⇚
Acute Lymphocytic Leukemia
Chemotherapy-Free First Line Induction and Consolidation Treatment for Acute Lymphocytic Leukemia
SUMMARY: It is estimated that 6150 individuals will be diagnosed with Acute Lymphocytic Leukemia (ALL) in the US and 1520 patients will die of the disease. ALL is more common in children, but can occur at any age and arises from malignant transformation of B- or T-cell progenitor cells. These cells express surface antigens that define their respective lineages. Precursor B-cell ALL cells typically express CD10, CD19, and CD34 on their surface, along with nuclear Terminal deoxynucleotide Transferase (TdT), whereas precursor T-cell ALL cells commonly express CD2, CD3, CD7, CD34, and TdT.
Philadelphia Chromosome (Chromosome 22) is a result of a reciprocal translocation between chromosomes 9 and 22, wherein the ABL gene from chromosome 9 fuses with the BCR gene on chromosome 22. As a result, the auto inhibitory function of the ABL gene is lost and the BCR-ABL fusion gene is activated resulting in cell proliferation and leukemic transformation of hematopoietic stem cells. Approximately 20% of adults and a small percentage of children with ALL are Philadelphia Chromosome (Ph) positive, and in the majority of children and in more than 50% of adults with Ph-positive ALL, the molecular abnormality (fusion protein) is different from that in Ph-positive Chronic Myelogenous Leukemia (p190 versus p210).
Adult patients with Ph-positive ALL are rarely cured with chemotherapy and the prognosis in these patients has markedly improved with the availability of BCR/ABL targeted Tyrosine Kinase Inhibitors (TKIs). Use of these TKIs with or without chemotherapy can result in a Complete Hematologic Remission in 94-100% of patients, irrespective of age. Eligible patients are then usually referred for allogeneic Hematopoietic Stem Cell Transplant (allo HSCT). To increase the chance of cure and decrease the likelihood of relapse, sustained decrease in Minimal Residual Disease is required, with a reduction in the tumor burden to less than 1 tumor cell in 10,000 bone marrow mononuclear cells.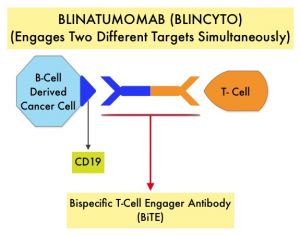
BiTE® technology (Bispecific T cell Engager antibody) engages the body's immune system to detect and target malignant cells. These modified antibodies are designed to engage two different targets simultaneously, thereby placing the patient’s T cells within reach of the targeted cancer cell and facilitating apoptosis of the cancer cell. BiTE® antibodies are currently being investigated to treat a wide variety of malignancies. BLINCYTO® (Blinatumomab) is a BiTE® antibody designed to activate the patients T cells with its anti-CD3 group and then bind them to tumor cells with its anti-CD19 group, thus promoting cellular cytotoxicity. CD19 is a protein expressed on the surface of B-cell derived leukemias and lymphomas
The Italian GIMEMA investigators adopted a chemotherapy-free induction strategy and conducted a Phase II single-group trial, in which adults (no upper age limit) with newly diagnosed Ph-positive ALL, received first line therapy with SPRYCEL® (Dasatinib) plus glucocorticoids, followed by two cycles of BLINCYTO® (Blinatumomab). This study enrolled 63 patients with newly diagnosed Ph-positive ALL, and patients received prephase treatment with a glucocorticoid for 7 days before they received SPRYCEL®, and glucocorticoids were continued for an additional 24 days and discontinued on day 31. SPRYCEL® 140 mg orally once daily was administered as induction therapy for 85 days.
Patients who completed the induction phase received consolidation treatment with BLINCYTO® 28 mcg per day, and before each BLINCYTO® cycle, Dexamethasone 20 mg was administered. A minimum of two cycles of BLINCYTO® was mandatory and up to three additional cycles were allowed. Levetiracetam 500 mg twice daily was administered during treatment with BLINCYTO®, to prevent CNS adverse events. SPRYCEL® was continued during treatment with BLINCYTO®, and after BLINCYTO® administration, except in those patients in whom a T315I mutation was detected during the induction phase. Lumbar punctures were performed at diagnosis, at days 14, 22, 43, 57, and 85, and at the end of each BLINCYTO® cycle, for a total of 12 procedures. The choice of postconsolidation treatment, including allogeneic HSCT and subsequent administration of a Tyrosine Kinase Inhibitor, was at the discretion of the investigators. The median patient age was 54 years, 54% of the patients were women, and the median WBC was 13,000 per cubic millimeter. Of the 63 enrolled patients, 65% had the p190 fusion protein, 27% had the p210 fusion protein, and 8% had both. The most frequent molecular aberration was IKZF1 deletion (54%). The Primary endpoint was sustained molecular response in the bone marrow after this treatment.
Complete Hematologic Response was observed in 98% of the patients at the end of SPRYCEL® induction therapy (day 85), and the molecular response rate was 29%, and this percentage increased to 60% after two cycles of BLINCYTO®, with further increase in molecular responses after additional cycles of treatment with BLINCYTO®. At a median follow up of 18 months, Overall Survival was 95% and Disease Free Survival (DFS) was 88%. The probability of DFS among patients who had a molecular response at the end of induction therapy (day 85) was 100%, as compared with 85% among patients with a non-molecular response. There was no significant difference noted in the DFS between patients with p190 and those with p210. Patients who had an IKZF1 deletion along with additional genetic aberrations had lower Disease Free Survivals. Mutations in the ABL1 gene were detected in 6 patients who had increased Minimal Residual Disease during induction therapy, and all these mutations were cleared by BLINCYTO®. A total of 24 patients received an allogeneic HSCT, and the transplantation-related mortality was 4%. The most common adverse events of any grade were pyrexia, cytomegalovirus infection/reactivation and neutropenia.
The authors concluded that a chemotherapy-free induction and consolidation first-line treatment with SPRYCEL® and BLINCYTO®, that was based on a targeted and immunotherapeutic strategy respectively, was associated with high incidences of molecular response and survival, with fewer Grade 3 or higher adverse events, in adults with Philadelphia chromosome-positive ALL.
Dasatinib-Blinatumomab for Ph-Positive Acute Lymphoblastic Leukemia in Adults. Foà R, Bassan R, Vitale A, et al. for the GIMEMA Investigators. N Engl J Med 2020; 383:1613-1623
First CAR T-Cell Immunotherapy Approved by the FDA for Acute Lymphoblastic Leukemia
SUMMARY: The FDA on August 30, 2017, granted regular approval to KYMRIAH® (Tisagenlecleucel) for the treatment of patients up to age 25 years with B-cell precursor Acute Lymphoblastic Leukemia (ALL), that is refractory or in second or later relapse. KYMRIAH® is the first Chimeric Antigen Receptor (CAR) T-cell immunotherapy approved by the FDA.
What is (CAR) T-cell immunotherapy? Chimeric Antigen Receptor (CAR) T-cell therapy is a type of immunotherapy and consists of T cells collected from the patient’s blood in a leukapheresis procedure, and genetically engineered to produce special receptors on their surface called Chimeric Antigen Receptors (CAR). These reprogrammed cytotoxic T cells with the Chimeric Antigen Receptors on their surface are now able to recognize a specific antigen on tumor cells. These genetically engineered and reprogrammed CAR T-cells are grown in the lab and are then infused into the patient. These cells in turn proliferate in the patient’s body and the engineered receptor on the cell surface help recognize and kill cancer cells that expresses that specific antigen. KYMRIAH® (genetically engineered T-cells) seeks out cancer cells expressing the antigen CD19, which is found uniquely on B cells and destroy them. Patients, following treatment with CAR T-cells, develop B-cell aplasia (absence of CD19 positive cells) due to B-cell destruction and may need immunoglobin replacement. Hence, B-cell aplasia can be a useful therapeutic marker, as continued B-cell aplasia has been seen in all patients who had sustained remission, following CAR T-cell therapy.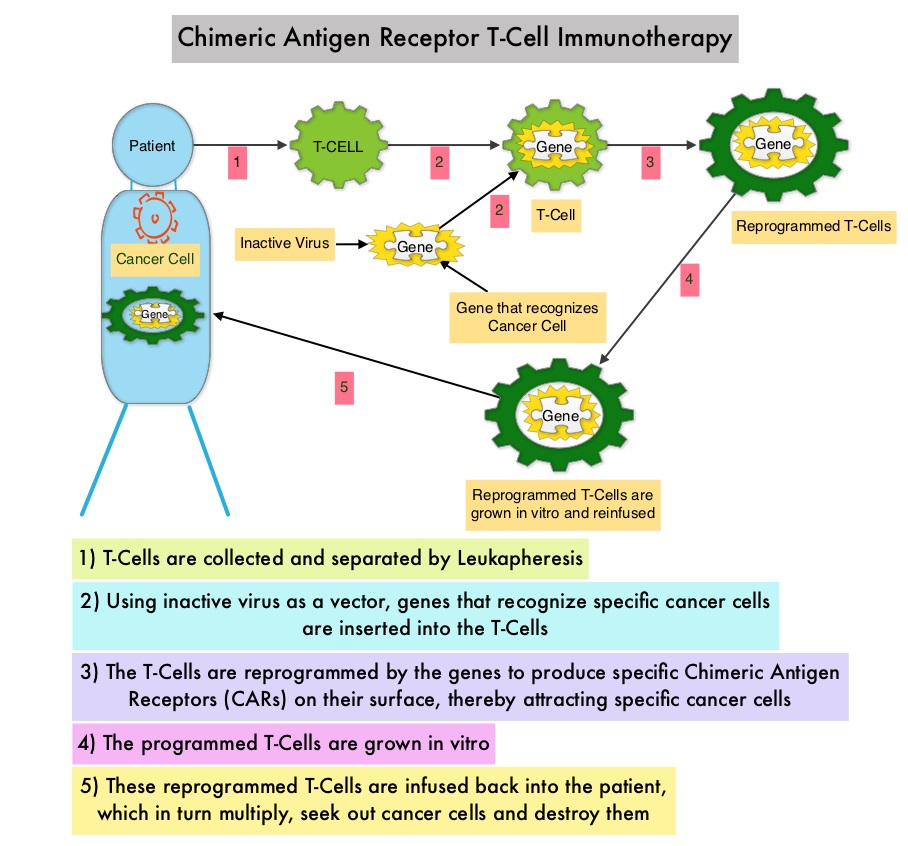 Cytokine Release Syndrome, an inflammatory process is the most common and serious side effect of CAR T-cell therapy and is associated with marked elevation of Interleukin-6. Cytokine release is important for T-cell activation and can result in high fevers and myalgias. This is usually self limiting although if severe can be associated with hypotension and respiratory insufficiency. Tocilizumab (ACTEMRA®), an Interleukin-6 receptor blocking antibody produces a rapid improvement in symptoms. This is however not recommended unless the symptoms are severe and life threatening, as blunting the cytokine response can in turn negate T-cell proliferation. Elevated serum Ferritin and C-reactive protein levels are surrogate markers for severe Cytokine Release Syndrome.
Cytokine Release Syndrome, an inflammatory process is the most common and serious side effect of CAR T-cell therapy and is associated with marked elevation of Interleukin-6. Cytokine release is important for T-cell activation and can result in high fevers and myalgias. This is usually self limiting although if severe can be associated with hypotension and respiratory insufficiency. Tocilizumab (ACTEMRA®), an Interleukin-6 receptor blocking antibody produces a rapid improvement in symptoms. This is however not recommended unless the symptoms are severe and life threatening, as blunting the cytokine response can in turn negate T-cell proliferation. Elevated serum Ferritin and C-reactive protein levels are surrogate markers for severe Cytokine Release Syndrome.
The CAR T-cells have been shown to also access sanctuary sites such as the central nervous system and eradicate cancer cells. CD19 antigen is expressed by majority of the B cell malignancies and therefore most studies using CAR T-cell therapy have focused on the treatment of advanced B-cell malignancies such as Chronic Lymphocytic Leukemia (CLL), Acute Lymphoblastic Leukemia (ALL) and Non Hodgkin lymphoma (NHL), such as Diffuse Large B-Cell Lymphoma (DLBCL). Previously published studies have shown significant responses with CAR T-cell therapy in patients with relapsed and refractory B-cell ALL. But the durability of remission has remained unclear.
This FDA approval was based on ELIANA, an ongoing single-arm, open-label, multicenter, global, phase II study, that has enrolled 88 pediatric/young adult patients with CD19-positive Relapsed/Refractory B-cell ALL and with 5% or more bone marrow lymphoblasts by morphology. The median age was 12 years, 59% of patients had prior allogeneic Stem Cell Transplant and patients had received a median of 3 lines of therapy previously. Following completion of lymphodepleting chemotherapy which in most patients consisted of Fludarabine/Cyclophosphamide, patients were infused with a single dose of KYMRIAH® within 2 to 14 days following the completion of lymphodepleting chemotherapy. The primary endpoint was Overall Remission Rate - Complete Remission [CR] + CR with incomplete blood count recovery [CRi], within 3 months. Secondary endpoints included Duration of Remission (DOR), Overall Survival, Safety, and cellular kinetics.
The authors reported an updated interim analysis with a median study follow up of 6.4 months. Of the 63 patients who were evaluable for efficacy, the Overall Remission Rate was 83%, with 63% of patients achieving a Complete Remission (CR) and 19% achieving a Complete Remission with incomplete hematological recovery (CRi) within 3 months of KYMRIAH® infusion. All patients with a confirmed CR or CRi were Minimal Residual Disease (MRD) negative by flow cytometry. The relapse-free probability at 6 months after remission onset was 75% and the median Duration of Remission has not been reached. The probability of survival at 6 months was 89% and at 12 months was 79%. Thirteen percent (13%) of responders went on to have allogeneic Stem Cell Transplant within 6 months, while in remission.
The most common adverse reactions were Cytokine Release Syndrome (CRS), hypogammaglobulinemia, nausea, diarrhea, vomiting, fever, infections, headache, encephalopathy, hypotension, bleeding episodes, tachycardia, hypoxia and fatigue. Grade 3 or 4 adverse events were noted in 84% of patients. Patients with Severe Cytokine Release Syndrome were effectively treated with the Interleukin-6 receptor blocking antibody Tocilizumab (ACTEMRA®). The expansion of the genetically engineered T-cells in vivo correlated with CRS severity, and persistence of these reprogrammed T cells along with B-cell aplasia in peripheral blood was observed for 1 year or more in some responders.
The authors concluded that the ELIANA trial is the first multicenter trial of a CAR T-cell therapy and a single infusion of KYMRIAH® was highly efficacious, in patients with relapsed and refractory ALL, and was associated with a high and durable remission rate. This technology may be applied to other malignancies, as new antigen targets are identified. Buechner J, Grupp SA, Maude SL, et al. Global registration trial of efficacy and safety of CTL019 in pediatric and young adult patients with relapsed/refractory (r/r) acute lymphoblastic leukemia (ALL): update to the interim analysis. Presented at: 2017 EHA Congress; June 22-25, 2017; Madrid, Spain. Abstract S476.
Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody, Blinatumomab in patients (pts) with relapsed/refractory B-precursor acute lymphoblastic leukemia (r/r ALL).
SUMMARY: The FDA on December 3, 2014, granted accelerated approval to BLINCYTO® (Blinatumomab), a bispecific T cell engager (BiTE) antibody, for treatment of Philadelphia chromosome-negative (Ph-) Relapsed or Refractory B- cell precursor Acute Lymphoblastic Leukemia (ALL). BiTE® technology engages the body's immune system to detect and target malignant cells. These modified antibodies are designed to engage two different targets simultaneously, thereby placing the T cells within reach of the targeted cancer cell and facilitating apoptosis of the cancer cell. BiTE® antibodies are currently being investigated to treat a wide variety of malignancies.  BLINCYTO® (Blinatumomab) is an investigational BiTE® antibody designed to direct the patients T cells against CD19, a protein found on the surface of B-cell derived leukemias and lymphomas. The approval was based on a multicenter single-arm phase II trial in which 185 patients with Relapsed or Refractory Philadelphia chromosome negative ALL patients were enrolled. The median age was 39 years, and patients had their 1st relapse and were refractory to post hematopoietic stem cell transplantation less than 12 months before. About a third of the patients had at least 2 salvage therapies. BLINCYTO® was given by continuous IV infusion, 4 weeks on and 2 weeks off for up to 5 cycles and the median number of cycles given were 2. The primary endpoint was complete remission (CR) and response with a reduction in Minimal Residual Disease (MRD) to less than 10-4 or CR with partial hematological recovery (CRh), within the first 2 cycles of treatment. It was noted that 32% of patients attained CR with 2 cycles of treatment with BLINCYTO® and these responses were durable (median 6.7 months). Further, 31% of the patients in this study had a CR with or without complete hematological recovery but with reduction in MRD to less than 10-4. At the time of primary analysis, 80% of responses occurred within cycle 1. Further, the Complete Remissions (CR) and CR with partial hematological recovery (CRh) were seen in all subgroups of patients, although this was more pronounced in those with less than 50% bone marrow blasts. The median Relapse Free Survival and Overall survival were 5.9 months and 6.1 months respectively. The most frequent grade 3 adverse events were febrile neutropenia, neutropenia and anemia, occurring in 26%, 15% and 15% of patients, respectively. The authors concluded that BLINCYTO® has significant single agent antileukemia activity in a difficult-to-treat population with Relapsed and Refractory Acute Lymphoblastic Leukemia. Future studies will hopefully address whether BLINCYTO® can serve as a bridge to transplantation, in patients with Relapsed and Refractory B-cell ALL. Cytokine Release Syndrome can result from the activation of the immune system. The FDA approved BLINCYTO® with a Risk Evaluation and Mitigation Strategy (REMS). Topp MS, Goekbuget N, Stein AS, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7005)
BLINCYTO® (Blinatumomab) is an investigational BiTE® antibody designed to direct the patients T cells against CD19, a protein found on the surface of B-cell derived leukemias and lymphomas. The approval was based on a multicenter single-arm phase II trial in which 185 patients with Relapsed or Refractory Philadelphia chromosome negative ALL patients were enrolled. The median age was 39 years, and patients had their 1st relapse and were refractory to post hematopoietic stem cell transplantation less than 12 months before. About a third of the patients had at least 2 salvage therapies. BLINCYTO® was given by continuous IV infusion, 4 weeks on and 2 weeks off for up to 5 cycles and the median number of cycles given were 2. The primary endpoint was complete remission (CR) and response with a reduction in Minimal Residual Disease (MRD) to less than 10-4 or CR with partial hematological recovery (CRh), within the first 2 cycles of treatment. It was noted that 32% of patients attained CR with 2 cycles of treatment with BLINCYTO® and these responses were durable (median 6.7 months). Further, 31% of the patients in this study had a CR with or without complete hematological recovery but with reduction in MRD to less than 10-4. At the time of primary analysis, 80% of responses occurred within cycle 1. Further, the Complete Remissions (CR) and CR with partial hematological recovery (CRh) were seen in all subgroups of patients, although this was more pronounced in those with less than 50% bone marrow blasts. The median Relapse Free Survival and Overall survival were 5.9 months and 6.1 months respectively. The most frequent grade 3 adverse events were febrile neutropenia, neutropenia and anemia, occurring in 26%, 15% and 15% of patients, respectively. The authors concluded that BLINCYTO® has significant single agent antileukemia activity in a difficult-to-treat population with Relapsed and Refractory Acute Lymphoblastic Leukemia. Future studies will hopefully address whether BLINCYTO® can serve as a bridge to transplantation, in patients with Relapsed and Refractory B-cell ALL. Cytokine Release Syndrome can result from the activation of the immune system. The FDA approved BLINCYTO® with a Risk Evaluation and Mitigation Strategy (REMS). Topp MS, Goekbuget N, Stein AS, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7005)
Chimeric Antigen Receptor T Cells for Sustained Remissions in Leukemia
SUMMARY: The FDA has granted Breakthrough Therapy Designation to immunotherapy with CTL019, which are genetically engineered T-cells. Chimeric Antigen Receptor (CAR) T-cell therapy is a type of immunotherapy in which T cells collected from the patient’s own blood and are genetically engineered to produce special receptors on their surface called chimeric antigen receptors (CAR’s). The cytotoxic T cells with these chimeric antigen receptors on their surface are now able to recognize a specific antigen on tumor cells. These engineered CAR T-cells which are grown in the lab are then infused into the patient and they in turn proliferate in the patient’s body and the engineered receptor on their surface help recognize and kill cancer cells that expresses that specific antigen. CTL019 are genetically engineered T-cells using CAR technology that seeks out cancer cells expressing the antigen CD19, which is found uniquely on B cells and destroy them.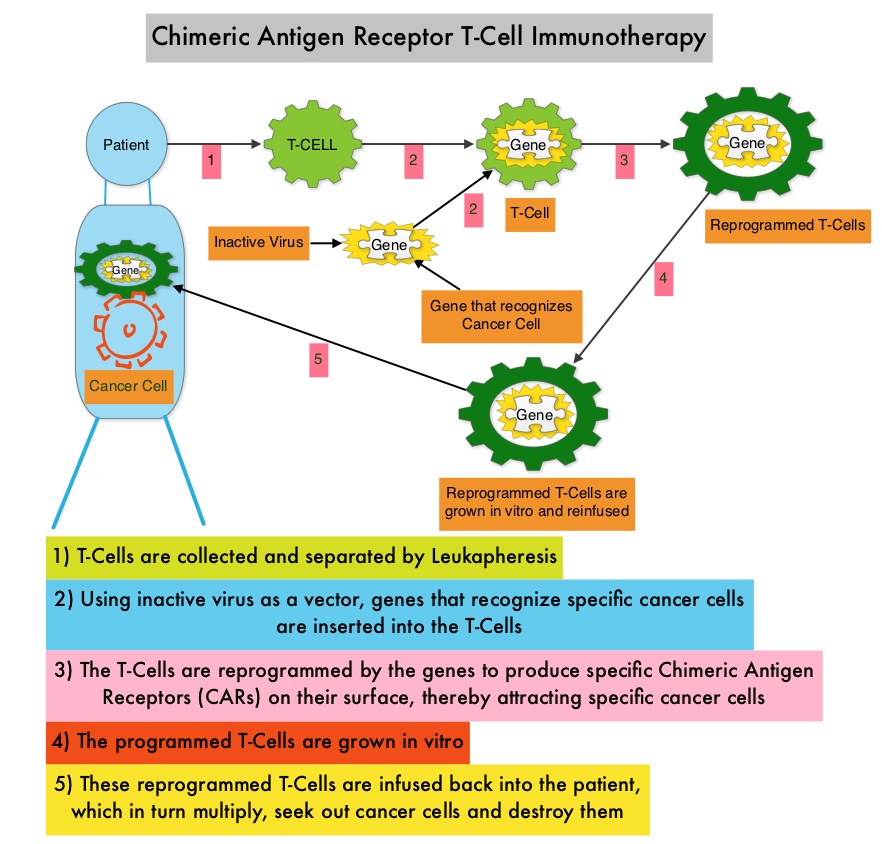 Patients, following treatment with CAR T-cells, develop B-cell aplasia (absence of CD19 positive cells) due to B-cell destruction and may need immunoglobin replacement. Hence, B-cell aplasia can be a useful therapeutic marker, as continued B-cell aplasia has been seen in all patients who had sustained remission, following CAR T-cell therapy. Cytokine Release Syndrome, an inflammatory process is the most common and serious side effect of CAR T-cell therapy and is associated with marked elevation of Interleukin-6. Cytokine release is important for T-cell activation and can result in high fevers and myalgias. This is usually self limiting although if severe can be associated with hypotension and respiratory insufficiency. Tocilizumab, an Interleukin-6 receptor blocking antibody produces a rapid improvement in symptoms. This is however not recommended unless the symptoms are severe and life threatening, as blunting the cytokine response can in turn negate T-cell proliferation. Elevated serum Ferritin and C-reactive protein levels are surrogate markers for severe Cytokine Release Syndrome. The CAR T-cells have been shown to also access sanctuary sites such as the central nervous system and eradicate cancer cells. CD19 antigen is expressed by majority of the B cell malignancies and therefore most studies using CAR T-cell therapy have focused on the treatment of advanced B-cell malignancies such as Chronic Lymphocytic Leukemia (CLL), Acute Lymphoblastic Leukemia (ALL) and Non Hodgkin lymphoma (NHL), such as Diffuse Large B-Cell Lymphoma (DLBCL). Previously published studies have shown significant responses with CAR T-cell therapy in patients with relapsed and refractory B-cell ALL. But the durability of remission has remained unclear.
Patients, following treatment with CAR T-cells, develop B-cell aplasia (absence of CD19 positive cells) due to B-cell destruction and may need immunoglobin replacement. Hence, B-cell aplasia can be a useful therapeutic marker, as continued B-cell aplasia has been seen in all patients who had sustained remission, following CAR T-cell therapy. Cytokine Release Syndrome, an inflammatory process is the most common and serious side effect of CAR T-cell therapy and is associated with marked elevation of Interleukin-6. Cytokine release is important for T-cell activation and can result in high fevers and myalgias. This is usually self limiting although if severe can be associated with hypotension and respiratory insufficiency. Tocilizumab, an Interleukin-6 receptor blocking antibody produces a rapid improvement in symptoms. This is however not recommended unless the symptoms are severe and life threatening, as blunting the cytokine response can in turn negate T-cell proliferation. Elevated serum Ferritin and C-reactive protein levels are surrogate markers for severe Cytokine Release Syndrome. The CAR T-cells have been shown to also access sanctuary sites such as the central nervous system and eradicate cancer cells. CD19 antigen is expressed by majority of the B cell malignancies and therefore most studies using CAR T-cell therapy have focused on the treatment of advanced B-cell malignancies such as Chronic Lymphocytic Leukemia (CLL), Acute Lymphoblastic Leukemia (ALL) and Non Hodgkin lymphoma (NHL), such as Diffuse Large B-Cell Lymphoma (DLBCL). Previously published studies have shown significant responses with CAR T-cell therapy in patients with relapsed and refractory B-cell ALL. But the durability of remission has remained unclear.
The authors in this study, treated a total of 30 patients with relapsed or refractory ALL ( included those who had relapsed after allogeneic stem cell transplantation and those refractory to CD19 directed bispecific antibody Blinatumomab), with autologous Chimeric Antigen Receptor (CAR) T-cells (CTL019 T-cells) and monitored response rates, toxicities as well as proliferation and persistence of circulating CTL019 T-cells in the patient’s body. The first assessment was performed 1 month after infusion of CTL019 and 90% of the patients were in complete remission and sustained remissions were noted for up to 2 years. At a median follow up of 6 months, the event free survival was 67% and overall survival was 78%. The authors compared this efficacy data with the FDA approved agents for relapsed ALL such as Clofarabine, Nelarabine and Liposomal encapsulated Vincristine, which have a complete remission of less than 25% with a median duration of response of 4-9 weeks. Persisting CTL019 T-cells in the body is a marker of therapeutic efficacy. CTL019 T-cells proliferated in the patient’s body and was detectable in the blood bone marrow, and cerebrospinal fluid of patients who had a response. At 6 months, the probability that a patient would have persistence of CTL019 T-cells was 68% and the probability that a patient would have relapse free B-cell aplasia was 73%. Severe Cytokine Release Syndrome was noted in 27% of the patients and these patients had a higher disease burden before CTL019 infusion. All of these patients were effectively treated with the Interleukin-6 receptor blocking antibody Tocilizumab. The authors concluded that Chimeric Antigen Receptor modified T-cell therapy against CD19 positive cells (CTL019) was highly efficacious, in patients with relapsed and refractory ALL and was associated with a high and durable remission rate. This technology may be applied to other malignancies, as new antigen targets are identified. Maude SL, Frey N, Shaw PA, et al. N Engl J Med 2014; 371:1507-1517
Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody, Blinatumomab in patients (pts) with relapsed/refractory B-precursor acute lymphoblastic leukemia (r/r ALL).
SUMMARY: The FDA in July 2014, granted Breakthrough Therapy Designation to Blinatumomab, a bispecific T cell engager (BiTE) antibody, for adults with Philadelphia-negative (Ph-) Relapsed/Refractory B-precursor Acute Lymphoblastic Leukemia (ALL). BiTE® technology engages the body's immune system to detect and target malignant cells. These modified antibodies are designed to engage two different targets simultaneously, thereby placing the T cells within reach of the targeted cancer cell and facilitating apoptosis of the cancer cell. BiTE antibodies are currently being investigated to treat a wide variety of malignancies. Blinatumomab is an investigational BiTE® antibody designed to direct the patients T cells against CD19, a protein found on the surface of B-cell derived leukemias and lymphomas.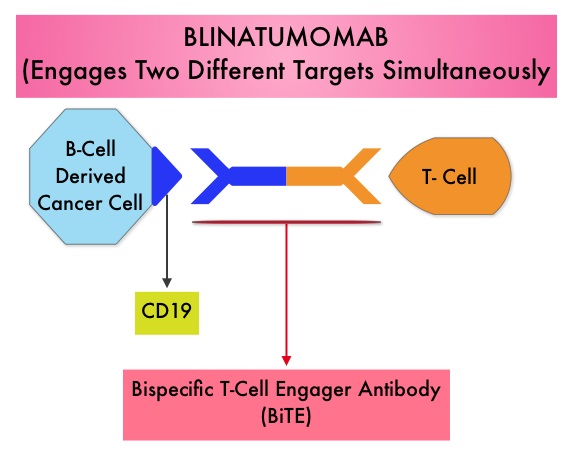 The Breakthrough Therapy Designation to Blinatumomab was based on a Phase II study in which 189 patients with Philadelphia chromosome negative ALL were enrolled. The median age was 39 years, and patients had their 1st relapse and were refractory to post hematopoietic stem cell transplantation less than 12 months before. About a third of the patients had at least 2 salvage therapies. Blinatumomab was given by continuous IV infusion, 4 weeks on and 2 weeks off for up to 5 cycles and the median number of cycles given were 2. The primary endpoint was complete remission (CR) or CR with partial hematological recovery (CRh) within the first 2 cycles of treatment. At the time of primary analysis, 43% of patients achieved a CR or CRh and 80% of responses occurred within cycle 1. Further, the Complete Remissions (CR) and CR with partial hematological recovery (CRh) were seen in all subgroups of patients, although this was more pronounced in those with less than 50% bone marrow blasts. The median Relapse Free Survival and Overall survival were 5.9 months and 6.1 months respectively. The most frequent grade 3 adverse events were febrile neutropenia, neutropenia, and anemia, occurring in 26%, 15%, and 15% of patients, respectively. The authors concluded that Blinatumomab has significant single agent antileukemia activity in a difficult-to-treat population with Relapsed and Refractory Acute Lymphoblastic Leukemia. Clinical trials will hopefully address whether Blinatumomab can serve as a bridge to transplantation, in patients with Relapsed and Refractory B-cell ALL. Topp MS, Goekbuget N, Stein AS, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7005)
The Breakthrough Therapy Designation to Blinatumomab was based on a Phase II study in which 189 patients with Philadelphia chromosome negative ALL were enrolled. The median age was 39 years, and patients had their 1st relapse and were refractory to post hematopoietic stem cell transplantation less than 12 months before. About a third of the patients had at least 2 salvage therapies. Blinatumomab was given by continuous IV infusion, 4 weeks on and 2 weeks off for up to 5 cycles and the median number of cycles given were 2. The primary endpoint was complete remission (CR) or CR with partial hematological recovery (CRh) within the first 2 cycles of treatment. At the time of primary analysis, 43% of patients achieved a CR or CRh and 80% of responses occurred within cycle 1. Further, the Complete Remissions (CR) and CR with partial hematological recovery (CRh) were seen in all subgroups of patients, although this was more pronounced in those with less than 50% bone marrow blasts. The median Relapse Free Survival and Overall survival were 5.9 months and 6.1 months respectively. The most frequent grade 3 adverse events were febrile neutropenia, neutropenia, and anemia, occurring in 26%, 15%, and 15% of patients, respectively. The authors concluded that Blinatumomab has significant single agent antileukemia activity in a difficult-to-treat population with Relapsed and Refractory Acute Lymphoblastic Leukemia. Clinical trials will hopefully address whether Blinatumomab can serve as a bridge to transplantation, in patients with Relapsed and Refractory B-cell ALL. Topp MS, Goekbuget N, Stein AS, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7005)
Outcomes after Induction Failure in Childhood Acute Lymphoblastic Leukemia
SUMMARY: In children and adolescents with acute lymphoblastic leukemia (ALL), allogeneic stem cell transplantation is usually considered the treatment option, after failure of remission-induction therapy. In their review of over 44,000 cases of pediatric ALL in three continents, the authors noted that patients with B-cell ALL had better outcomes when treated with a second round of chemotherapy without a transplant. Patients with T-cell ALL however were noted to have a better outcome with transplantation. This review suggests that induction failure in patients with ALL does not automatically warrant transplantation. Schrappe M, Hunger SP, Pui C, et al. N Engl J Med 2012; 366:1371-1381