatment of patients with metastatic ColoRectal Cancer (mCRC), whose disease has progressed on a first line AVASTIN® (Bevacizumab), ELOXATIN® (Oxaliplatin) and Fluoropyrimidine containing regimen. The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. With the availability of new active agents for the treatment of CRC, improving Overall Survival for patients with advanced disease, by prudently planning a treatment strategy and properly sequencing these agents, has become increasing relevant. 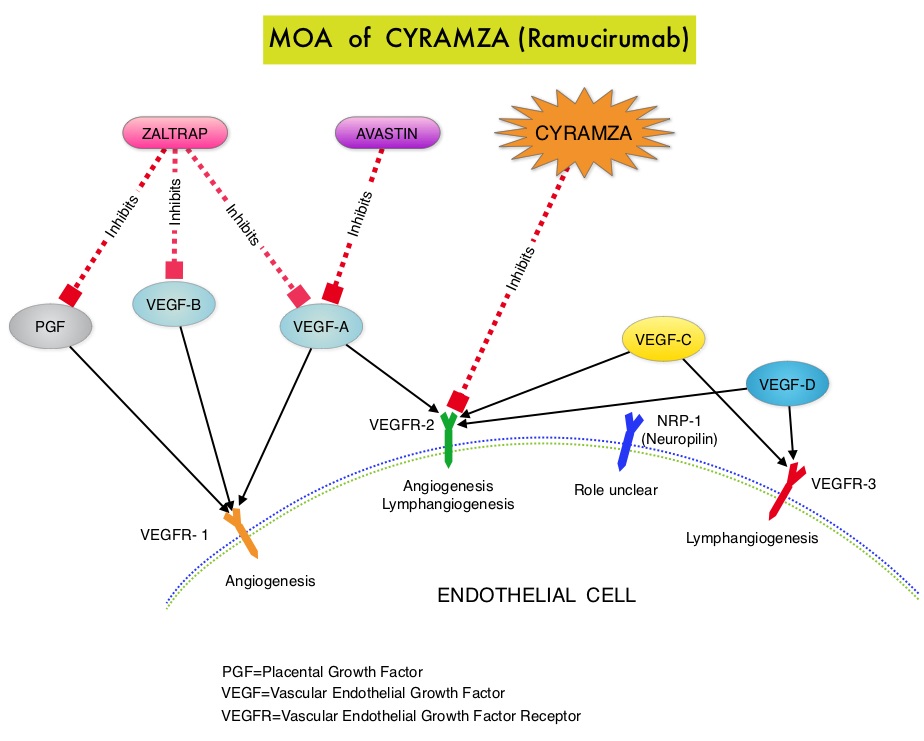 CYRAMZA® (Ramucirumab) is a recombinant human IgG1 monoclonal antibody that binds to Vascular Endothelial Growth Factor Receptor 2 (VEGFR-2) and blocks binding of the VEGFR ligands VEGF-A, VEGF-C, and VEGF-D and thus inhibits ligand-induced proliferation and migration of endothelial cells. This is unlike AVASTIN®, which inhibits VEGF-A. Several studies have demonstrated that continuing VEGF inhibition along with standard second-line chemotherapy beyond disease progression has a significant advantage, in patients with mCRC. Two observational studies (BRiTE and ARIES) as well as an open label phase III study have all shown improvement in median Overall Survival (OS) when AVASTIN® was continued beyond first progression and given along with second line chemotherapy. In the VELOUR trial, FOLFIRI in combination with ZALTRAP® (Aflibercept), a VEGF-A, VEGF-B and Placental Growth Factor inhibitor, when given as second line therapy for those patients with mCRC who had progressed on AVASTIN® plus ELOXATIN® containing regimen, resulted in a significant improvement in the median PFS and OS.
CYRAMZA® (Ramucirumab) is a recombinant human IgG1 monoclonal antibody that binds to Vascular Endothelial Growth Factor Receptor 2 (VEGFR-2) and blocks binding of the VEGFR ligands VEGF-A, VEGF-C, and VEGF-D and thus inhibits ligand-induced proliferation and migration of endothelial cells. This is unlike AVASTIN®, which inhibits VEGF-A. Several studies have demonstrated that continuing VEGF inhibition along with standard second-line chemotherapy beyond disease progression has a significant advantage, in patients with mCRC. Two observational studies (BRiTE and ARIES) as well as an open label phase III study have all shown improvement in median Overall Survival (OS) when AVASTIN® was continued beyond first progression and given along with second line chemotherapy. In the VELOUR trial, FOLFIRI in combination with ZALTRAP® (Aflibercept), a VEGF-A, VEGF-B and Placental Growth Factor inhibitor, when given as second line therapy for those patients with mCRC who had progressed on AVASTIN® plus ELOXATIN® containing regimen, resulted in a significant improvement in the median PFS and OS.
The RAISE trial is a double-blind, phase III study in which 1072 patients with mCRC who progressed on or after first-line treatment with AVASTIN®, ELOXATIN® and a Fluoropyrimidine were randomized to receive FOLFIRI given along with antiangiogenic agent CYRAMZA® (N = 536) or placebo (N = 536), every 2 weeks. The FOLFIRI regimen consisted of CAMPTOSAR® (Irinotecan) 180 mg/m2 IV, Folinic Acid 400 mg/m2 IV and 5-FU 400 mg/m2 IV bolus followed by 5-FU 2400 mg/m2 continuous IV infusion over 46 to 48 hours. CYRAMZA® was administered at a dose of 8 mg/kg IV every 2 weeks. The median age of patients was 62 years, about 50% harbored KRAS mutations and 99% of the patients had an ECOG performance status of 0 or 1. Treatment was continued until disease progression or unacceptable toxicity. The primary endpoint of the study was Overall Survival (OS) and secondary endpoints included Progression Free Survival (PFS), Objective Response Rate (ORR) and toxicity. There was a statistically significant Overall Survival improvement in patients receiving FOLFIRI plus CYRAMZA® compared to those receiving FOLFIRI plus placebo with a median OS of 13.3 and 11.7 months for patients on the FOLFIRI plus CYRAMZA® and FOLFIRI plus placebo arms, respectively (HR=0.85; P=0.023). The median PFS with FOLFIRI and CYRAMZA® was 5.7 months versus 4.5 months with FOLFIRI and placebo (HR= 0.79; P=0.001). There was no statistically significant difference in Objective Response Rate noted in the two treatment groups. Compared to the placebo group, more patients receiving CYRAMZA®, experienced grade 3 or more adverse events such as neutropenia (38.4% vs 23.3%) and hypertension (10.8% vs 2.8%). Other adverse events associated with CYRAMZA® included hemorrhage (43.9% vs 22.7% with placebo) and proteinuria (17% vs 4.5% with placebo). The authors concluded that CYRAMZA® is a new treatment option for second line treatment of patients with metastatic ColoRectal Cancer, including those with KRAS mutations. Tabernero J, Cohn AL, Obermannova R, et al. RAISE: A randomized, double-blind, multicenter phase III study of irinotecan, folinic acid, and 5-fluorouracil (FOLFIRI) plus ramucirumab (RAM) or placebo (PBO) in patients (pts) with metastatic colorectal carcinoma (CRC) progressive during or following first-line combination therapy with bevacizumab (bev), oxaliplatin (ox), and a fluoropyrimidine (fp). 2015 Gastrointestinal Cancers Symposium; January 15-17, 2015; San Francisco, CA. Abstract 512.
Higher Serum Vitamin D Levels May Improve Survival in Patients with Advanced Colon Cancer
SUMMARY: The American Cancer Society estimates that approximately 133,000 new cases of colorectal cancer will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. There is a growing body of evidence suggesting that Vitamin D has colon cancer preventing properties and may induce antitumor immunity. A recent study by Song and colleagues (Gut. 2015;64:260-271) showed that high plasma level 25-Hydroxy Vitamin D [25(OH)D] was associated with lower risk of colorectal cancer with intense immune reaction, supporting that vitamin D through tumor-host interaction may play a role in cancer immunoprevention. 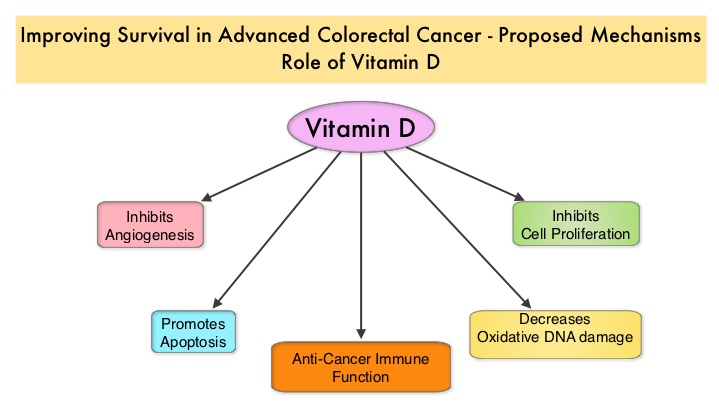 There appears to be a strong association between plasma 25(OH)D level and colorectal cancer (CRC) specific mortality, with better outcomes in patients with Stage I-III CRC, who had higher plasma levels of 25(OH)D (Zgaga L, et al. J Clin Oncol 2014;32:2430-2439). The researchers in this present study conducted a prospective analysis of data from CALGB 80405 trial and evaluated the relationship between plasma 25(OH)D level and patient outcomes, which included Overall Survival and Progression Free Survival (PFS). CALGB 80405 is a phase III trial in which patients with newly diagnosed, advanced colorectal cancer were initially randomized to three groups- 1) Chemotherapy (FOLFIRI or mFOLFOX6) with ERBITUX® (Cetuximab) 2) Chemotherapy with AVASTIN® (Bevacizumab) 3) Chemotherapy with ERBITUX® and AVASTIN®. The protocol was later amended to only include patients with KRAS Wild Type tumors and the chemotherapy with ERBITUX® and AVASTIN® group was deleted. This trial was not designed to compare chemotherapy regimens. The Overall Survival (OS) in both the treatment groups were similar at 29+ months.
There appears to be a strong association between plasma 25(OH)D level and colorectal cancer (CRC) specific mortality, with better outcomes in patients with Stage I-III CRC, who had higher plasma levels of 25(OH)D (Zgaga L, et al. J Clin Oncol 2014;32:2430-2439). The researchers in this present study conducted a prospective analysis of data from CALGB 80405 trial and evaluated the relationship between plasma 25(OH)D level and patient outcomes, which included Overall Survival and Progression Free Survival (PFS). CALGB 80405 is a phase III trial in which patients with newly diagnosed, advanced colorectal cancer were initially randomized to three groups- 1) Chemotherapy (FOLFIRI or mFOLFOX6) with ERBITUX® (Cetuximab) 2) Chemotherapy with AVASTIN® (Bevacizumab) 3) Chemotherapy with ERBITUX® and AVASTIN®. The protocol was later amended to only include patients with KRAS Wild Type tumors and the chemotherapy with ERBITUX® and AVASTIN® group was deleted. This trial was not designed to compare chemotherapy regimens. The Overall Survival (OS) in both the treatment groups were similar at 29+ months.
In the present study, plasma 25(OH)D level were measured at baseline in 1,043 patients at the time of their enrollment in CALGB 80405, and dietary and lifestyle behaviors were collected from self-administered questionnaires. The median plasma 25(OH)D level was 17.2 ng/mL, with the range varying from 2.2 to 72.7 ng/mL (recommended range is 20-30 ng/mL). Factors associated with lower 25(OH)D level included older age, black race, lower dietary and supplemental vitamin D intake, higher Body Mass Index (BMI), ECOG performance status of 1 versus 0 and lower physical activity. Additionally, patients whose blood specimens were drawn in the winter and spring months had significantly lower 25(OH)D level, as did patients who were from the Northern and Northeastern parts of the United States. Vitamin D supplement use was uncommon in this patient population. After adjusting for pathologic and clinical prognostic factors, patients in the group with the highest level of 25(OH)D had significantly improved median OS compared to those in the group with the lowest level (32.6 vs 24.5 months; HR=0.67, P trend 0.002). Higher level of 25(OH)D was also associated with improved PFS (median 12.2 vs 10.1 months; HR 0.80, P trend = 0.02). These results were consistent across all subgroups of patients. The authors concluded that higher plasma level of 25(OH)D was associated with significantly improved survival in metastatic CRC patients treated with a combination of chemotherapy and biologic agents. With 30-35% of the malignancies attributed to dietary habits, the onus is therefore on the treating physicians to provide nutrition counseling during and after cancer treatment. Recommending vitamin D supplements for those patients with colon cancer with low vitamin D levels, may therefore not be unreasonable. Vitamin D status and survival of metastatic colorectal cancer patients: Results from CALGB/SWOG 80405 (Alliance). Ng K, Venook AP, Sato K, et al. J Clin Oncol 33, 2015 (suppl 3; abstr 507)
Pre- and Post-diagnosis Physical Activity, Television Viewing, and Mortality Among Patients With Colorectal Cancer in the National Institutes of Health–AARP Diet and Health Study
SUMMARY: The American Cancer Society estimates that approximately 137,000 new cases of colorectal cancer were diagnosed in the United States in 2014 and over 50,000 died of the disease. Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable. Standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival and Overall Survival. Reducing risk of death and improving survival even further with leisure time physical activity is the topic of this discussion. The most prevalent sedentary behavior, watching TV, has been associated with poorer survival in the general population. Several studies have suggested protective effects of physical activity on cancer recurrence although this has not been conclusive. Pooled data from other studies have shown that lack of physical activity among survivors of ColoRectal Cancer (CRC) has been associated with higher mortality risk. However, the independent effects of physical activity before and after colorectal cancer diagnosis, has remained unclear and the association between watching TV and mortality in survivors of CRC has not been defined.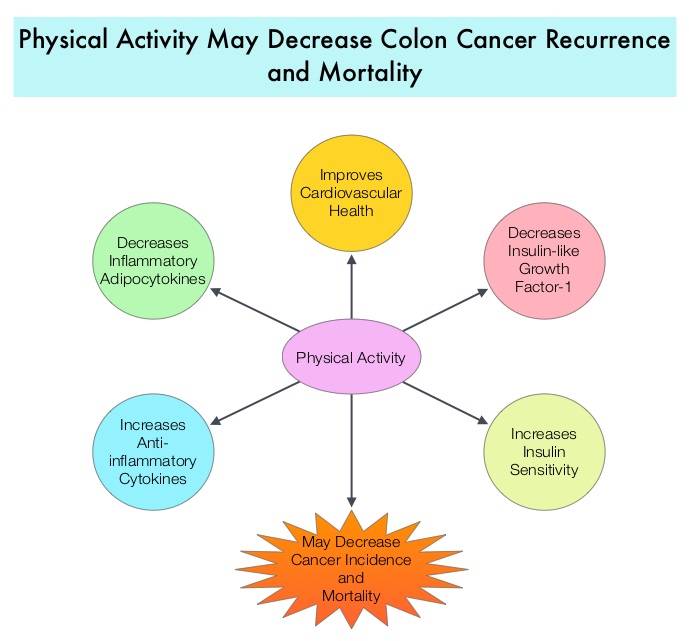 There are several biologic mechanisms that explain the association between sedentary life style, physical activity, and mortality. The adipose tissue in the body in addition to serving as the storage site for energy also releases adipokines, which have pro-inflammatory and anti-inflammatory properties. Physical activity decreases inflammatory adipocytokines and increases anti-inflammatory cytokines and thereby could affect cancer incidence and mortality. Also, physical activity has been shown to increase insulin sensitivity. Several studies have shown increased risk of CRC, increased angiogenesis, tumor growth, and anti-apoptotic activity with higher circulating insulin and insulin-like growth factor-1 and lower insulin-binding protein levels. Physical activity also improves cardiovascular health by lowering blood pressure. The authors in this study explored the impact of lifestyle such as moderate to vigorous intensity physical activity level and TV viewing time (sedentary life style) on ColoRectal Cancer mortality among CRC survivors, with particular attention to pre and post cancer diagnosis contributing factors. Data was collected from a large cohort of patients enrolled in the National Institutes of Health Diet and Health Study and the associations were analyzed between pre CRC diagnosis (N=3797) and post CRC diagnosis (N= 1759) life styles (physical activity and TV watching) and overall and disease-specific mortality. It was noted that patients who had 7 or more hours of weekly leisure physical activity before their diagnosis of CRC had a 20% lower risk of all-cause mortality compared to those who had a sedentary life style and were not engaged in any leisure time activity (HR=0.80; P=0.02). Patients who were engaged in 7 or more hours of weekly leisure physical activity post CRC diagnosis had a 31% lower risk of all-cause mortality compared to those who reported no activity (HR=0.69; P=0.006). This benefit was noted independent of pre-diagnosis activity. Amongst those who reported sedentary lifestyle, patients who spent 5 or more TV hours per day before CRC diagnosis had a 22% increased risk in all-cause mortality compared to those who watched no more than 2 hours of TV per day (HR=1.22; P=0.002). A similar trend of increased risk of all-cause mortality was seen in those who spent more TV hours, post diagnosis although this was not statistically significant. The authors concluded that in patients with CRC, leisure time physical activity was inversely associated with all-cause mortality, whereas more TV hours was associated with increased mortality risk. Health Care providers should therefore proactively promote increasing physical activity and minimizing TV hours, among survivors of ColoRectal Cancer. Arem H, Pfeiffer RM, Engels EA, et al. J Clin Oncol 2015; 33:180-188
There are several biologic mechanisms that explain the association between sedentary life style, physical activity, and mortality. The adipose tissue in the body in addition to serving as the storage site for energy also releases adipokines, which have pro-inflammatory and anti-inflammatory properties. Physical activity decreases inflammatory adipocytokines and increases anti-inflammatory cytokines and thereby could affect cancer incidence and mortality. Also, physical activity has been shown to increase insulin sensitivity. Several studies have shown increased risk of CRC, increased angiogenesis, tumor growth, and anti-apoptotic activity with higher circulating insulin and insulin-like growth factor-1 and lower insulin-binding protein levels. Physical activity also improves cardiovascular health by lowering blood pressure. The authors in this study explored the impact of lifestyle such as moderate to vigorous intensity physical activity level and TV viewing time (sedentary life style) on ColoRectal Cancer mortality among CRC survivors, with particular attention to pre and post cancer diagnosis contributing factors. Data was collected from a large cohort of patients enrolled in the National Institutes of Health Diet and Health Study and the associations were analyzed between pre CRC diagnosis (N=3797) and post CRC diagnosis (N= 1759) life styles (physical activity and TV watching) and overall and disease-specific mortality. It was noted that patients who had 7 or more hours of weekly leisure physical activity before their diagnosis of CRC had a 20% lower risk of all-cause mortality compared to those who had a sedentary life style and were not engaged in any leisure time activity (HR=0.80; P=0.02). Patients who were engaged in 7 or more hours of weekly leisure physical activity post CRC diagnosis had a 31% lower risk of all-cause mortality compared to those who reported no activity (HR=0.69; P=0.006). This benefit was noted independent of pre-diagnosis activity. Amongst those who reported sedentary lifestyle, patients who spent 5 or more TV hours per day before CRC diagnosis had a 22% increased risk in all-cause mortality compared to those who watched no more than 2 hours of TV per day (HR=1.22; P=0.002). A similar trend of increased risk of all-cause mortality was seen in those who spent more TV hours, post diagnosis although this was not statistically significant. The authors concluded that in patients with CRC, leisure time physical activity was inversely associated with all-cause mortality, whereas more TV hours was associated with increased mortality risk. Health Care providers should therefore proactively promote increasing physical activity and minimizing TV hours, among survivors of ColoRectal Cancer. Arem H, Pfeiffer RM, Engels EA, et al. J Clin Oncol 2015; 33:180-188
Statin Use After Colorectal Cancer Diagnosis and Survival: A Population-Based Cohort Study
SUMMARY: Approximately 32 million Americans take a statin in the United States. Statins (3-Hydroxy-3-MethylGlutaryl coenzyme A reductase inhibitors) are usually prescribed to lower LDL cholesterol. Cholesterol is a structural component of cell membranes and a reduction in the availability of cholesterol can result in decreased proliferation and migration of cancer cells. The six statin drugs available in the United States include LIPITOR® (Atorvastatin), ZOCOR® (Simvastatin), CRESTOR® (Rosuvastatin), MEVACOR® (Lovastatin), PRAVACHOL® (Pravastatin) and LESCOL® (Fluvastatin). 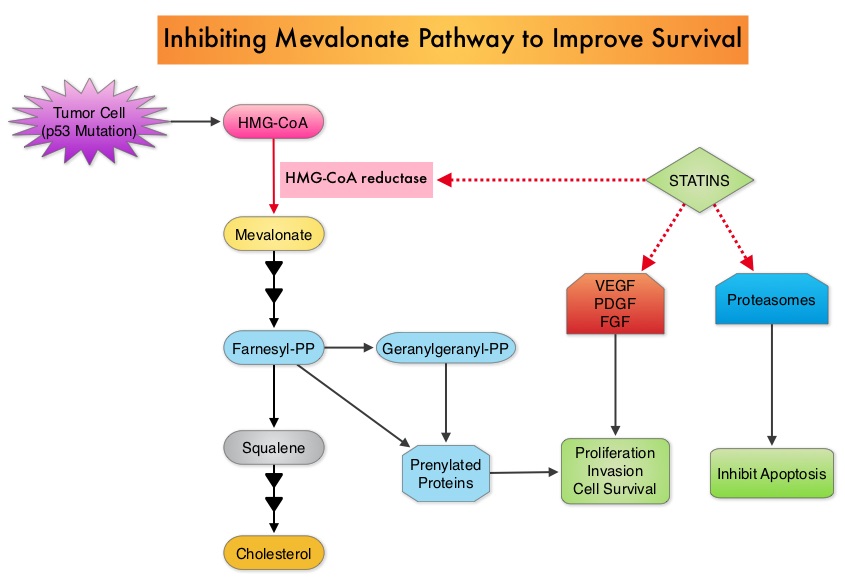 Statin use in cancer patients has been associated with a reduction in cancer related mortality in several clinical studies. This benefit has been attributed to the inhibition of HMG-CoA reductase, which is a rate limiting enzyme in the mevalonate and cholesterol synthesis pathway. The mevalonate pathway is upregulated by mutated p53 (tumor suppressor gene) which is often expressed in cancer cells. By inhibiting the mevalonate pathway, statins can reduce isoprenoid levels such as farnesylpyrophosphate (F-PP) and geranylgeranylpyrophosphate (GG-PP). These isoprenoids are essential for the posttranslational modification of several proteins involved in important intracellular signaling pathways and therefore play a crucial role in cell growth, proliferation, survival and migration. Statins also inhibit angiogenic pathways and proteasomes, thereby negatively impacting cell proliferation and survival. Survival benefit with statin use after colorectal cancer diagnosis has been unclear. To answer this question, the authors identified a cohort of patients (N=7657) diagnosed with stage I to III colorectal cancer from 1998 to 2009, in the National Cancer Data Repository (English Cancer Registry). Information on statin use was obtained from medical records of patients and in this cohort of patients 35% were identified to have used statin drugs following diagnosis of colorectal cancer. Twenty percent of these patients had stage I disease, 43% had stage II disease and 37% had stage III disease. Patients were followed up for 14 years following their diagnosis of colorectal cancer. Statin use after a diagnosis of colorectal cancer was associated with a 29% reduction in colorectal cancer-specific mortality (HR= 0.71). There was a dose-response association with a 36% reduction in colorectal cancer-specific mortality with statin use for more than 1 year (HR=0.64). Statin users after colorectal cancer diagnosis also had a 25% reduction in all-cause mortality (HR=0.75). The authors concluded that based on this large population based colorectal cancer cohort, statin use following diagnosis of colorectal cancer was associated with longer rates of survival. Cardwell CR, Hicks BM, Hughes C, et al. J Clin Oncol 2014;32:3177-3183
Statin use in cancer patients has been associated with a reduction in cancer related mortality in several clinical studies. This benefit has been attributed to the inhibition of HMG-CoA reductase, which is a rate limiting enzyme in the mevalonate and cholesterol synthesis pathway. The mevalonate pathway is upregulated by mutated p53 (tumor suppressor gene) which is often expressed in cancer cells. By inhibiting the mevalonate pathway, statins can reduce isoprenoid levels such as farnesylpyrophosphate (F-PP) and geranylgeranylpyrophosphate (GG-PP). These isoprenoids are essential for the posttranslational modification of several proteins involved in important intracellular signaling pathways and therefore play a crucial role in cell growth, proliferation, survival and migration. Statins also inhibit angiogenic pathways and proteasomes, thereby negatively impacting cell proliferation and survival. Survival benefit with statin use after colorectal cancer diagnosis has been unclear. To answer this question, the authors identified a cohort of patients (N=7657) diagnosed with stage I to III colorectal cancer from 1998 to 2009, in the National Cancer Data Repository (English Cancer Registry). Information on statin use was obtained from medical records of patients and in this cohort of patients 35% were identified to have used statin drugs following diagnosis of colorectal cancer. Twenty percent of these patients had stage I disease, 43% had stage II disease and 37% had stage III disease. Patients were followed up for 14 years following their diagnosis of colorectal cancer. Statin use after a diagnosis of colorectal cancer was associated with a 29% reduction in colorectal cancer-specific mortality (HR= 0.71). There was a dose-response association with a 36% reduction in colorectal cancer-specific mortality with statin use for more than 1 year (HR=0.64). Statin users after colorectal cancer diagnosis also had a 25% reduction in all-cause mortality (HR=0.75). The authors concluded that based on this large population based colorectal cancer cohort, statin use following diagnosis of colorectal cancer was associated with longer rates of survival. Cardwell CR, Hicks BM, Hughes C, et al. J Clin Oncol 2014;32:3177-3183
Calcium, Vitamin D, Dairy Products, and Mortality Among Colorectal Cancer Survivors: The Cancer Prevention Study-II Nutrition Cohort
SUMMARY: The American Cancer Society estimates that approximately 137,000 new cases of colorectal cancer will be diagnosed in the United States in 2014 and over 50,000 are expected to die of the disease. Data from 60 epidemiological studies enrolling more than 26,000 ColoRectal Cancer (CRC) patients have shown that higher consumption of milk and dairy products reduces the risk of colon cancer and high Calcium intake reduces the risk of CRC. In vivo and in vitro studies have confirmed these findings.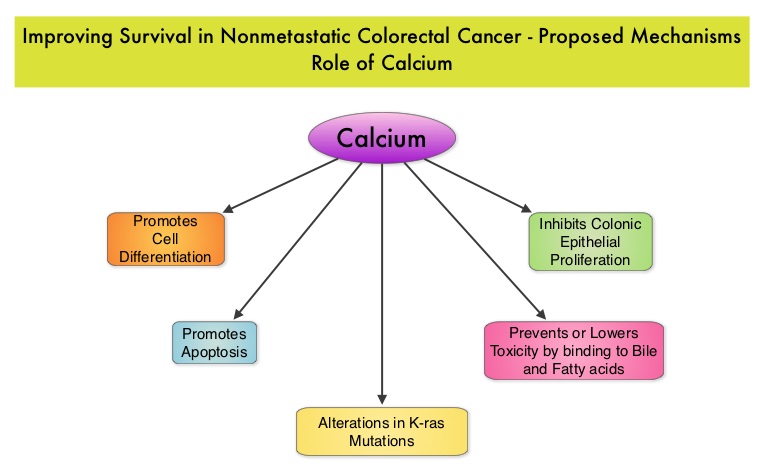 Milk, in addition to being a rich source of dietary Calcium and Vitamin D is a primary dietary source of conjugated linoleic acid which has been shown to inhibit colon cancer cell growth. Dairy products also provide other beneficial components such as butyric acid, lactoferrin and fermentation products. The impact of milk and dairy products on CRC survival however has remained unclear. The Cancer Prevention Study - II Nutrition Cohort is a prospective study of cancer incidence that began in 1992. Participants in this study (N=184,000) were provided a self administered questionnaire and baseline information about their dietary habits (including dietary Calcium and Vitamin D, as well as Calcium, Vitamin D and multivitamin supplements), physical activity, body size, cancer screening and early detection, etc. was collected and follow up questionnaires were sent every other year to update information and learn about new cancer diagnosis. Patients were followed up until June 2009 and by the end of this period, 3,832 individuals who had no history of disease at baseline had been diagnosed with invasive colon or rectal cancer. After excluding patients with distant metastatic disease, 2,284 patients were included in this analysis and among them, 1,111 patients reported post diagnosis diet. The primary outcome of this study was all cause mortality and the secondary outcome was mortality resulting from colorectal cancer. Using standard statistical models, the investigators noted that post CRC diagnosis total Calcium intake and milk intake, was inversely associated with all-cause mortality and significantly reduced CRC specific mortality.
Milk, in addition to being a rich source of dietary Calcium and Vitamin D is a primary dietary source of conjugated linoleic acid which has been shown to inhibit colon cancer cell growth. Dairy products also provide other beneficial components such as butyric acid, lactoferrin and fermentation products. The impact of milk and dairy products on CRC survival however has remained unclear. The Cancer Prevention Study - II Nutrition Cohort is a prospective study of cancer incidence that began in 1992. Participants in this study (N=184,000) were provided a self administered questionnaire and baseline information about their dietary habits (including dietary Calcium and Vitamin D, as well as Calcium, Vitamin D and multivitamin supplements), physical activity, body size, cancer screening and early detection, etc. was collected and follow up questionnaires were sent every other year to update information and learn about new cancer diagnosis. Patients were followed up until June 2009 and by the end of this period, 3,832 individuals who had no history of disease at baseline had been diagnosed with invasive colon or rectal cancer. After excluding patients with distant metastatic disease, 2,284 patients were included in this analysis and among them, 1,111 patients reported post diagnosis diet. The primary outcome of this study was all cause mortality and the secondary outcome was mortality resulting from colorectal cancer. Using standard statistical models, the investigators noted that post CRC diagnosis total Calcium intake and milk intake, was inversely associated with all-cause mortality and significantly reduced CRC specific mortality.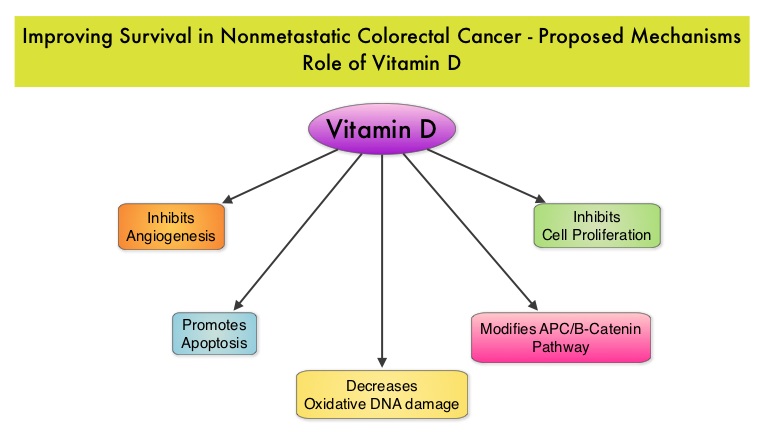 This benefit however, was not seen with Vitamin D intake. Also of interest, pre-diagnosis Calcium, Vitamin D, and dairy product intakes did not influence mortality outcomes. The authors concluded that higher post-diagnosis intakes of total Calcium and milk may be associated with lower risk of death among patients with non-metastatic ColoRectal Cancer. In a more recent publication, it has been reported that there is a strong association between plasma level of 25-hydroxyvitamin D (25-OHD) and CRC specific mortality, with better outcomes in patients with Stage I-III CRC, who had higher plasma levels of 25-OHD (Zgaga L, et al. J Clin Oncol 2014;32:2430-2439). With 30-35% of the malignancies attributed to dietary habits, the onus is therefore on the treating physicians to provide nutrition counseling during and after cancer treatment and is not to be ignored. Yang B, McCullough ML, Gapstur SM, et al. J Clin Oncol 2014;32:2335-2343
This benefit however, was not seen with Vitamin D intake. Also of interest, pre-diagnosis Calcium, Vitamin D, and dairy product intakes did not influence mortality outcomes. The authors concluded that higher post-diagnosis intakes of total Calcium and milk may be associated with lower risk of death among patients with non-metastatic ColoRectal Cancer. In a more recent publication, it has been reported that there is a strong association between plasma level of 25-hydroxyvitamin D (25-OHD) and CRC specific mortality, with better outcomes in patients with Stage I-III CRC, who had higher plasma levels of 25-OHD (Zgaga L, et al. J Clin Oncol 2014;32:2430-2439). With 30-35% of the malignancies attributed to dietary habits, the onus is therefore on the treating physicians to provide nutrition counseling during and after cancer treatment and is not to be ignored. Yang B, McCullough ML, Gapstur SM, et al. J Clin Oncol 2014;32:2335-2343
CALGB/SWOG 80405: Phase III trial of irinotecan/5-FU/leucovorin (FOLFIRI) or oxaliplatin/5-FU/leucovorin (mFOLFOX6) with bevacizumab (BV) or cetuximab (CET) for patients (pts) with KRAS wild-type (wt) untreated metastatic adenocarcinoma of the colon or rectum (MCRC).
SUMMARY: The American Cancer Society estimates that approximately 137,000 new cases of colorectal cancer will be diagnosed in the United States in 2014 and over 50,000 are expected to die of the disease. Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable. Standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival and Overall Survival.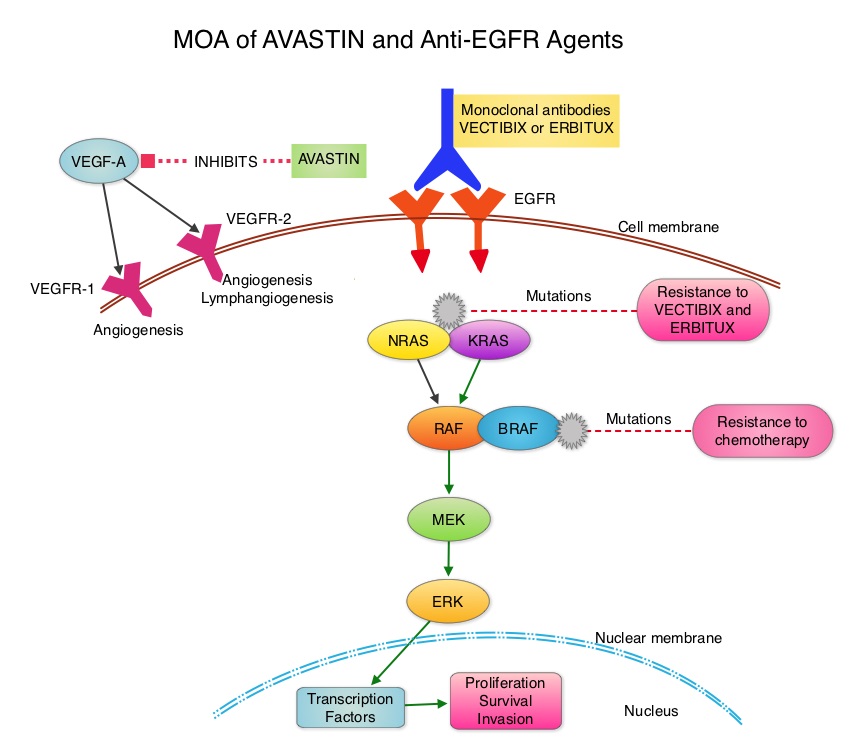 The benefit with anti EGFR agents however is only demonstrable in patients with metastatic colon cancer, whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now becoming clear that even amongst the KRAS Wild Type patient groups, about 15% to 20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Therefore, pan RAS (expanded RAS) testing may become relevant. To determine the optimal combination treatment regimen, this phase III intergroup trial evaluated the addition of ERBITUX® or AVASTIN® to physician’s choice of standard first line chemotherapy such as FOLFIRI or mFOLFOX6. Even though the original study included unselected metastatic colorectal cancer patients and randomization to a third arm (combination of ERBITUX® and AVASTIN®), this study was amended to include only pts with KRAS Wild Type tumors and the combination ERBITUX® and AVASTIN® arm was deleted. Patients were randomized to either ERBITUX® 400 mg/m2 week one and then 250 mg/m2, weekly or AVASTIN® 5 mg/kg every 2 weeks given along with FOLFIRI or mFOLFOX6 chemotherapy (physicians choice at the time of enrollment). The median age was 59 years and treatment groups were Chemo plus AVASTIN® (N=559) and Chemo plus ERBITUX® (N=578). Approximately 27% of the patients received FOLFIRI chemotherapy regimen and 76% received mFOLFOX6 chemotherapy regimen. Treatment was given until disease progression and median follow up was 24 months. The primary endpoint was Overall Survival. The median Overall Survival was similar in the ERBITUX® combination and the AVASTIN® combination groups (about 29 months) and so was the Progression Free Survival in both groups (about 10.5 months). The chemotherapy used with either of the antibodies had no influence on the outcomes. The toxicity profiles were different as expected, with increased incidence of Grade 3-4 rash (7% versus 0%) and diarrhea (11% versus 8%), in the ERBITUX® group and increased incidence of Grade 3-4 hypertension (7% versus 1%) and gastrointestinal events (2% versus 0.5%), in the AVASTIN® group. The authors concluded that either ERBITUX® or AVASTIN® in combination with chemotherapy have equivalent overall survival benefit, when given as first line therapy, for patients with metastatic colorectal cancer, whose tumors are KRAS Wild Type. It remains to be seen however, if pan RAS (expanded RAS) testing and other molecular studies will identify subsets of patients who will benefit from specific antibody chemotherapy combination regimens. Venook AP, Niedzwiecki D, Lenz H, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA3)
The benefit with anti EGFR agents however is only demonstrable in patients with metastatic colon cancer, whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now becoming clear that even amongst the KRAS Wild Type patient groups, about 15% to 20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Therefore, pan RAS (expanded RAS) testing may become relevant. To determine the optimal combination treatment regimen, this phase III intergroup trial evaluated the addition of ERBITUX® or AVASTIN® to physician’s choice of standard first line chemotherapy such as FOLFIRI or mFOLFOX6. Even though the original study included unselected metastatic colorectal cancer patients and randomization to a third arm (combination of ERBITUX® and AVASTIN®), this study was amended to include only pts with KRAS Wild Type tumors and the combination ERBITUX® and AVASTIN® arm was deleted. Patients were randomized to either ERBITUX® 400 mg/m2 week one and then 250 mg/m2, weekly or AVASTIN® 5 mg/kg every 2 weeks given along with FOLFIRI or mFOLFOX6 chemotherapy (physicians choice at the time of enrollment). The median age was 59 years and treatment groups were Chemo plus AVASTIN® (N=559) and Chemo plus ERBITUX® (N=578). Approximately 27% of the patients received FOLFIRI chemotherapy regimen and 76% received mFOLFOX6 chemotherapy regimen. Treatment was given until disease progression and median follow up was 24 months. The primary endpoint was Overall Survival. The median Overall Survival was similar in the ERBITUX® combination and the AVASTIN® combination groups (about 29 months) and so was the Progression Free Survival in both groups (about 10.5 months). The chemotherapy used with either of the antibodies had no influence on the outcomes. The toxicity profiles were different as expected, with increased incidence of Grade 3-4 rash (7% versus 0%) and diarrhea (11% versus 8%), in the ERBITUX® group and increased incidence of Grade 3-4 hypertension (7% versus 1%) and gastrointestinal events (2% versus 0.5%), in the AVASTIN® group. The authors concluded that either ERBITUX® or AVASTIN® in combination with chemotherapy have equivalent overall survival benefit, when given as first line therapy, for patients with metastatic colorectal cancer, whose tumors are KRAS Wild Type. It remains to be seen however, if pan RAS (expanded RAS) testing and other molecular studies will identify subsets of patients who will benefit from specific antibody chemotherapy combination regimens. Venook AP, Niedzwiecki D, Lenz H, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA3)
Multitarget Stool DNA Testing for Colorectal-Cancer Screening
SUMMARY: The American Cancer Society estimates that approximately 137,000 new cases of colorectal cancer will be diagnosed in the United States in 2014 and over 50,000 are expected to die of the disease. It is the third leading cause of cancer death in the U.S. and the lifetime risk of developing colorectal cancer is 1 in 20. Implementation of screening programs in the U.S. has resulted in a 46% decrease in the rate of death from colorectal cancer, from its peak. The U.S. Preventive Services Task Force recommends annual screening with high sensitivity Fecal Occult Blood Testing (FOBT), sigmoidoscopy every 5 years with high-sensitivity FOBT every 3 years and screening colonoscopy every 10 years. Fecal Immunochemical testing (FIT) measures intact human globin protein as opposed to heme. Animal heme from meat will not trigger a false positive test with FIT and as such dietary restrictions are not necessary. Further, FIT is superior to FOBT in detecting advanced adenomas and only requires one stool specimen, as opposed to three specimens for FOBT.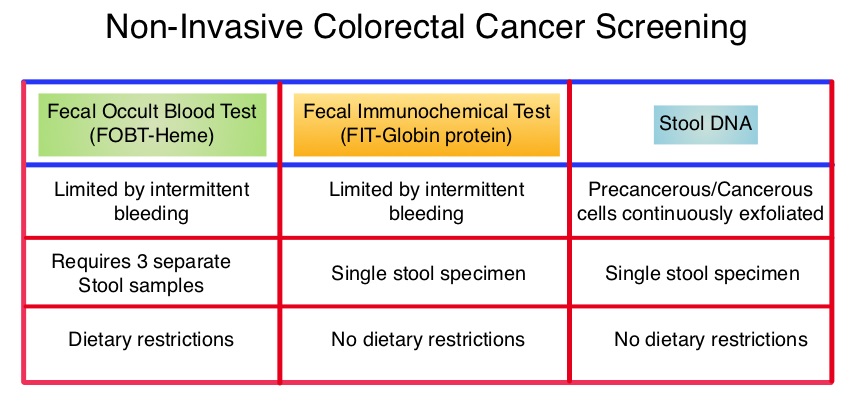 COLOGUARD® is highly sensitive, noninvasive, multitarget, stool based DNA test, for colorectal cancer screening ie.early detection of colorectal cancer and precancerous lesions. This test takes advantage of the genetic and epigenetic alterations that leads to the development of colorectal cancer and analyzes the altered DNA signatures of cancerous and precancerous cells that exfoliate into the colon. In addition, this test includes an immunochemical assay for human hemoglobin. The stool samples can be easily collected, mailed from home, and requires no bowel preparation, medication restrictions or dietary change. The purpose of this study was to determine the sensitivity of COLOGUARD® as compared with FIT, for the detection of screening-relevant colorectal cancer. The study was conducted at 90 medical centers throughout the United States and Canada and evaluable patients (N=9989) were asymptomatic individuals between ages 50 and 84 years who were required to provide a stool sample and undergo screening colonoscopy within 90 days. Enrollment was weighted toward those aged 65 years or older. The primary outcome was the ability of COLOGUARD® to detect colorectal cancer and secondary outcomes were the ability of COLOGUARD® to detect advanced precancerous lesions, polyps with high grade dysplasia and serrated sessile polyps measuring 1 cm or more, when compared to FIT. (Sensitivity is defined as the proportion of persons with disease who have a positive test and Specificity is defined as proportion of persons without disease who have a negative test.) The sensitivity for detecting colorectal cancer was 92% with COLOGUARD® and 74% with FIT (P=0.002). The sensitivity for detecting advanced precancerous lesions was 42.4% vs 23.8% (P<0.001), polyps with high-grade dysplasia was 69.2% vs 46.2% (P=0.004) and serrated sessile polyps measuring 1 cm or more were 42.4% vs 5.1%, (P<0.001) with COLOGUARD® and FIT respectively. Specificities with COLOGUARD® were lower compared to FIT (P<0.001). The authors concluded that COLOGUARD® can detect significantly more colorectal cancers and precancerous lesions than FIT. The high sensitivity of this non-invasive, stool DNA test, to detect curable stage of colorectal cancer, may increase the number of people, who will choose to be screened for colorectal cancer. Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. N Engl J Med 2014; 370:1287-1297
COLOGUARD® is highly sensitive, noninvasive, multitarget, stool based DNA test, for colorectal cancer screening ie.early detection of colorectal cancer and precancerous lesions. This test takes advantage of the genetic and epigenetic alterations that leads to the development of colorectal cancer and analyzes the altered DNA signatures of cancerous and precancerous cells that exfoliate into the colon. In addition, this test includes an immunochemical assay for human hemoglobin. The stool samples can be easily collected, mailed from home, and requires no bowel preparation, medication restrictions or dietary change. The purpose of this study was to determine the sensitivity of COLOGUARD® as compared with FIT, for the detection of screening-relevant colorectal cancer. The study was conducted at 90 medical centers throughout the United States and Canada and evaluable patients (N=9989) were asymptomatic individuals between ages 50 and 84 years who were required to provide a stool sample and undergo screening colonoscopy within 90 days. Enrollment was weighted toward those aged 65 years or older. The primary outcome was the ability of COLOGUARD® to detect colorectal cancer and secondary outcomes were the ability of COLOGUARD® to detect advanced precancerous lesions, polyps with high grade dysplasia and serrated sessile polyps measuring 1 cm or more, when compared to FIT. (Sensitivity is defined as the proportion of persons with disease who have a positive test and Specificity is defined as proportion of persons without disease who have a negative test.) The sensitivity for detecting colorectal cancer was 92% with COLOGUARD® and 74% with FIT (P=0.002). The sensitivity for detecting advanced precancerous lesions was 42.4% vs 23.8% (P<0.001), polyps with high-grade dysplasia was 69.2% vs 46.2% (P=0.004) and serrated sessile polyps measuring 1 cm or more were 42.4% vs 5.1%, (P<0.001) with COLOGUARD® and FIT respectively. Specificities with COLOGUARD® were lower compared to FIT (P<0.001). The authors concluded that COLOGUARD® can detect significantly more colorectal cancers and precancerous lesions than FIT. The high sensitivity of this non-invasive, stool DNA test, to detect curable stage of colorectal cancer, may increase the number of people, who will choose to be screened for colorectal cancer. Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. N Engl J Med 2014; 370:1287-1297
Analysis of KRAS/NRAS mutations in phase 3 study 20050181 of panitumumab (pmab) plus FOLFIRI versus FOLFIRI for second-line treatment (tx) of metastatic colorectal cancer (mCRC).
SUMMARY: It is estimated that approximately 97,000 new cases of colon cancer will be diagnosed in 2014 and over 50,000 will die of the disease. The lifetime risk of developing colorectal cancer is about 1 in 20. Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable. Multi agent chemotherapy in combination with monoclonal antibodies, targeted against Epidermal Growth Factor Receptor (EGFR) such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab), have demonstrated survival benefit, for patients with metastatic colon cancer, whose tumors do not harbor KRAS mutations in exon 2. The authors in this study evaluated the benefit of testing metastatic colorectal cancer tumors for RAS mutations beyond the mutations in the KRAS gene at exon 2.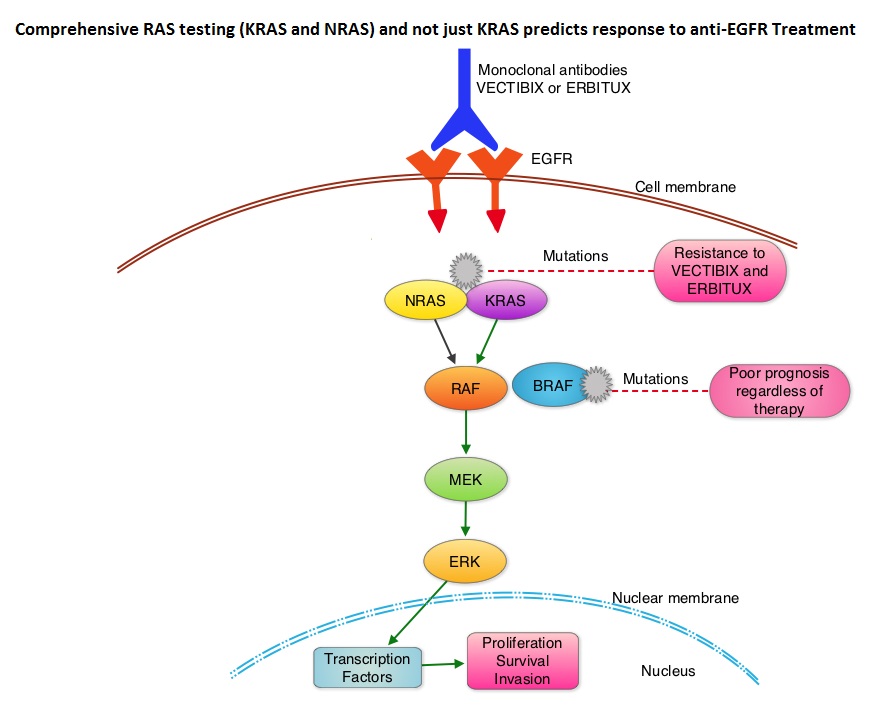 The most common RAS oncogenes in human cancer are HRAS, KRAS, and NRAS. Mutations in HRAS are not common in colon cancer whereas KRAS and NRAS mutations are seen in colon cancer and tend to be mutually exclusive. Activating mutations in exon 2 of the KRAS gene is seen in about 40% of colon cancer patients and predicts resistance to EGFR therapy. Mutational analysis is therefore usually performed to look for mutations in exon 2 of the KRAS gene. It appears however that a broader assessment of the RAS genes may more accurately predict resistance to EGFR therapy. It is also known that mutations in BRAF gene, which is downstream from RAS, may confer poor prognosis in colon cancer, regardless of therapy. The authors in a previous publication showed that in a phase III study involving 1,186 patients, the addition of VECTIBIX®, a fully human, EGFR targeted, monoclonal antibody, when combined with FOLFIRI (Folinic acid, Fluorouracil and Irinotecan), significantly improved Progression Free Survival, when compared to FOLFIRI alone (HR=0.73; P=0.004), with a trend towards improved Overall Survival (HR=0.85; P=0.12). Evolving data has suggested that testing for additional mutations in the RAS genes may help better understand the efficacy of/resistance to VECTIBIX®. In this present analysis, tumor samples of patients from the authors previous study, that were already known to be Wild Type KRAS - unmutated at KRAS exon 2 (N=597), were assessed for additional RAS mutations, specifically in KRAS exons 3 and 4 and NRAS exons 2, 3 and 4. Eighteen percent (18%) of the Wild Type KRAS exon 2 patients harbored additional RAS mutations. It was noted that patients receiving VECTIBIX® along with FOLFIRI had an improvement in both the median OS and PFS when they had wild-type (unmutated) RAS tumors compared to those, whose tumors harbored RAS mutations (median OS: 16.2 vs 11.8 months; median PFS: 6.4 vs 4.8 months). More importantly, amongst patients with mutated RAS tumors, the addition of VECTIBIX® to FOLFIRI resulted in no significant survival benefit compared to FOLFIRI alone (median OS: 11.8 vs 11.1 months; median PFS: 4.8 vs 4.0 months). The authors concluded that comprehensive RAS mutational analysis rather than KRAS testing alone, gives more relevant information for proper selection of patients with metastatic colorectal cancer, who would benefit from EGFR targeted monoclonal antibodies such as VECTIBIX®. In addition patients with RAS mutations could be spared from the associated cost and toxicites of EGFR targeted monoclonal antibodies that will not improve their outcomes. Peeters M, Oliner KS, Price TJ, et al. J Clin Oncol 32, 2014 (suppl 3; abstr LBA387)
The most common RAS oncogenes in human cancer are HRAS, KRAS, and NRAS. Mutations in HRAS are not common in colon cancer whereas KRAS and NRAS mutations are seen in colon cancer and tend to be mutually exclusive. Activating mutations in exon 2 of the KRAS gene is seen in about 40% of colon cancer patients and predicts resistance to EGFR therapy. Mutational analysis is therefore usually performed to look for mutations in exon 2 of the KRAS gene. It appears however that a broader assessment of the RAS genes may more accurately predict resistance to EGFR therapy. It is also known that mutations in BRAF gene, which is downstream from RAS, may confer poor prognosis in colon cancer, regardless of therapy. The authors in a previous publication showed that in a phase III study involving 1,186 patients, the addition of VECTIBIX®, a fully human, EGFR targeted, monoclonal antibody, when combined with FOLFIRI (Folinic acid, Fluorouracil and Irinotecan), significantly improved Progression Free Survival, when compared to FOLFIRI alone (HR=0.73; P=0.004), with a trend towards improved Overall Survival (HR=0.85; P=0.12). Evolving data has suggested that testing for additional mutations in the RAS genes may help better understand the efficacy of/resistance to VECTIBIX®. In this present analysis, tumor samples of patients from the authors previous study, that were already known to be Wild Type KRAS - unmutated at KRAS exon 2 (N=597), were assessed for additional RAS mutations, specifically in KRAS exons 3 and 4 and NRAS exons 2, 3 and 4. Eighteen percent (18%) of the Wild Type KRAS exon 2 patients harbored additional RAS mutations. It was noted that patients receiving VECTIBIX® along with FOLFIRI had an improvement in both the median OS and PFS when they had wild-type (unmutated) RAS tumors compared to those, whose tumors harbored RAS mutations (median OS: 16.2 vs 11.8 months; median PFS: 6.4 vs 4.8 months). More importantly, amongst patients with mutated RAS tumors, the addition of VECTIBIX® to FOLFIRI resulted in no significant survival benefit compared to FOLFIRI alone (median OS: 11.8 vs 11.1 months; median PFS: 4.8 vs 4.0 months). The authors concluded that comprehensive RAS mutational analysis rather than KRAS testing alone, gives more relevant information for proper selection of patients with metastatic colorectal cancer, who would benefit from EGFR targeted monoclonal antibodies such as VECTIBIX®. In addition patients with RAS mutations could be spared from the associated cost and toxicites of EGFR targeted monoclonal antibodies that will not improve their outcomes. Peeters M, Oliner KS, Price TJ, et al. J Clin Oncol 32, 2014 (suppl 3; abstr LBA387)
Newly Diagnosed Colorectal Cancer – NCCN Recommends Universal Screening for Lynch Syndrome
SUMMARY: Lynch Syndrome (Hereditary NonPolyposis Colorectal Cancer - HNPCC), is an autosomal dominant inherited disorder associated with increased risk of colorectal, endometrial, ovary, gastric, small bowel, pancreatic, brain, ureter or renal pelvis cancer. In the United States, approximately 140,000 new cases of colorectal cancer are diagnosed each year of which 3 to 5 percent are caused by Lynch Syndrome (LS). One in 35 patients with newly diagnosed colorectal cancer is related to Lynch Syndrome. Four genes, MLH1, MSH2, MSH6, and PMS2 are involved in the repair of mistakes that occur during DNA replication.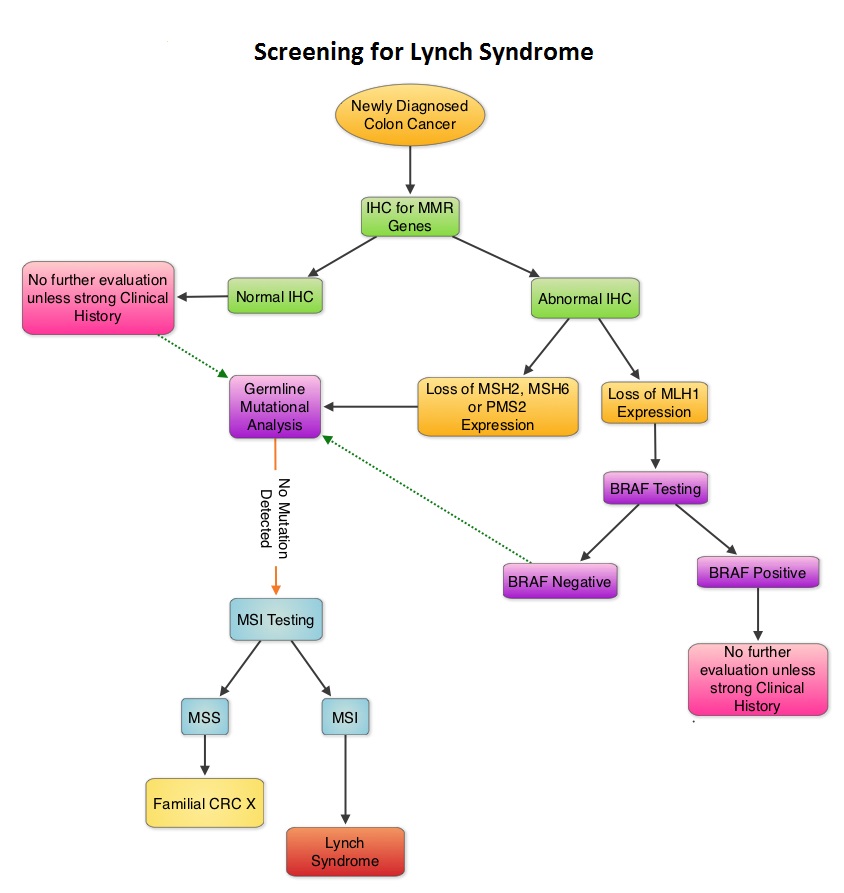 When any of these genes are mutated, repair of DNA replication mistakes is prevented resulting in continuous division of abnormal cells and possibly cancer. The EPCAM gene lies next to the MSH2 gene on chromosome 2 and mutations in the EPCAM gene can cause the MSH2 gene to be inactivated, interrupting DNA repair and leading to accumulation of DNA replication errors and possible malignancy. A Clinical Diagnosis of Lynch Syndrome can be made based on personal and family history if at least three relatives have a malignancy associated with Lynch Syndrome such as colorectal, endometrial, small bowel, ureter or renal pelvis cancer. In addition the following criteria should be met: • One relative must be a first-degree relative of the other two. • At least two successive generations must be affected. • At least one relative with a Lynch syndrome associated cancer should be diagnosed before 50 years of age. • Familial Adenomatous Polyposis should be excluded. • Tumors should be verified whenever possible. Because family history can sometimes be difficult to obtain or confirm NCCN in those circumstances has recommended screening all newly diagnosed colorectal cancer patients for Lynch syndrome. Germline defects/mutations in the mismatch repair genes MLH1, MSH2, MSH6 and PMS2 results in microsatellite instability in tumors. Tumors are described as MSI-High when they have changes in 2 or more, of the 5 microsatellite markers. So, High levels of MSI within a tumor are suggestive of defective DNA mismatch repair. ImmunoHistoChemistry (IHC) staining of tumor tissue is performed for protein expression of the four mismatch repair genes known to be mutated in Lynch Syndrome (MLH1, MSH2, MSH6 and PMS2). IHC test is described as normal when all 4 mismatch repair proteins are normally expressed suggesting that an underlying mismatch repair gene mutation is unlikely. When IHC test is abnormal, it means that that at least one of the 4 mismatch repair proteins is not expressed and an inherited mutation may be present in the gene related to that protein. This can be further confirmed by mutation analysis of the corresponding gene. Screening tests for Lynch syndrome include IHC staining of tumor tissue for protein expression of the four mismatch repair genes and tumor evaluation for MSI. In LS, more than 90% of the tumors are MSI-H (microsatellite instability-high) and/or lack expression of at least one of the mismatch repair proteins by IHC staining and there is a 96% correlation between IHC and MSI when used as a screening test for LS. Approximately 5% of tumors that display MSI may have normal protein expression for the four mismatch repair genes. It should be noted that an abnormal MSI and/or IHC test in colon cancer patients is not diagnostic of Lynch syndrome but can be a useful screening test. This is because even though MSI in the tumor tissue is pathognomonic of Lynch syndrome, approximately 15% of patients with sporadic colorectal cancers exhibit tumors with high MSI as a result of somatic MLH1 promoter hypermethylation. Further, the majority of colon cancer tumors that lack protein expression on IHC staining of MLH1 (often coexisting with loss of PMS2) are often due to an acquired genetic defect. If the IHC indicates absence of MLH1 protein expression, tumor should be tested for BRAF mutation V600E which can be seen in sporadic colorectal cancers but rarely found in patients who have Lynch Syndrome. Once a diagnosis of Lynch Syndrome is made, at risk family members should undergo colonoscopic evaluation at 20-25 years of age or 2-5 years prior to the earliest colon cancer, if it is diagnosed before age 25 and is repeated every 1-2 years. Prophylactic hysterectomy and bilateral salpingo-oophorectomy (BSO) should be considered by women who have completed childbearing. NCCN Guidelines Version 1.2014 Lynch Syndrome
When any of these genes are mutated, repair of DNA replication mistakes is prevented resulting in continuous division of abnormal cells and possibly cancer. The EPCAM gene lies next to the MSH2 gene on chromosome 2 and mutations in the EPCAM gene can cause the MSH2 gene to be inactivated, interrupting DNA repair and leading to accumulation of DNA replication errors and possible malignancy. A Clinical Diagnosis of Lynch Syndrome can be made based on personal and family history if at least three relatives have a malignancy associated with Lynch Syndrome such as colorectal, endometrial, small bowel, ureter or renal pelvis cancer. In addition the following criteria should be met: • One relative must be a first-degree relative of the other two. • At least two successive generations must be affected. • At least one relative with a Lynch syndrome associated cancer should be diagnosed before 50 years of age. • Familial Adenomatous Polyposis should be excluded. • Tumors should be verified whenever possible. Because family history can sometimes be difficult to obtain or confirm NCCN in those circumstances has recommended screening all newly diagnosed colorectal cancer patients for Lynch syndrome. Germline defects/mutations in the mismatch repair genes MLH1, MSH2, MSH6 and PMS2 results in microsatellite instability in tumors. Tumors are described as MSI-High when they have changes in 2 or more, of the 5 microsatellite markers. So, High levels of MSI within a tumor are suggestive of defective DNA mismatch repair. ImmunoHistoChemistry (IHC) staining of tumor tissue is performed for protein expression of the four mismatch repair genes known to be mutated in Lynch Syndrome (MLH1, MSH2, MSH6 and PMS2). IHC test is described as normal when all 4 mismatch repair proteins are normally expressed suggesting that an underlying mismatch repair gene mutation is unlikely. When IHC test is abnormal, it means that that at least one of the 4 mismatch repair proteins is not expressed and an inherited mutation may be present in the gene related to that protein. This can be further confirmed by mutation analysis of the corresponding gene. Screening tests for Lynch syndrome include IHC staining of tumor tissue for protein expression of the four mismatch repair genes and tumor evaluation for MSI. In LS, more than 90% of the tumors are MSI-H (microsatellite instability-high) and/or lack expression of at least one of the mismatch repair proteins by IHC staining and there is a 96% correlation between IHC and MSI when used as a screening test for LS. Approximately 5% of tumors that display MSI may have normal protein expression for the four mismatch repair genes. It should be noted that an abnormal MSI and/or IHC test in colon cancer patients is not diagnostic of Lynch syndrome but can be a useful screening test. This is because even though MSI in the tumor tissue is pathognomonic of Lynch syndrome, approximately 15% of patients with sporadic colorectal cancers exhibit tumors with high MSI as a result of somatic MLH1 promoter hypermethylation. Further, the majority of colon cancer tumors that lack protein expression on IHC staining of MLH1 (often coexisting with loss of PMS2) are often due to an acquired genetic defect. If the IHC indicates absence of MLH1 protein expression, tumor should be tested for BRAF mutation V600E which can be seen in sporadic colorectal cancers but rarely found in patients who have Lynch Syndrome. Once a diagnosis of Lynch Syndrome is made, at risk family members should undergo colonoscopic evaluation at 20-25 years of age or 2-5 years prior to the earliest colon cancer, if it is diagnosed before age 25 and is repeated every 1-2 years. Prophylactic hysterectomy and bilateral salpingo-oophorectomy (BSO) should be considered by women who have completed childbearing. NCCN Guidelines Version 1.2014 Lynch Syndrome
Maintenance treatment with capecitabine and bevacizumab versus observation after induction treatment with chemotherapy and bevacizumab in metastatic colorectal cancer (mCRC): The phase III CAIRO3 study of the Dutch Colorectal Cancer Group (DCCG).
SUMMARY: Treatment of metastatic colorectal cancer with a combination of chemotherapy given along with AVASTIN® is well established. However the duration of therapy remains unclear and it is common to give drug holidays to patients. The outcome in patients who are given these drug holidays remains unclear. The CAIRO3 study is a phase III trial in which patients with previously untreated, unresectable metastatic colorectal cancer received induction treatment with six cycles of Capecitabine (XELODA®)/Oxaliplatin (ELOXATIN®) plus Bevacizumab (AVASTIN®) - CAPOX-B. Patients who had not progressed during induction and had reponses or had stable disease (N=558) were then randomized to receive either XELODA® at 625 mg/m2 twice daily along with AVASTIN® at 7.5 mg/kg every 3 weeks or be observed. Upon first progression, patients in both treatment groups were treated with CAPOX-B until second progression and this was considered the primary endpoint for this study. Secondary endpoints included Overall Survival (OS). Median follow up was 40 months. The median time to second progression from randomization was 19.8 months in the maintenance group and 15 months in the observation group (HR=0.63; P<0.001) The time to first progression in the maintenance treatment group was 8.5 months versus 4.1 months in the observation group (HR 0.41; P<0.001). The time to second progression following treatment with CAPOX-B was 11.8 months in the maintenance group versus 10.5 months for the observation group (HR 0.77; P=0.007), representing a 23% reduction in the risk of progression. The adjusted median OS was 21.7 months with maintenance treatment and 18.2 months in the observation group (HR=0.80; P=0.035). Treatment was well tolerated with slight increase in hand-foot syndrome and neurotoxicity in the maintenance group. Based on this data, the authors recommended maintenance treatment with XELODA® and AVASTIN® until progression or unacceptable toxicity, following 6 cycles of efficacious treatment with CAPOX-B. It is important to note that in the SAKK 41/06 trial conducted by the Swiss Group, observation alone was non-inferior to single agent maintenance AVASTIN® following initial chemotherapy, suggesting that the addition of fluoropyrimidine (XELODA®) chemotherapy to AVASTIN® as maintenance treatment, improves time to progression and median OS in patients with metastatic colorectal cancer. Koopman M, Simkens LH, Ten Tije, AJ et al. J Clin Oncol 31, 2013 (suppl; abstr 3502)
Validation of the 12-Gene Colon Cancer Recurrence Score in NSABP C-07 As a Predictor of Recurrence in Patients With Stage II and III Colon Cancer Treated With Fluorouracil and Leucovorin (FU/LV) and FU/LV Plus Oxaliplatin
SUMMARY: The beneficial role of adjuvant chemotherapy is established in Stage III colon Cancer. This however is less convincing in patients with stage II colon cancer. The conventional clinical and pathological features such as Tumor stage, Grade, Lymphovascular invasion and number of lymph nodes evaluated, may be of some prognostic significance in Stage II colon cancer, but have not been validated. Nonetheless, a majority of these patients receive ELOXATIN® (Oxaliplatin) based adjuvant chemotherapy, with very little benefit and significant toxicity. The 12-gene Colon Cancer Recurrence Score assay was developed after it was validated in multiple studies in over 3000 patients. This assay is not recommended for Stage II MMR (MisMatchRepair) Deficient patients, as these patients have a better survival and their tumors are resistant to 5-Fluorouracil and may actually do worse with adjuvant chemotherapy following surgery. The recurrent score corresponds to the likelihood of colon cancer recurrence 3 years after surgery, with a higher score suggesting a higher risk of recurrence. The authors in this analysis conducted a prospectively designed, clinical validation study of Recurrence Score, in 892 fixed Paraffin embedded tumor specimens from patients with stage II and III colon cancer, randomly assigned to Fluorouracil (FU) or FU plus ELOXATIN® in the National Surgical Adjuvant Breast and Bowel Project C-07. The primary objective of this study was to retrospectively determine the relationship between the recurrent score and the recurrent risk in stage II/III patients treated with 5-FU or 5-FU/ELOXATIN®. Secondary objectives were to determine if recurrence score provided significant information beyond T stage, tumor grade, MMR status and number of lymph nodes examined. From this analysis, the authors reported that recurrent score performs similarly in both Stage II and Stage III colon cancer patients and predicts recurrence risk beyond T and N stage, Grade, MMR status, number of lymph nodes examined and treatment. Amongst Stage II patients, T4 tumors that are MMR proficient fall in the high risk category and chemotherapy should be considered regardless of the recurrent score whereas T3 tumors that are MMR proficient fall in the standard/intermediate risk category and recurrent score assay may assist in the decision making process. In this group, a recurrence score of 41 or more puts these patients at a recurrence risk that is similar to those who have T4 tumors that is MMR proficient and will therefore benefit from adjuvant chemotherapy. In certain stage IIIA/B patients, a low recurrence score of less than 30 is associated with low absolute benefit with ELOXATIN® and therefore is not recommended. The authors concluded that the 12- Gene Colon Cancer Recurrent Score results can help guide adjuvant therapy decisions for patients with Stage II colon cancer and certain patients with Stage III colon cancer. Yothers G, O’Connell MJ, Lee M, et al. J Clin Oncol 2013;31:4512-4519.
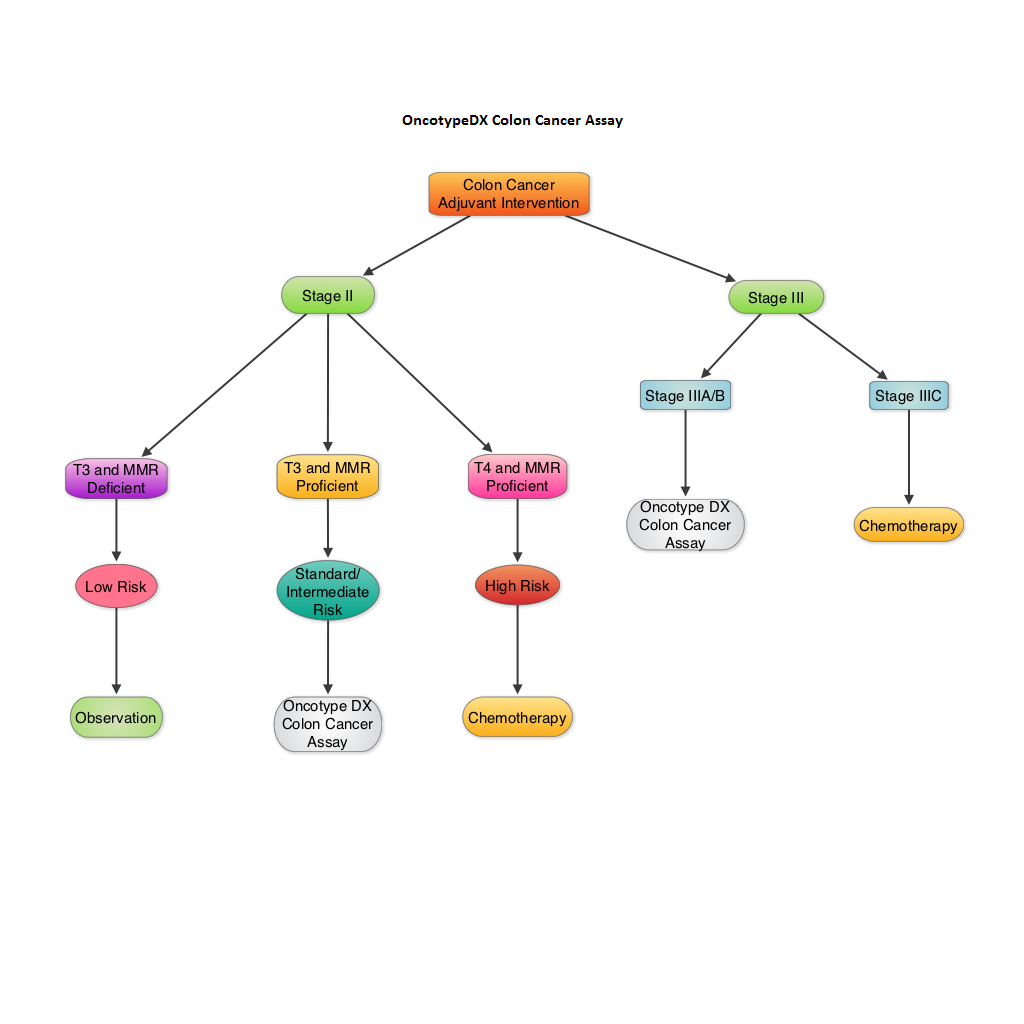
Bevacizumab plus capecitabine versus capecitabine alone in elderly patients with previously untreated metastatic colorectal cancer (AVEX): an open-label, randomised phase 3 trial
SUMMARY: The authors in this randomized phase III trial specifically enrolled chemo naïve patients, 70 years of age or older, with metastatic ColoRectal Cancer (CRC) because, this sub group of patients are often excluded or under- represented in clinical trials. Two hundred and eighty (N=280) chemo naïve patients with metastatic CRC, deemed not to be candidates for more aggressive regimens such as ELOXATIN® (Oxaliplatin) or CAMPTOSAR® (Irinotecan) based chemotherapy regimens, were randomly assigned in a 1:1 ratio to receive either AVASTIN® (Bevacizumab) plus XELODA® (Capecitabine) (n=140) or XELODA® alone (n=140). Treatment consisted of XELODA® 1000 mg/m2 orally twice a day on days 1—14 alone or with AVASTIN® 7•5 mg/kg, given intravenously on day 1. Treatment was given every 3 weeks until disease progression or until unacceptable toxicities were noted. The median age was 76 years and patients were stratified by performance status. The median number of cycles for AVASTIN® plus XELODA® was 9 and for XELODA® alone was 6 cycles. The primary endpoint was Progression Free Survival (PFS). The PFS was significantly longer with the combination of AVASTIN® and XELODA® versus XELODA® alone (9•1 months vs 5•1 months; Hazard Ratio= 0•53; P<0•0001). The combination treatment in general was well tolerated but with a slightly higher incidence of hand-foot syndrome and hemorrhage compared to single agent XELODA®. Overall Survival (OS) was not significantly different between the treatment groups as this study was not powered to detect OS differences. The authors concluded that, in this study, which only enrolled elderly patients with metastatic CRC, unsuitable for aggressive therapy, a combination of AVASTIN® and XELODA® is a reasonable option with proven benefit. Cunningham D, Lang I, Marcuello E, et al. Lancet Oncol 2013;14:1077-1085
Randomized comparison of FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment of KRAS wild-type metastatic colorectal cancer: German AIO study KRK-0306 (FIRE-3).
SUMMARY: It is common practice to combine anti-EGFR agent ERBITUX® (Cetuximab) or anti-VEGF agent AVASTIN® (Bevacizumab) with chemotherapy, in the initial management of patients with metastatic colorectal cancer. There is however a higher likelihood for patients with tumors expressing wild type KRAS (non-mutated KRAS), to respond to ERBITUX®. In this randomized multicenter study, a CAMPTOSAR® (Irinotecan) based backbone, FOLFIRI (folinic acid, fluorouracil and Irinotecan) given along with ERBITUX® (Group A) was compared with FOLFIRI plus AVASTIN® (Group B), in treatment naïve patients with metastatic ColoRectal Cancer (mCRC). Of the 592 patients with wild type KRAS mCRC, 297 patients were randomized to Group A and 295 patients to Group B. The median age was 64 years. The median duration of treatment was 4.7 months and 5.3 months in Group A and Group B respectively. The primary endpoint was Objective Response Rate (ORR). Even though the ORR was comparable in Groups A and B (62% vs 57%), there was a significant improvement in the overall survival (OS) favoring Group A (28.8 vs 25.0 months, HR= 0.77, P=0.0164). The comparable response rates and surprising improvement in OS in the ERBITUX® group suggests that either ERBITUX® or AVASTIN® can be added to FOLFIRI, in the first-line treatment of wild type KRAS mCRC patients. It is however clear that in wild type KRAS mCRC patients, it may be harmful to combine ERBITUX® with FOLFOX chemotherapy regimen, as was seen in the EPOCH trial and based on MRC COIN trial, NORDIC-VII trial and N0147 trial, ERBITUX® should not be combined with FOLFOX chemotherapy regimen as there is no added benefit. It is now well established that mCRC that harbors KRAS mutations in exon 2 (about 40% of the patients) do not benefit from anti-EGFR therapies. The PRIME study has given us aditional insight and it appears that other activating RAS mutations may also predict lack of response to anti-EGFR therapies. With regards to BRAF mutations, they portend a poor prognosis, regardless of treatment. Heinemann V, Weikersthal LF, Decker T, et al. J Clin Oncol 31, 2013 (suppl; abstr LBA3506)
FDA approves STIVARGA® (Regorafenib) for Advanced Colorectal Cancer
SUMMARY: The FDA approved STIVARGA® (Regorafenib), an oral multi-kinase inhibitor for the treatment of patients with metastatic colorectal cancer (CRC) who have progressed on 5FU, ELOXATIN® (Oxaliplatin), CAMPTOSAR® (Irinotecan), anti- VEGF and anti-EGFR therapies. The approval was based on a phase III trial in which 760 patients with metastatic CRC who had progressed after approved standard therapies, were randomly assigned in a 2:1 ratio to receive either STIVARGA® plus best supportive care (BSC) or placebo plus BSC. Patients receiving STIVARGA® had a statistically significant improvement in the overall survival and progression free survival compared to placebo, without any unexpected toxicities. The most common side effects of STIVARGA® were fatigue, loss of appetite, hand-foot syndrome, diarrhea, mucositis, elevated blood pressure, and dysphonia. This important study gives a new option for individuals with advanced colorectal cancer. Grothey A, F. Sobrero AF, Siena S, et al. J Clin Oncol 30, 2012 (suppl 4; abstr LBA385)
Results of a phase III randomized, double-blind, placebo-controlled, multicenter trial (CORRECT) of regorafenib plus best supportive care (BSC) versus placebo plus BSC in patients (pts) with metastatic colorectal cancer (mCRC) who have progressed after standard therapies.
SUMMARY: In this phase III trial, patients with metastatic colorectal carcinoma who had progressed after approved standard therapies were randomly assigned in a 2:1 ratio to receive either Regorafenib, an oral multikinase inhibitor plus best supportive care or placebo plus best supportive care. Seven hundred and sixty patients were randomized. Patients receiving Regorafenib had a statistically significant improvement in the overall survival and progression free survival compared to placebo, without any unexpected toxicities. This important study gives a new option for individuals with advanced colorectal cancer who have progressed on all available standard therapies. Grothey A, F. Sobrero AF, Siena S, et al. J Clin Oncol 30, 2012 (suppl 4; abstr LBA385)
Bevacizumab (BEV) plus chemotherapy (CT) continued beyond first progression in patients with metastatic colorectal cancer (mCRC) previously treated with BEV plus CT: Results of a randomized phase III intergroup study (TML study).
SUMMARY: The ML18147 (TML) is a randomized phase III trial in which patients who received AVASTIN® (Bevacizumab) plus standard chemotherapy as initial treatment (first-line treatment) for their metastatic colorectal cancer were then randomized to either continue AVASTIN® with a different chemotherapy after their cancer progressed (second-line treatment) or receive the different chemotherapy regimen without AVASTIN®. Patient group continuing AVASTIN® as a part of second line treatment demonstrated an improved survival compared to those who received chemotherapy alone, as second line treatment. This study has demonstrated that continuing AVASTIN® with second line chemotherapy post progression, extends survival in patients with metastatic colorectal cancer. Arnold D, Andre T, Bennouna J, et al. J Clin Oncol 30, 2012 (suppl; abstr CRA3503)
Intravenous (IV) aflibercept versus placebo in combination with irinotecan/5-FU (FOLFIRI) for second-line treatment of metastatic colorectal cancer (MCRC): Results of a multinational phase 3 trial (EFC10262-VELOUR).
SUMMARY: ZALTRAP® (Aflibercept) is a soluble fusion protein that is capable of binding with high affinity to pro-angiogenic factors such as all VEGF-A isoforms, VEGF-B, and PlGF. This is unlike bevacizumab, which is a monoclonal antibody that only targets all isoforms of VEGF-A. VELOUR is a phase III trial in which 1,226 patients who had failed oxaliplatin-based therapy received second-line therapy and the comparison was FOLFIRI (leucovorin, fluorouracil, irinotecan) with or without ZALTRAP® (Aflibercept). With a median follow-up of 22.3 months, there was significant improvement in the progression-free survival noted in the ZALTRAP® (Aflibercept) group (6.9 vs 4.67 months; HR = 0.758;P = .00007) as well as overall survival (13.5 vs 12.06 months; HR = 0.817;P = .0032). This benefit was seen irrespective of prior bevacizumab therapy. The authors did point out that in the E3200 Intergroup trial, which tested second-line FOLFOX4 chemotherapy with or without bevacizumab, all of the patients were bevacizumab-naive, whereas 70% in the VELOUR trial were bevacizumab-naive.Van Cutsem E, Tabernero J, Lakomy R, et al. Results of a multinational phase 3 trial (EFC10262-VELOUR). 13th ESMO World Congress on Gastrointestinal Cancer. Abstract 0-0024.